
Abstract
Innovation roadmaps are important, because they encourage the actors in an innovation ecosystem to creatively imagine multiple possible science future(s), while anticipating the prospects and challenges on the innovation trajectory. In this overarching context, this expert review highlights the present unmet need for therapeutic innovations for pituitary neuroendocrine tumors (PitNETs), also known as pituitary adenomas. Although there are many drugs used in practice to treat PitNETs, many of these drugs can have negative side effects and show highly variable outcomes in terms of overall recovery. Building innovation roadmaps for PitNETs' treatments can allow incorporation of systems biology approaches to bring about insights at multiple levels of cell biology, from genes to proteins to metabolites. Using the systems biology techniques, it will then be possible to offer potential therapeutic strategies for the convergence of preventive approaches and patient-centered disease treatment. Here, we first provide a comprehensive overview of the molecular subtypes of PitNETs and therapeutics for these tumors from the past to the present. We then discuss examples of clinical trials and drug repositioning studies and how multi-omics studies can help in discovery and rational development of new therapeutics for PitNETs. Finally, this expert review offers new public health and personalized medicine approaches on cases that are refractory to conventional treatment or recur despite currently used surgical and/or drug therapy.
Introduction
Pituitary neuroendocrine tumors (PitNETs), also known as pituitary adenomas, are considered rare diseases, but their incidence is on the rise, contributing to mortality and morbidity in global health (Ostrom et al., 2020; Raverot et al., 2018; Trouillas et al., 2020).
PitNETs are classified into clinically functioning and nonfunctioning tumors (NF-PitNETs). Functioning tumors exhibit signs and symptoms of hormonal hypersecretion, such as somatotrophic PitNETs (growth hormone [GH]-secreting adenomas/acromegaly) due to elevated plasma levels of GH and/or insulin growth factor 1 (IGF-1). The lactotrophic PitNETs (prolactinomas or prolactin-secreting adenomas) associated with amenorrhea-galactorrhea or hypogonadism and the corticotrophic PitNETs (Cushing's syndrome/adenoma secreting adrenocorticotropic hormone [ACTH]-secreting adenoma) associated with hypercortisolism are also clinically noteworthy (Lopes, 2017; Trouillas et al., 2020).
NF-PitNETs generally do not exhibit signs and symptoms of endocrinopathies, with the exception of mild hyperprolactinemia due to compression of the pituitary stalk (Lopes, 2017; Trouillas et al., 2020). NF-PitNETs have subtypes according to the positivity of immunohistochemistry and expression of specific transcription factors. These subtypes are silent gonadotropic, silent thyrotropic, silent lactotropic, silent corticotropic, silent somatotropic, null cell, and plurihormonal Pit-1 positive tumors (Yavropoulou et al., 2020).
Aggressive pituitary tumors (APTs) and pituitary carcinomas (PCs) are the other types of pituitary neoplasms (Fig. 1). The dysfunctions caused by PitNETs are associated with various organs and tissues such as bones, ovaries, testes, or mammary glands (Fig. 2).
