
Abstract
The COVID-19 pandemic caused by the severe acute respiratory syndrome (SARS)-CoV-2 infection is a systemic disease and a major planetary health burden. While SARS-CoV-2 impacts host biology extensively, our knowledge of these alterations from a systems perspective remains incomplete. Moreover, there is currently only a limited description of this systemic disease. For precision diagnosis and treatment of SARS-CoV-2, multiomics technologies and systems science research offer significant prospects. This expert review offers a critical analysis of the prospects and challenges of the emerging mass spectrometry-based proteomics approaches to the study of COVID-19 as seen through a systems medicine lens. We also discuss the ways in which proteomics is poised to offer hope for diagnostics and therapeutics innovation on SARS-CoV-2 infection as the disease transitions from a pandemic to an endemic disease, and thus further challenging the health systems and services worldwide in the coming decade. Proteomics is an important high-throughput technology platform to achieve a functional overview of the ways in which COVID-19 changes host biology, and hence, can help identify possible points of entry for innovation in medicines and vaccines, among others.
Introduction
Coronaviruses produce disease in many organisms. Previously, human respiratory disease has resulted from severe acute respiratory syndrome (SARS)-CoV and Middle East respiratory syndrome-CoV infections. Recently, the novel coronavirus, SARS-CoV-2, was identified as the causative agent of a potentially lethal respiratory disease of global public health concern (Cui et al., 2019; Hui et al., 2020; Wu et al., 2020b).
In December 2019, the COVID-19 infection broke out in Wuhan, China, and spread rapidly worldwide (Guan et al., 2020b; Huang et al., 2020). Given the global prevalence of this disease, the World Health Organization (WHO) has identified it as a pandemic public health threat and has considered any research in this field supportive (Deng and Peng, 2020). A growing body of evidence has suggested that COVID-19 can be transmitted between people through aerosols and close contact with a patient affected with COVID-19 (Han et al., 2020; Zhu et al., 2020).
So far, there is no specific drug against COVID-19. However, a limited number of vaccines have been designed in different countries that are currently undergoing an international rollout. Available antiviral drugs and respiratory-related therapies are applied as supportive therapy to alleviate the symptoms (Gralinski and Menachery, 2020; Hui et al., 2020). The most common symptoms of a COVID-19 infection include fever, dry cough, tiredness, and shortness of breath (Hui et al., 2020; Wu et al., 2020a).
Studies of proteomics and proteins have been recently identified and suggested as potential diagnostic and prognosis biomarkers as well as drug targets in COVID-19. Therefore, we conducted this review to reassess proteomics studies on COVID-19, which can serve a helpful approach in this area and provide new insights for developing novel therapies for COVID-19 management. A high-level overview of proteomics methods in the study of COVID-19 is depicted in Figure 1.
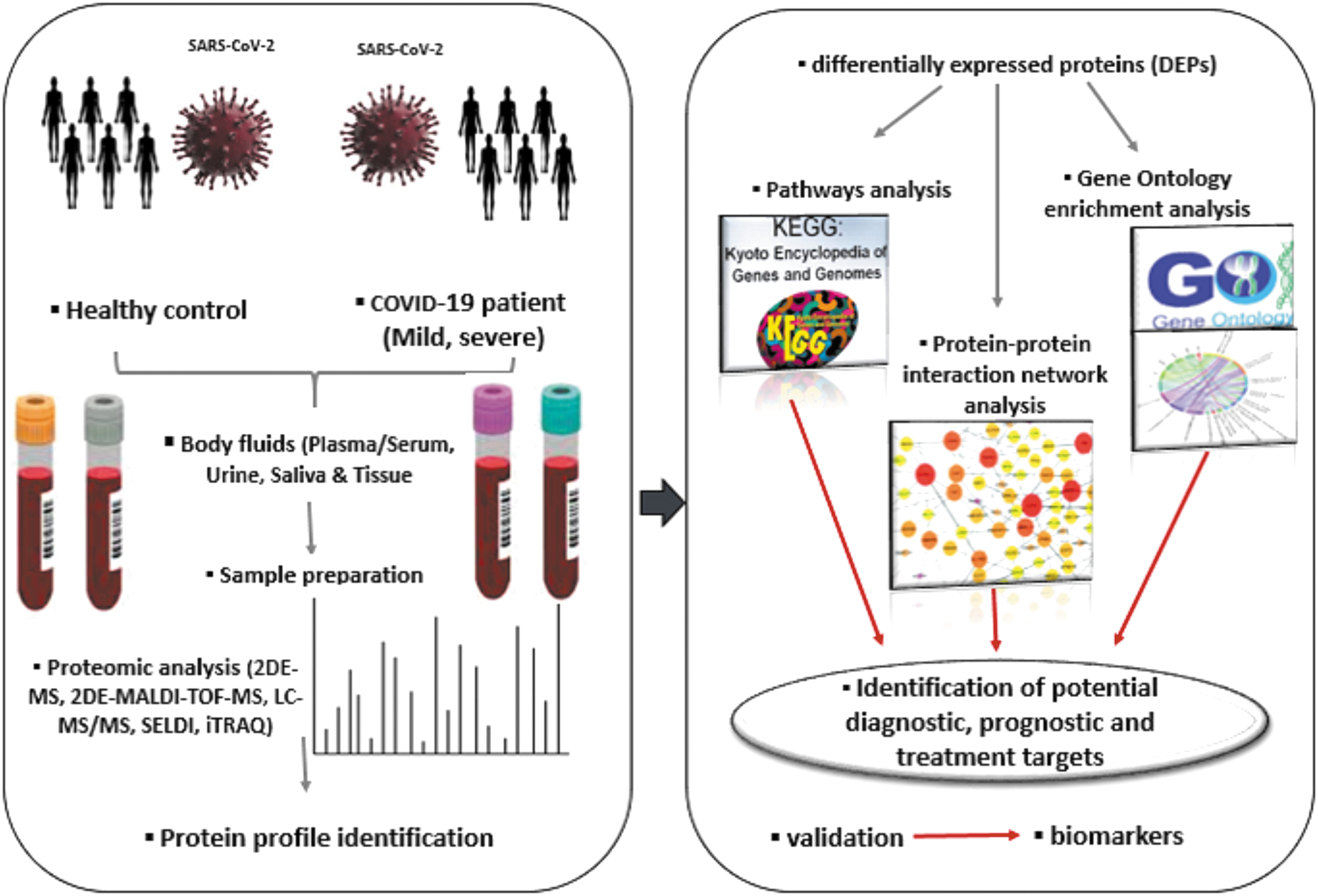
Overview of the proteomics technology in the study of COVID-19 disease to identify potential biomarkers. 2DE-MS, two-dimensional electrophoresis mass spectrometry; iTRAQ, isobaric tags for relative and absolute quantitation; LC-MS/MS, liquid chromatography coupled to tandem mass spectrometry; MALDI-TOF-MS, matrix assisted laser desorption ionization-time of flight mass spectrometry; SELDI, surface-enhanced laser desorption/ionization.