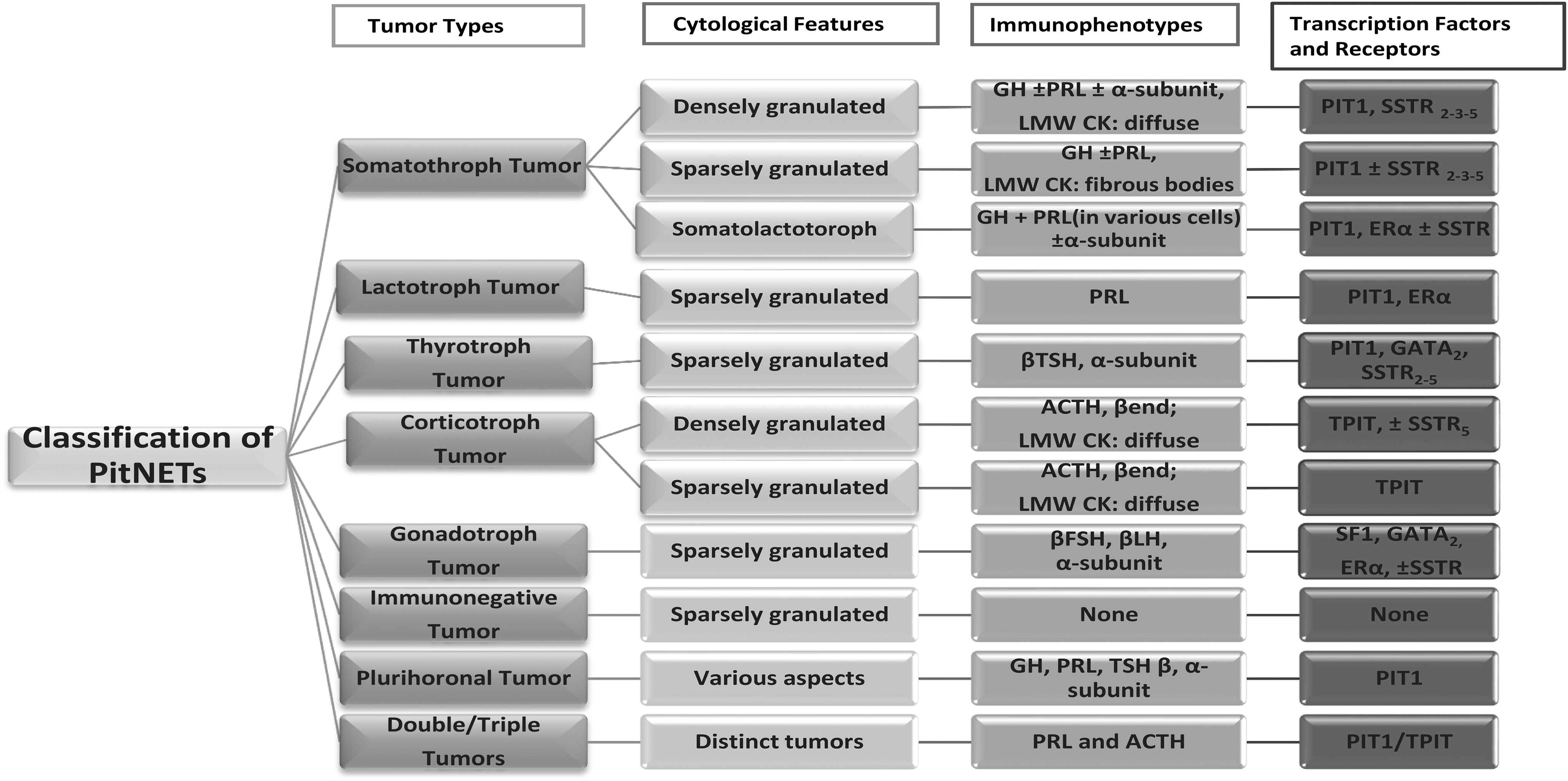
Classification of PitNETs. PitNETs, pituitary neuroendocrine tumors.
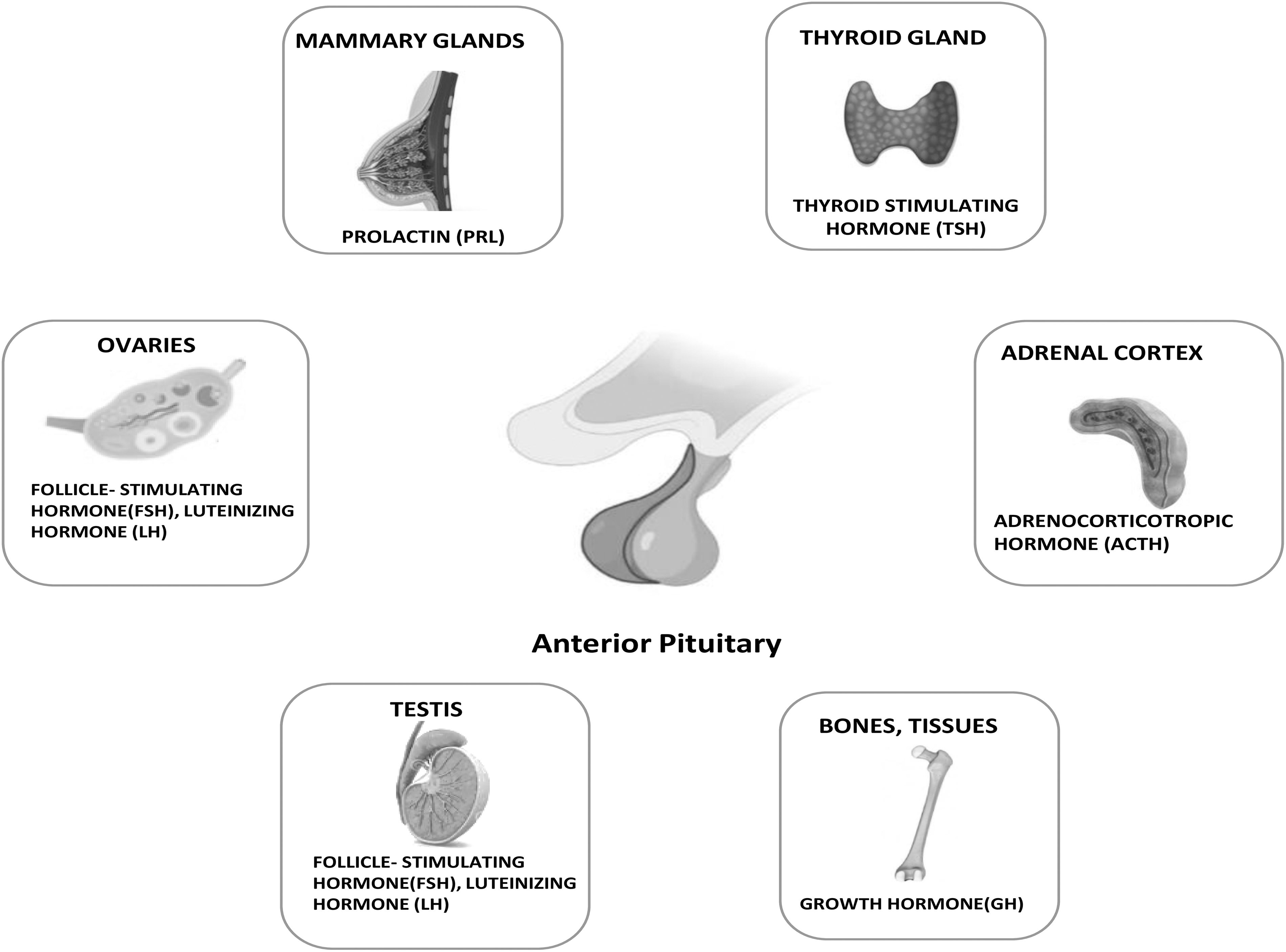
PitNET-associated organs and tissues.
There is an unmet need for innovative therapeutics for PitNETs. Systems biology approaches offer insights at multiple levels of cell biology in PitNETs from genes to proteins to metabolites. In addition, drug repositioning (DR) offers the prospect of leveraging drugs approved for clinical use outside of their indications and holds the exciting promise of accelerating drug discovery and development, especially when those drugs have already been evaluated for safety.
DR brings about new hope for cancer patients, as most noncancer drugs have a few or tolerable health side effects and have less impact on patients' quality of life (Frantzi et al., 2020; Würth et al., 2016). Therefore, a better understanding of the molecular pathogenesis of pituitary tumors will help to determine the applicability of such new approaches.
In this expert review, we first provide a comprehensive overview of the molecular subtypes of PitNETs and the therapeutics for these tumors from the past to the present. We then discuss some of the clinical trials and DR studies and discuss the ways in which multi-omics studies can aid in the discovery and development of novel therapeutics for PitNETs.
In addition, this article suggests that innovation roadmaps for PitNET treatment innovation are important because such roadmaps encourage the actors in an innovation ecosystem, be they academics, industry, governments, civil society organizations, to creatively imagine multiple possible science future(s), while anticipating the prospects and challenges on the innovation trajectory.