Roles of Proteomics in Infectious Diseases Research
Concerning the vital role of the proteomic approach in analyzing a set of proteins involved in the biological processes inside the cell, this technique plays a critical role in understanding disease phenotypes, explaining pathological mechanisms, and logical drug discovery (Ideker et al., 2001; Petricoin and Liotta, 2003). In recent years, proteomics, as an important component of systems biology, has attracted researchers' attention for medical diagnosis, drug development, and the study of pathogenic mechanisms of different diseases, especially infectious diseases (Liotta and Petricoin, 2000).
The use of proteomics technology in the study of various aspects of infectious diseases worldwide is relatively new, and recently this technique has been used in the study of COVID-19 disease. Proteomics is an important research tool in which different protein expressions are measured in different samples, including blood, urine, cells, and tissues in diseases. Studying cells under external stimuli is also possible using this modern technique, such as a virus entering a cell.
Various proteomics approaches have been used for protein identification, including gel-based methods, protein microarrays, and mass spectrometry (MS)-based approaches. The most common gel-based technique utilized in proteomics is two-dimensional gel electrophoresis (2DE). Unlike gel-based techniques, most MS-based proteomics approaches rely on initial protease-assisted digestion of proteins followed by protein quantification (Parker and Borchers, 2014). There are two main MS-based procedures, including “top-down” and “bottom-up” or “shotgun” proteomics. In the first approach, the intact proteins are analyzed directly using MS, which is preferable to peptide-based methods to study the molecular composition.
“Bottom-up” proteomics analysis relies on the characterization of proteins by analyzing peptides generated by proteolytic methods on the protein (Zhang et al., 2013). Proteomics has been extensively applied in infectious diseases research field, and different proteins are present in several types of infectious diseases, including parasitic and viral infectious diseases such as leishmaniasis (Amiri-Dashatan et al., 2018, 2020), dengue fever (Dwivedi et al., 2017; Perera and Kuhn, 2008), SARS-CoV (Kang et al., 2005; Poon et al., 2009), and SARS-CoV-2 (Bojkova et al., 2020; Prates et al., 2021).
The study of the proteome of the SARS-CoV-2 and COVID-19 by proteomics could be beneficial in discovering the main target proteins as candidates for effective drug and vaccine development. As in previous years, proteomics technology identified and described proteins and antigenic proteins of the SARS-CoV and introduced the angiotensin-converting enzyme-2 (ACE2) protein as the main receptor for SARA-CoV-2 in humans (Li et al., 2003; Ying et al., 2004). Since SARS-CoV-2, like other RNA viruses, disrupts cellular homeostasis after entering the cell, proteomics has made it possible to study the effects of the virus on human cells.
Proteomics studies resulting from SARS-CoV-2 and COVID-19 are classified into several categories as follows: (1) the identification of the SARS-CoV-2-host protein interactome; (2) proteomics profiling of SARS-CoV-2-infected human cells; (3) comparative proteomic profiling of infected cells versus normal cells; and (4) clinical proteomics of COVID-19-positive patients. Therefore, proteomics is a valuable tool for diagnosis, biomarker discovery, and drug and vaccine development for COVID-19 disease.
Overview of COVID-19
Like SARS-CoV, COVID-19 is also associated with fever symptoms, body aches, dry cough, and shortness of breath in severe cases. The rate of transmission of COVID-19 is very high, and people of all ages are at risk. SARS-CoV-2 is transmitted through aerosol droplets between people. Therefore, close contact with humans with COVID-19 can result in transmission. Sometimes, there is a possibility of spreading in closed areas because of the high concentration of aerosols (Anjorin, 2020). However, there are other ways of transmission, including transmission through contaminated surfaces by SARS-CoV-2. It is detected on the surfaces where people are in daily contact and can survive for 6 to 9 days in uninfected areas (Marquès and Domingo, 2020).
The clinical features of this disease are very different from those of asymptomatic septic shock and organ dysfunction. This disease is classified into mild, moderate, severe, and lethal types based on its severity (He et al., 2020). According to studies, about 80% of the disease is mild and critical (Padron-Regalado, 2020). Patients with severe infections show symptoms such as respiratory distress syndrome and septic shock (Mehta et al., 2020).
Patients with underlying comorbidities (e.g., diabetes, cardiovascular disease, respiratory disease, or cancer) are at higher risk of severe forms of COVID-19 and thus higher mortality rates (George and George, 2020). The most common methods of diagnosing the disease include evaluating samples for the viral RNA using reverse transcription-polymerase chain reaction (RT-PCR) and the chest computed tomography (CT) imaging method in patients with a poor molecular diagnosis (Ahn et al., 2020).