Therapeutics in Current Clinical Use for PitNETs
Because of the heterogeneity of PitNETs and the identification of different subtypes, a variety of therapeutic agents have been presented and used in clinical practice (Table 1). As expected, these agents showed variable efficacy and specificity in different subtypes.
Currently Used Therapeutics in the Clinic for the Treatment of Pituitary Neuroendocrine Tumors
DA, dopamine agonist; GH, growth hormone; LAR, long acting release; NF-PitNET, nonfunctioning pituitary neuroendocrine tumor; PD-1, programmed death-1; PitNET, pituitary neuroendocrine tumor; SSA, somatostatin analog; VEGF, vascular endothelial growth factor.
Somatotrophic PitNETs
Somatotrophic PitNETs are also known as GH-secreting adenomas. These tumors account for ∼20% of surgically treated PitNETs and more than 95% of acromegaly cases. Less than 5% of acromegaly cases are due to hypersecretion of GH-releasing hormone (Bano, 2020). The excessive release of GH causes the production of IGF-1 from the liver and other tissues (Melmed, 2006).
Currently available drug therapies to mitigate the effects of somatotrophic pituitary adenomas include dopamine agonists (DAs), somatostatin analogs (SSAs), and/or a GH receptor antagonist. Of the DAs, cabergoline currently offers the best efficacy for the clinical treatment of somatotroph adenomas. Treatment with cabergoline as a single agent provides biochemical control by normalizing serum IGF-1 levels in approximately one-third of patients with acromegaly (Sandret et al., 2011).
First-generation SSAs—long-acting-release (LAR) octreotide and lanreotide depot—overcome biochemical abnormalities in 20% to 35% of patients (Colao et al., 2014; Katznelson et al., 2014; Mercado et al., 2007; Salvatori et al., 2014). Treatment with octreotide LAR in patients with somatotrophic adenomas provides high efficacy in suppressing elevated IGF-1 levels and regressing tumor growth (Mercado et al., 2007). The inclusion of cabergoline in SSA therapy can show therapeutic effect in ∼50% of patients (Sandret et al., 2011).
Pasireotide has better efficacy potential in suppressing IGF-1 levels and achieving biochemical control of the disease compared with octreotide (Colao et al., 2014). The multiple side effects of SSAs are usually mild to moderate and consist of gallbladder stones and sludge, flatulence, abdominal cramps, and diarrhea (Katznelson et al., 2014; Racine and Barkan, 2002). Glucose tolerance abnormalities and diabetes have been observed in a large proportion of patients treated with pasireotide (Colao et al., 2014).
Pegvisomant is a recombinant GH receptor antagonist that has no direct antiproliferative effect on pituitary adenomas in patients with acromegaly. With the use of this GH receptor blocker, normalization of serum IGF-1 levels has been observed in ∼60% to 84% of patients in clinical practice (Muller et al., 2004; Van Der Lely et al., 2001). As an effective treatment option, a combination of pegvisomant and cabergoline may provide better control of IGF-1 levels in some patients with acromegaly (Bernabeu et al., 2013).
Pegvisomant can also be used in combination with long-acting SSAs (Neggers et al., 2011). These combination therapies allow for a reduction in pegvisomant doses and thus provide an economic advantage.
Thyrothrophic PitNETs
Thyrotrophic PitNETs are very rare tumors, accounting for less than 1% of all functioning pituitary adenomas (Daly et al., 2006; Gruppetta et al., 2013; Raappana et al., 2010; Tjörnstrand et al., 2014). Thyrotrophic PitNETs are characterized by a lack of thyroid-stimulating hormone (TSH) suppression, resulting in excessive secretion of thyroid hormones T3 and T4 (Önnestam et al., 2013). Drug treatment of thyrotrophic adenomas is based on long-acting SSAs, which include octreotide and lanreotide.