In addition, immunological-based methods, including serologic and antigen tests, are used for COVID-19 diagnosis. In serologic tests, three types of antibodies are evaluated: immunoglobulin M (IgM), immunoglobulin G (IgG), and immunoglobulin A (IgA). COVID-19 antigen tests are the second type of immunologic assay that can be used for COVID-19 detection. The principle of this test is based on identifying viral antigens so that it can diagnose a current infection and not past infections (Shaffaf and Ghafar-Zadeh, 2021). To date, there is no specific treatment for this ailment. The primary treatment for this disease is based on antiviral drugs and respiratory therapies. Treatment options using monoclonal antibodies (Taylor et al., 2021) and cell therapy (Choudhery and Harris, 2020) are also being studied.
Symptomatic patients who are suspected of having COVID-19 should self-quarantine (Escher, 2020; Kumar and Agarwal, 2020). The rapid and alarming spread of COVID-19 disease worldwide has challenged all sections of society. The disease is a serious threat to public health and has infected about 252,796,512 people and caused >5 million deaths (as of November 11, 2021) worldwide. There is no specific drug to deal with, and the essential action is the self-protection of people with hygiene items and materials. Initially, during the early stages of COVID-19 infection, severe acute respiratory infection develops into acute respiratory distress syndrome (ARDS) in some patients and even multiorgan dysfunction (Li et al., 2020b).
COVID-19 Pathogenesis
Due to SARS-CoV and SARS-CoV-2 similarity, the molecular mechanisms of COVID-19 pathogenesis are possibly similar. Hyperinflammation has been raised as the significant reason for the previously confirmed disease severity in SARS-CoV (Mehta et al., 2020). Although details of the cellular processes of SARS-CoV-2 are unknown, a possible sequence of events can be proposed according to previous investigations into SARS-CoV. Three phases were postulated for COVID-19 infection based on infected cell types and clinical stages of the disease (Wu and McGoogan, 2020).
Asymptomatic Phase
Initially, the inhaled novel coronaviruses enter the epithelial cells of the airways and replicate in these cells. Because ACE2 was a major receptor of SARS-CoV, SARS-CoV-2 binds to ACE2 to enter host cells (Wan et al., 2020). In this regard, the SARS-CoV-2 enters the cell through the interaction between transmembrane spike (S) glycoprotein and the N-terminal segment of the ACE2 host cell membrane enzyme (Walls et al., 2020). Asymptomatic carriers that can only be identified by the virus's RNA diagnostic test of nasal swabs do not have any symptoms, including fever, body pain, gastrointestinal, or respiratory symptoms (Mason, 2020). In addition, no significant abnormalities can be seen in their chest radiograph. However, the transmission of the virus through asymptomatic cases has been reported in many recent studies (Bai et al., 2020). Although the virus is a local propagation, a limited innate immune response occurs at this stage (Mason, 2020).
ARD Stage (Upper Airway)
Acute respiratory distress (ARD) describes as laboratory-confirmed COVID-19, with respiratory symptoms and chest CT without signs of pneumonia (Guan et al., 2020a). At this stage of infection, the SARS-CoV-2 pervades and migrates to the respiratory tract, triggering a stronger innate immune response. Both the virus and primitive markers of the innate immune system response are recognizable in this phase of the disease (Tang et al., 2005).
There is currently limited knowledge about the innate immune response against COVID-19. Various studies, for example, found an increase in total neutrophil cells and a decrease in total lymphocyte count to be closely related to COVID-19 severity (Schultze and Aschenbrenner, 2021). In addition, in patients with COVID-19, there is also evidence of increased plasma concentrations of innate cytokines such as IP-1, MCP-1, and TNF-α (Schultze and Aschenbrenner, 2021). The epithelial cells which SARS-CoV-2 infects are the main source of interferon.
The effective innate immune response to infection is closely dependent on IFNT1 and its downstream signaling cascade, leading to virus replication inhibition and finally stimulating an adaptive immune response (Prompetchara et al., 2020). Interferon especially limits the virus's spread and has an immunomodulatory role in elevating the macrophage phagocytosis of antigens (Huang et al., 2019). These responses are the first line of defense against the SARS-CoV-2 at the site of entry. Measurement of the host's innate immune response to the coronavirus may aid in predicting subsequent stages of infection and improving patient care methods. Since the innate immune response plays an important protective role in disease and is an efficient factor in the outcome prediction of the disease, IFNT1 antagonists could be potential and valuable antiviral drugs.
Acute Respiratory Distress Syndrome (Pneumonia)
The COVID-19 cases with pneumonia had both respiratory symptoms and pneumonia signs on their chest radiographs. Approximately 20% of COVID-19 patients will develop pulmonary infiltrates, some of which will experience severe disease. At this stage, the SARS-CoV-2 infects alveolar cells of type II (Wu and McGoogan, 2020). Although all body organs express ACE2, alveolar cells express high amounts of this receptor (Sungnak et al., 2020). As SARS-CoV spreads within type II cells, many viral particles are released, and the cells suffer from apoptosis (Qian et al., 2013).
Recent investigations have suggested that the cytokine storm is one of the major mechanisms of ARDS and multiple organ disorders in COVID-19 patients (Channappanavar and Perlman, 2017). Generally, the inflammation response contributes to COVID-19 pathogenesis, while hyperinflammation and cytokine storm have a crucial role in disease severity.
ARDS leads to diffuse alveolar injury in the lung. Hyaline membrane formation occurs in the alveoli in the acute phase, followed by edema and fibroblast proliferation (Tian et al., 2020), diffuse alveolar injury in COVID-19, and induces ARDS. Coagulation dysfunction is a common event in COVID-19 and is determined by increased D-dimer expression levels (Wang et al., 2020). Most death cases from COVID-19-ARDS have signs of thrombotic disseminated intravascular coagulation (Asakura and Ogawa, 2021).
Proteomic Studies on COVID-19
New technologies such as proteomics in medical research have created new opportunities in identifying biomarkers for the diagnosis, prognosis, and treatment of diseases. Proteomics has also emerged as a new application in the study of infectious diseases, particularly COVID-19. The current review emphasizes different proteomic methods currently utilized to decipher novel drug targets and potential biomarkers for SARS-CoV-2 and COVID-19. The most applied technique includes liquid chromatography coupled with MS. Protein identifications from body fluids, including serum, plasma, urine, and other biospecimens, have been made in COVID-19 patients (Fraser et al., 2020; Nie et al., 2021).
Most of the investigations in the field of COVID-19 proteomics have been performed on serum/plasma samples (D'Alessandro et al., 2020; Fraser et al., 2020; Messner et al., 2020; Park et al., 2020; Shen et al., 2020; Shu et al., 2020), while there are only limited studies on urine and tissues (Nie et al., 2021; Qiu et al., 2020; Wendt et al., 2020). In addition, two studies have used cell lysates of infected cells with SARS-CoV-2 to identify host cell pathways and biological processes modulated by the virus (Bojkova et al., 2020; Grenga et al., 2020). An overview of the selected proteomics studies of SARS-CoV-2 and COVID-19 is presented in Table 1.
The Recent Proteomic Research in a SARS-CoV-2 Context
ACE2, angiotensin-converting enzyme-2; AKI, acute kidney injury; CRP, C-reactive protein; DEPs, differently expressed proteins; ELISA, Enzyme-Linked Immunosorbent Assay; FDR, false discovery rate; ICU, intensive care unit; IL, interleukin; KEGG, Kyoto Encyclopedia of Genes and Genomes; LC-MS/MS, liquid chromatography coupled to tandem mass spectrometry; MRM-HR, multiple reaction monitoring-high resolution; SARS, severe acute respiratory syndrome; SWATH-MS, Sequential Window Acquisition of all Theoretical Mass Spectra; UPLC-MS/MS, Ultra-Performance Liquid Chromatography–Mass Spectrometry; WHO, World Health Organization.
Boldface = potential biomarkers.
Serum Proteomic Signatures of COVID-19
MS-based proteomics is gradually becoming a valuable analytical tool in searching for novel biomarkers that could be conducive to determining diagnostic, prognostic, and potential drug targets for various pathological conditions. Recently, the identification and characterization of disease progression based on liquid biopsies such as serum or plasma are particularly encouraging since proteomic profiling of serum or plasma displays systemic changes during cellular dysfunction.
Shen et al. (2020) performed an ultra-performance liquid chromatography–MS/MS (UPLC-MS/MS) approach for proteomic and metabolomic profiling of 46 COVID-19 serums compared with 53 control individuals. This research group hypothesized that SARS-CoV-2 altered the molecular characteristics of patients. The detection of these molecular changes may help to develop an effective treatment for COVID-19 patients.
They introduced 93 and 204 proteins and metabolites with different expressions in the sera of severe COVID-19 patients, respectively, which correlate with disease severity. They performed a machine learning model using proteomics and metabolomics results from nonsevere and severe patients. They verified the trained model with targeted proteomics (MRM-HR) and metabolomics assays (Shen et al., 2020). Their results showed that dysregulation of macrophages, platelet degranulation, complement system pathways, and massive metabolic suppression are the most important molecular alterations in the sera of COVID-19 patients compared with other groups, which could be used for severity evaluation of COVID-19 using potential biomarkers (Shen et al., 2020).
As the results of studies in COVID-19 patients have shown, the expression level of proinflammatory cytokines is higher in these patients (Chen et al., 2020b). There is also evidence that the interleukin-6 (IL-6) level is associated with disease severity (Lingeswaran et al., 2020). Despite this information, the effect of the IL-6 cytokine on the proteomic profile of patients with COVID-19 has not been explained.
In a recent study, D'Alessandro et al. (2020) investigated the serum proteomic analysis of 16 control groups and 33 COVID-19-positive patients classified by circulating level of IL-6 by Nano Ultra-HPLC-MS/MS. They reported an increased level of inhibitory components of the fibrinolytic cascade, including several SERPINs in severe patients correlated with coagulopathic complications in COVID-19. In addition, sera of COVID-19 patients with the highest IL-6 levels exhibited increased protein markers of hemolysis, including HBA, HBB, and CA1.
Finally, they proposed changing coagulation and complement status as a function of the IL-6 level (D'Alessandro et al., 2020). These results can provide the basis for the proper use of therapeutic interventions in patients with higher severity. Furthermore, Fraser et al. (2020) performed targeted proteomics on 10 COVID-19 patients admitted to the intensive care unit (ICU) and 10 age- and sex-matched healthy control subjects to clarify pathogenesis and potential outcome markers.
Their data showed the six main proteins in the unique plasma proteome of COVID-19 patients predicted ICU survival and mortality with 100% accuracy. Furthermore, their findings suggest that these six proteins (CLM-1, IL12RB1, CD83, FAM3B, IGF1R, and OPTC) should be investigated further as potential biomarkers for disease severity (Fraser et al., 2020).
In another study, Park et al. (2020) also investigated candidate biomarkers for evaluating disease severity. They compared the plasma protein profiles of three mild COVID-19 patients to those of five severe subjects, utilizing a label-free quantitative proteomics approach (Park et al., 2020). They identified 91 different expressed plasma proteins between the mild and severe groups of COVID-19. Then they identified 76 novels, previously unreported proteins, which could be new potential prognostic biomarkers (Park et al., 2020).