Some studies have shown that they normalize TSH and thyroid hormone levels in more than 80% of patients and reduce tumor size in more than 40% of patients (Kuhn et al., 2000; Malchiodi et al., 2014). Although cholelithiasis and carbohydrate intolerance and transient gastrointestinal side effects may occur, SSAs are safe enough to be used during pregnancy (Blackhurst et al., 2002; Chaiamnuay et al., 2003).
Corticotrophic PitNETs
Corticotrophic PitNET or ACTH-secreting pituitary adenoma is the most common cause of Cushing's syndrome, secreting excessive amounts of ACTH, and stimulating adrenocortical steroidogenesis and cortisol production (Bertagna et al., 2009; Cuevas-Ramos and Fleseriu, 2014). The ACTH-secreting pituitary adenomas account for ∼70% of endogenous Cushing's syndrome cases and are associated with significantly increased morbidity and mortality (Pivonello et al., 2016).
In the clinical manifestation of corticotrophic PitNETs, drug treatment strategies that include centrally acting agents, steroidogenesis inhibitors, and glucocorticoid receptor (GR) antagonists play a critical role in normalizing the toxic effects of persistently high cortisol levels.
As an antifungal agent, ketoconazole effectively inhibits several enzymes in the mechanism of cortisol synthesis, which, in turn, normalizes cortisol levels in ∼50% of patients (Castinetti et al., 2014). The availability of ketoconazole has been restricted in many countries according to European Medicine Agencies, and the U.S. Food and Drug Administration (FDA) issued a “black box warning” due to the potential risk of hepatotoxicity associated with its use (Castinetti et al., 2014). Although the potential risk of acute liver failure associated with ketoconazole use is only about 3 in 1000 patients per year, prospective long-term safety studies are needed (Lo Re III et al., 2016).
Mitotane is an adrenolytic and is used to treat all forms of hypercortisolism (Baudry et al., 2012). Compared with other steroidogenesis inhibitors, mitotane has a slow onset of action (Fleseriu and Petersenn, 2013; Luton et al., 1979). According to the data of a retrospective study, normalization of 24-h free urine cortisol levels of up to 80% was achieved in patients with ACTH-secreting pituitary adenoma (Baudry et al., 2012).
Despite its high efficacy, mitotane is not suitable as monotherapy due to its long onset of action and its various potential side effects, including gastrointestinal, neurologic, metabolic, hepatic, hematologic, skin, and bladder toxicities (Lonser et al., 2017; Tritos and Biller, 2019). Etomidate is an intravenous anesthetic that rapidly decreases postoperative serum cortisol levels by inhibiting multiple steps of cortisol synthesis (Allolio et al., 1988; Drake et al., 1998; Preda et al., 2012; Schulte et al., 1990).
Clinical use of etomidate is limited due to the potential for various sedative side effects (nausea, vomiting, myoclonus, and dystonia) and the need for careful dose titration and patient monitoring (Carroll et al., 2019).
Metyrapone blocks the terminal enzyme involved in cortisol synthesis that converts 11-deoxycortisol to cortisol, resulting in controlled serum cortisol levels in ∼50% to 75% of patients (Daniel et al., 2015; Feelders and Hofland, 2013). Potential adverse effects associated with metyrapone use include dizziness, gastrointestinal discomfort, hyperandrogenism in women (hirsutism, acne), and mineralocorticoid excess (hypertension, edema, hypokalemia) (Daniel et al., 2015; Nieman et al., 2015; Tritos and Biller, 2014). Although metyrapone is not FDA approved for use during pregnancy, it has been found in the literature to be suitable for monotherapy in pregnant patients (Gormley et al., 1982; Lindsay et al., 2005).
Mifepristone is a potent GR antagonist that inhibits dexamethasone suppression and increases endogenous cortisol and ACTH levels (Bertagna et al., 1984; Fleseriu et al., 2013). Treatment with mifepristone can lead to adrenal insufficiency due to the increase in cortisol and ACTH levels compared with baseline, which can be treated by administering high doses of dexamethasone (Fleseriu et al., 2013). Serious adverse effects of mifepristone that limit its clinical utility include adrenal insufficiency and hypokalemia (Fleseriu et al., 2014).