Their results indicated that the main host responses to SARS-CoV-2 infection included neutrophil activation, complement activation, platelet function, and T cell suppression. In addition, further bioinformatics analysis suggested a high specificity of several inflammatory factors, particularly IL-6, IL-1, and TNF-α (Park et al., 2020). Despite limitations such as the small number of samples examined by this group, the results obtained may provide a window into the expansion of prognostic biomarkers and therapeutic target candidates.
In addition, Messner et al. (2020) looked at the plasma/serum proteome as a source of protein expression signatures in 31 COVID-19-positive patients with varying severity. They aimed to determine the protein expression profiles of patients to classify COVID-19 patients according to WHO grading. They applied ultra-high-throughput platform analysis and identified 37 protein groups with either increased or decreased levels, depending on the disease severity (Messner et al., 2020). Then, they confirmed 27 potential biomarkers that are differentially expressed depending on the WHO severity grade of COVID-19 in an independent study (A1BG, ACTB, ACTG1, ALB, APOA1, APOC1, C1R, C1S, C8A, CD14, CFB, CFH, CFI, CRP, FGA, FGB, FGG, GSN, HP, ITIH3, ITIH4, LBP, LGALS3BP, LRG1, SAA1, SAA2, and SERPINA10).
Studies have shown that IL-6 is one of the most important proinflammatory markers in this disease. According to some studies, its expression is related to the severity of the disease (Lingeswaran et al., 2020; Yoshikawa et al., 2009). Messner et al. (2020) also reported some proteins involved in the IL-6 signaling pathway. This included proteins related to activation of the classical complement pathway, including C1R, C1S, and C8A, and also the alternative pathway factor B (CFB) and the complement modulators: factors I (CFI) and H (CFH).
Another upregulated protein was C-reactive protein (CRP), a component of acute-phase reactants and serum amyloid proteins, SAA1 and SAA2. Other studies have reported that cytokine storm plays a critical role in the COVID-19 infection severity (Klausegger et al., 1999). CRP as an acute-phase protein is proposed as an early predictor of inflammation or infection. In addition, the serum level of CRP is routinely determined in the early diagnosis of pneumonia (Warusevitane et al., 2016), and several publications have suggested the prognostic value of CRP (Liu et al., 2020). Increased levels of CRP were reported in up to 86% of COVID-19 patients in severe grade (Guan et al., 2020b).
Several studies reported a high concentration of CRP in severe cases compared with the mild group. For example, in a study, the mean concentration of CRP was reported as 46 and 23 mg/L in severe and nonsevere patients, respectively (Mo et al., 2020). Ahnach et al. (2020) also introduced CRP as an early predictor of COVID-19 severity.
Some of the studies explore the significance of SAA in evaluating the severity and prognosis of COVID-19. SSA is usually used as an inflammation indicator in clinics. According to studies in the field of COVID-19 infection, an increased level of SAA correlated with the severity of the disease (Yu et al., 2020). Li et al. (2020a) investigated predictive biomarkers to evaluate the severity and prognosis of COVID-19 and observed that COVID-19 patients had significantly elevated SAA and CRP levels. They suggested that SAA is valuable in assessing the severity of COVID-19 and distinguishing critically severe patients from mild ones (Li et al., 2020a).
Moreover, Shu et al. (2020), compared host plasma proteome alteration in response to SARS-CoV-2 infection in patients with fatal outcomes, patients with severe disease, and patients diagnosed as mild types using the LC-MS/MS method. They detected a total of 195 significant differently expressed proteins (Shu et al., 2020). Gene ontology and KEGG (Kyoto Encyclopedia of Genes and Genomes) pathway analyses identified inflammation, immune cell migration and degranulation, complement system, coagulation cascades, and energy metabolism as the most significantly enriched processes.
These results have been already observed in the studies of other researchers (Chen et al., 2020a; Huang et al., 2020). In the meantime, platelet degranulation and the complement and coagulation cascades were more frequently changed in the fatal and severe groups than in the mild group, indicating that this dysregulation process is closely associated with COVID-19 severity prediction.
In addition, two SARS-CoV-2-related proteins (including nsP2 and nsP7) were identified in the severe and fatal groups, indicating the important role of these two proteins in the pathogenesis mechanism of COVID-19. They also conducted a machine learning-based pipeline to discover 11 potential biomarkers. Then some of these biomarkers were validated by an Enzyme-Linked Immunosorbent Assay (ELISA) using a larger cohort (Shu et al., 2020). The efforts of this research group can be very valuable in better understanding the pathogenesis of the disease and introducing potential therapeutic targets.
Understanding the factors affecting the progression and severity of COVID-19 is one of the important challenges in the better management of this pandemic. To address this issue, Villar et al. (2021) conducted quantitative SWATH-MS (Sequential Window Acquisition of all Theoretical Mass Spectra) proteomics along with multiple data analysis algorithms to describe serum prognostic biomarkers for COVID-19 Symptomatology (Villar et al., 2021). A total of 189 proteins were detected in serum samples from all cohorts. Of them, 49, 113, 124, and 129 proteins were significantly dysregulated in asymptomatic, recovered, nonsevere, and severe cases when compared with healthy controls, respectively. The results are consistent with previous data in COVID-19 investigations and show that the differently expressed proteins, and related biological processes increase with COVID-19 disease symptomatology, from asymptomatic to severe cases.
Among the identified differently expressed proteins in various comparisons, coagulation factor XII (F12), carboxypeptidase B2 (CPB2), transmembrane protein 198 (TMEM198), ATP-binding cassette subfamily F member 1 (ABCF1), and pregnancy zone protein (PZP) were not identified in previous studies.
Of them, PZP was downregulated in the asymptomatic form of COVID-19, an immunosuppressive protein, which prevents fatal rejection by suppressing T cell function during pregnancy. Furthermore, overexpression of this protein has been linked to an increase in the severity of bronchiectasis infection (Finch et al., 2019). However, the expression value of PZP could be represented as a prognosis biomarker for COVID-19 severity and asymptomatic cases.
According to the literature, SELENOP levels associated with selenium status affect immunity and tissue homeostasis (Carlson et al., 2009; Huang et al., 2012), in which Villar et al. (2021) presented this protein as a biomarker for disease recovery. PON1 was found to play an important role in the prevention of obesity as well as in the protection against bacterial, parasitic, and viral infections (Farid and Horii, 2012). According to Villar et al. (2021), PON1 increased during the nonsevere progression into severe form and proposed as a recovery marker.
In addition, CPB2 was upregulated in all groups except asymptomatic COVID-19 patients in the above study. CCPB2 plays an important role in innate immunity through the inactivation of complement component C5a, which triggers inflammatory pathways (Leung and Morser, 2018; Merle et al., 2015). These proteins, which relate to the immune system, were verified using the ELISA test for disease recovery [Selenoprotein P (SELENOP) and serum paraoxonase/arylesterase 1 (PON1)], severity [Carboxypeptidase B2 (CPB2)], and symptomatology [Pregnancy Zone Protein (PZP)] using protein-specific ELISA tests (Villar et al., 2021).
In addition to serum proteomic study of COVID-19 patients compared with healthy individuals to introduce potential biomarkers, Yang et al. (2021) studied the proteomics analysis of COVID-19 complications in patients with pulmonary fibrosis. Pulmonary fibrosis was reported in patients with COVID-19 by CT imaging and autopsy (Xu et al., 2020). The only treatment for pulmonary fibrosis as a progressive lung disease is transplantation (George et al., 2019).
Several studies identified the Arg-Gly-Asp integrin-binding domain in the SARS-CoV-2 spike protein as a potential target pathway (Qiao and Olvera de la Cruz, 2020). Furthermore, the TGF-pathway is the primary antifibrotic therapeutic pathway (King et al., 2009). However, more of the molecular pathways of profibrotic pathology require exploration. In this regard, proteomics is a helpful technique to screen for disease-related biomarkers. Yang et al. (2021) used integrated proteomics and metabolomics methods and combined their results with chest CT imaging to explore the associated biological pathways of pulmonary fibrosis progression in COVID-19.
They found significant different expression of proteins related to the immune system, biological adhesion markers, and glycosaminoglycan degradation in pulmonary fibrosis patients. Previous investigations showed that glycosaminoglycan accumulation and its deposition in the extracellular matrix participated in pulmonary fibrosis progression (Li et al., 2016). It has been well demonstrated that the immune system plays a main role in developing fibrosis and COVID-19 (Song et al., 2020).
Although in Yang et al.'s (2021) study, FcR-mediated phagocytosis, peroxisome proliferator-activated receptor (PPAR) signaling, and transient receptor potential (TRP) inflammatory pathways were presented as related pathways of fibrosis formation and progression in COVID-19 patients, nevertheless, these results require validation in in vivo and in vitro experiments. These findings; however, offer novel treatment options for COVID-19 and fibrosis patients (Yang et al., 2021).
Urinary Proteomics Profiles of COVID-19
Assays of proteomics biomarkers in urine are noninvasive compared with other biofluids and can be easily repeated. The urine proteome profile is less complex than the serum/plasma and tissues but can contain potential biomarkers for the diagnosis and prognosis of various diseases, such as infectious diseases. In this regard, Li et al. (2020) evaluated the diagnostic roles of urine samples in the progression of mild-to-severe types of COVID-19 and the recovery state with cutting-edge urine proteomics (Li et al., 2020b). They used liquid chromatography coupled to tandem mass spectrometry (LC-MS/MS), and two technical repeats were applied to every sample.
To classify mild and severe disease in samples, the IL-6 index was used, which showed that in patients with severe disease, the stress response based on IL-6 expression level to viral infection was much higher than its standard level. They detected 2656, 1380, and 1641 proteins in 32 healthy controls, COVID-19, and two recovery patients, respectively. They observed 1008 common proteins among the healthy controls, COVID-19, and recovered patients.
On the other hand, they stated that 211 and 63 proteins were exclusively expressed in COVID-19 patients and recovery samples, respectively. They have not detected any SARS-CoV-2-associated proteins in the urine samples, which could be justified by the scarcity of virus proteins in the urine and the filtration of the kidneys (Li et al., 2020b). Clustering analysis showed that patients and healthy controls could be categorized into two groups. Also, the mild COVID-19 patients were clustered in a distinct cluster from the severe patient group. They used differently expressed proteins to characterize the molecular features of COVID-19 pathogenesis in mild, severe, and healthy groups.
In this way, they found 86 and 83 considerably upregulated and 100 and 172 significantly downregulated proteins in mild and severe COVID-19 patients, respectively (Li et al., 2020a). Gene ontology results showed that complement activation, regulation of immune response, cellular oxidant detoxification, cellular response to hypoxia, and oxidative stress-induced apoptosis play an essential role in COVID-19 disease pathogenesis and progression.
These results are consistent with previous proteomics studies performed on patients' serum (Li et al., 2020a). They found several potential biomarkers to distinguish between the mild and severe types of COVID-19, including the hypoxia upregulated protein 1 (HYOU1), heparin cofactor 2 (SERPIND1), and cyclic AMP-responsive element-binding protein 3-like protein 3 (CREB3L3). The HYOU1 protein is a heat shock protein that accumulates in the endoplasmic reticulum (ER) under hypoxic conditions. In addition, this protein plays a vital role in protein folding and secretion in the ER.
In addition, HYOU1 protein is associated with elevated apoptosis; however, it is a critical cytoprotective component in hypoxia-induced cellular perturbation (Shen et al., 2004). Heparin cofactor 2 (SERPIND1) is a serine proteinase inhibitor known as a thrombin inhibitor and the cofactor for heparin (He et al., 2002). This increase in expression of SERPIND1 may be due to a protective response to reduce the risk of intravascular coagulation reported in patients with COVID-19. CREB3L3 is another biomarker reported by Li et al. (2020), which is upregulated in mild and severe patients and can be a defense mechanism against COVID-19. In addition, this study found that intracellular cholesterol transporter 2 (NPC2), APOA1, and cubilin (CUBN) were downregulated in severe COVID-19 patients. These findings suggest that lipid metabolism and transport (as well as cholesterol homeostasis) were disrupted.
Another urine proteomic study in COVID-19 was done by Wendt et al. (2020). This study aimed to identify if urinary peptides were significantly associated with SARS-CoV-2 infection and develop a multimarker urinary peptide-based test, COVID-20, which may enable the prognosis of critical and fatal outcomes in COVID-19 patients. Finally, this research study (Wendt et al., 2020) identified 20 endogenous peptides, primarily derived from various collagen chains, capable of distinguishing moderate or severe disease from critical state or death with 83% sensitivity and 100% specificity.
Acute kidney injury (AKI) is a significant complication related to COVID-19 and occurs in up to 76% of patients with COVID-19 in the ICU. Using urinary proteomics is a practical approach to describing the proteins involved in kidney health and disease conditions. It provides a noninvasive method for assessing disease and monitoring response in patients with renal diseases (Kim et al., 2011). In this regard, Ye et al. (2021) conducted a pilot study of urine proteomics in COVID-19-associated AKI. They analyzed urine samples from 14 patients, including COVID-AKI (n = 6), COVID-no AKI (n = 3), and no COVID-no AKI (n = 5) (Ye et al., 2021).
This research group evaluated whether underlying variance could be distinguished between AKI positive and other samples without AKI. A significant increase in 97 proteins and a decrease in 140 proteins were detected in the AKI+ group. Furthermore, MB, CA1, MANSC domain-containing protein 1 (MANSC1), and ABRA C-Terminal-Like (ABRACL) proteins were detected with a significantly increased level in the COVID+ group compared with the COVID− group.
In addition, Granulin Precursor (GRN), CAMP Responsive Element-Binding Protein 3 Like-3 (CREB3L3), Mucin-1 (MUC1), CD320 antigen (CD320), and Dihydrolipoamide S-Succinyltransferase (DLST) were significantly decreased in COVID+. These newly identified proteins could provide potential biomarkers to assess the COVID-19 infection. The Gene Ontology and Pathway Enrichment analysis showed that complement activation, coagulation cascades, and regulated exocytosis were the most upregulated pathways between the compared groups. Enrichment results suggest decreased capacity to regulate complement activation, thereby damaging the intensifier. This finding is consistent with AKI exacerbation in mice with deleted CD55 after ischemia/reperfusion damage (Yamada et al., 2004). Taken together, their exciting data reveal the requirement for further studies with an expanded cohort.
Proteomics Analysis of Naso-Oropharyngeal Swab in COVID-19
Moreover, proteomics using Nano-LC-MS/MS of four COVID-19 by Akgun et al. (2020) identified molecular pathway alterations associated with the naso-oropharyngeal swab samples as the site of infection. They identified neutrophil elastase (ELANE), azurocidin (AZU1), myeloperoxidase (MPO), myeloblastin (PRTN3), cathepsin G (CTSG), and transcobalamin-1 (TCN1) as significantly altered proteins in naso-oropharyngeal samples of SARS-CoV-2 patients. These proteins are primarily associated with a change in the innate immune system through neutrophil degranulation and NETosis (Akgun et al., 2020).
Neutrophils play an essential role in infectious diseases and perform several functions during viral infections, including phagocytosis and degranulation (Camp and Jonsson, 2017). In addition, neutrophils' interactions with immune cells and releasing cytokines infer the antiviral response. Degranulation as an innate immune system component also participates in a defense mechanism against infection (Carrillo et al., 2017).
PRTN3 and MPO are expressed in the neutrophil granulocytes, which are involved in COVID-19 pathogenesis through activation of inflammatory cytokines and chlorine oxidant production, respectively (Klebanoff et al., 2013). The elevated PRTN3 and MPO expression levels in the neutrophils of patients with COVID-19 are the targets for antineutrophil antibodies. Increased PRTN3, on the other hand, has been shown to impede the elimination of inflammation, which leads to immune system dysregulation (Witko-Sarsat et al., 2010).
Proteomics Analysis of Tissue Samples from Patients with COVID-19
Multiorgan damages are a leading complication of a severe form of COVID-19. However, the molecular mechanism of multiorgan injuries in patients with COVID-19 remains unclear, preventing effective therapeutic development. Therefore, depicting quantitative proteomic profiling of host responses to fatal SARS-CoV-2 infection using postmortem tissues can help further our understanding of the molecular basis of COVID-19 pathology.
In this regard, two studies investigated postmortem tissue samples using proteomic methods (Nie et al., 2021; Qiu et al., 2020). Qiu et al. (2020) profiled the host response to SARS-CoV-2 infection using quantitative LC-MS/MS proteomics of eight different COVID-19 postmortem tissues, including lung, kidney, liver, intestine, brain, heart, muscle, and spleen. They observed that protein alterations in the lung tissue are commonly enriched in inflammation. At the same time, organ movement, respiration, and metabolism were the main processes enriched by altered protein expressed in other organs.
Based on these results, it can be concluded that lung damage occurs mainly due to a hyperinflammatory response to SARS-CoV-2 and intravascular thrombosis. However, other organ injury is due to hypoxia and organ dysfunction. In contrast, Nie et al. (2021) using LC-MS/MS global proteomics analysis of 144 autopsy samples from seven organs in 19 COVID-19 patients found that cathepsin L1, rather than ACE2, was considerably overexpressed in the lungs of COVID-19 patients. Excessive inflammation and disorders of glucose and fatty acid metabolism were observed in multiple organs. Additionally, dysregulation of key components in hypoxia, angiogenesis, blood coagulation, and fibrosis were detected in multiple organs of the COVID-19 patients (Nie et al., 2021).
Proteomics of SARS-CoV-2-Infected Host Cells
Because host cell pathways are altered after SARS-CoV-2 infection, identifying altered cellular pathways provides novel insights into potential drug targets and therapeutic development for COVID-19 treatment. To achieve these goals, several studies have investigated the proteomics of SARS-CoV-2-infected cells. In their study, Bojkova et al. (2020) identified dysregulated host cell pathways in SARS-CoV-2-infected cellular models. This analysis showed that SARS-CoV-2 reshapes fundamental biological processes, including translation, splicing, protein homeostasis, and nucleic acid metabolism.
Consistent with this result, the translation machinery severely affected SARS-CoV and other RNA viruses (Klann et al., 2020). Detection of host-modified pathways by the SARS-CoV-2 can identify new drug targets based on their behavior in the host cell and evaluate appropriate inhibitors. In other proteomics studies of infected cells by SARS-CoV-2, Grenga et al. detected 3220 host cells and 6 SARS-CoV-2 proteins (Grenga et al., 2020). Their analysis was consistent with the Bojkova et al. study. Details of proteomics investigations are provided in Table 1.
Hopes and Challenges from Proteomics Research on COVID-19
The SARA-CoV-2 epidemic has been the most important global infectious threat in the last century and has had far-reaching health, social, and economic consequences worldwide. It is believed that omics-based methods such as proteomics are able to provide help in this fight. In this review, we have tried to highlight the relevant studies in this field. Proteomics technology is a set of methods for studying biological systems. With the advent of COVID-19 disease, researchers in the field of proteomics have made significant advances, including understanding how the host cell system is hijacked by the virus, diagnosis, and predicting the severity of the disease.
In this regard, comparative proteomics in the study of patient and healthy individuals can help to better understand viral infections and provide information on more effective treatments. MS-based methods are suitable to study COVID-19 since they can detect differential expression of proteins and their post-translational modifications, and thus can represent inducers of pathological molecular mechanisms of disease.
Post-translational changes in the virus proteins lead to high complexity in the molecular system of the virus (Mahmud and Garrett, 2020). Given that the abundance of proteins, post-translational changes, and protein interactions together have not been fully identified in the virus, a full understanding of this global threat has not yet been established. Proteomics has the potential and ability to detect the virus more quickly through protein profiling with MS-based methods, as well as increasing disease information and predicting disease progression. Using MS-based methods integrated with multivariate analysis, researchers reported the ability of MS-based omics methods as a complementary diagnostic approach to discriminate SARS-CoV-2 from other coronaviruses.
Overall, various MS-based proteomics have presented potential as an important SARS-CoV-2 and COVID-19 investigation area. However, the expansion of powerful and more sensitive proteomics methods along with clinical trials and cohort studies are essential to demonstrate the promising insights of proteomics-based research in pandemics such as COVID-19.
Emerging virus samples, sample preparation and processing, and presenting of extraction techniques for MS-based approaches are challenging and mainly important. The limitation of proteomics in disease studying are: analysis complexity, absence of standard sample processing, low ability of this approach in the estimation of low abundance of proteins, and no validation of potential biomarkers in larger number of patients due to lack of antibodies. Another major challenge in use of proteomics in SARS-CoV-2 is the analysis of membrane proteins in virus particles. On the other hand, the most proteomics methods use complicated instrumentation, and expensive materials (Chandramouli and Qian, 2009).
One of the main challenges will be the integration of proteomics with other omics technologies such as transcriptomics, genomics, and metabolomics findings, as well as their practical interpretation in connection with clinical data and epidemiology. With all of these advantages and disadvantages, it is hoped that the data from proteomics research on the COVID-19 battlefield will be a very valuable resource for introducing promising therapeutic goals as well as identifying the molecular mechanisms undergoing expression after treatment. For a better and victorious confrontation against COVID-19, it is necessary to use a combination of omics (polyomics) methods.
Conclusions
Deciphering the molecular mechanism of SARS-CoV-2 is an essential aim of MS-based proteomics research to combat the COVID-19 pandemic. In the present review, we present all of the proteomics studies in the field of COVID-19 that can be useful in clarifying the various aspects of this infection. The use of proteomics methods identifies diagnostics, prognosis, and prediction of response to therapy. Additionally, the discovery of biomarkers and the study of molecular alterations by integrating analysis of proteomics with other “OMICs” platforms, including genomics, metabolomics, and lipidomics, along with bioinformatics analysis, will shed new light on the understanding of COVID-19 pathophysiology.
To conclude, proteomics technologies in the study of COVID-19 are in the early stages. They have not yet provided a validated biomarker, but it has opened up severe horizons in molecular pathogenesis, diagnosis methods, and delivery of therapeutic targets. Due to the complexity of the COVID-19 infection, a biomarker panel consisting of multiple protein markers will be helpful to differentiate between healthy and patient individuals, the initiation and progression of the infection to the severe form, predict the response to treatment, and ultimately create opportunities for new prophylactic and therapeutic interventions by clinicians.
Footnotes
Authors' Contributions
N.A.-D., M.K., and M.R.-T. designed the study. N.A.-D. and M.K. wrote the article. M.R.-T. edited the article. All authors made an important intellectual contribution, read, and approved the final version of the article.
Acknowledgment
The authors would like to thank the Proteomics Research Center, Shahid Beheshti University of Medical Sciences, for their support.
Author Disclosure Statement
The authors declare they have no conflicting financial interests.
Funding Information
No funding was received for this article.