Pasireotide and its long-acting formulation, pasireotide LAR, act as somatostatin receptors and control cortisol levels in 19% of patients, but they also exhibit a hyperglycemic effect causing glucose intolerance in 73% (Colao et al., 2012). Gastrointestinal side effects such as diarrhea, nausea, abdominal pain, and cholelithiasis, which are a common disadvantage of somatostatin receptor antagonists, also pose a risk to patients treated with pasireotide.
In the clinical management of corticotropic PitNET, a combined approach with some of the drugs may be effective in patients who do not respond to a single agent.
Lactotrophic PitNETs
Prolactinomas, more recently referred to as lactotrophic PitNETs, are usually benign neoplasms but affect the quality of life of patients by impairing vision, sex life, and fertility. Prolactinomas are manifested by complications such as osteoporosis, amenorrhea, and galactorrhea, which occur as a result of elevated prolactin levels and disrupt the hypothalamic-pituitary-gonadal axis (Chanson and Maiter, 2019).
Restoration of normal gonadal functions, reversal of mass effects, and shrinkage of the tumor are the main goals of treatment. The first-line treatment for prolactinoma is drug therapy, followed by surgical resection and radiotherapy in resistant cases that do not respond adequately to drug therapy (Chanson and Maiter, 2019; Vroonen et al., 2019). The DAs including cabergoline, bromocriptine, and quinagolide are used as first-line therapeutic agents for prolactinoma (Barlier and Jaquet, 2006; Casanueva et al., 2006; Gillam et al., 2006; Melmed et al., 2010). Despite their efficacy, DAs can also have adverse effects.
Nausea, dizziness, vomiting, headache, and constipation are common adverse effects of DAs. Patients with macroadenomas may require higher doses of DAs, so clinicians should be aware of the valve risk that may occur as a result of high doses (Molitch, 2014). Another adverse effect that may be caused by DAs is compulsive behaviors such as gambling and hypersexuality (Noronha et al., 2016).
On the other hand, the treatment of DA-resistant prolactinomas is a real challenge for the clinic. The SSAs such as octreotide and pasireotide have also been reported as therapeutic agents for the treatment of resistant prolactinomas (Coopmans et al., 2019; Sosa-Eroza et al., 2018). Treatment with pasireotide has been reported to result in normoprolactinemia and tumor shrinkage (Coopmans et al., 2019). Octreotide LAR has also been reported to reduce both tumor size and prolactin levels when used synergistically with ongoing cabergoline treatment (Sosa-Eroza et al., 2018).
Like all chemotherapeutic agents, these SSAs can cause adverse side effects such as alopecia, abdominal cramps, flatulence, hyperglycemia, and diarrhea (Casanueva et al., 2006; Lasolle et al., 2017).
Nonfunctioning PitNETs
NF-PitNETs are a histopathologically diverse group of tumors that are usually benign and do not manifest with endocrinopathies (Trouillas et al., 2020; Yavropoulou et al., 2020). NF-PitNETs are difficult neoplasms to diagnose, because they have no signs other than mild hyperprolactinemia due to dysfunction of the pituitary stalk. As long as they do not cause symptoms such as visual disturbances and headaches, they may not be recognized. Once it causes symptoms, the tumor usually becomes a macroadenoma.
Transsphenoidal surgery is the main treatment in most cases of nonfunctioning and functioning PitNETs to decompress the affected adjacent structures, to relieve visual disturbances and headaches, and to achieve rapid reduction of high levels of hyper-secreted hormones (Greenman, 2017; Molitch, 2014). However, postoperative residuals are common, especially in resection of macroadenomas due to their larger shape and cavernous invasion, which also negatively affects clinical outcome (Even-Zohar and Greenman, 2018; Greenman and Stern, 2015).
Despite the clinical prevalence of NF-PitNETs, no drug treatment is currently approved for them, and an effective pharmacological therapy for NF-PitNETs is still in the trial phase (Greenman, 2017). Because there are currently no clinically used therapeutics for NF-PitNETs, we reviewed the studies that reported clinical trials, case studies, or in vivo trials.
Cabergoline, bromocriptine, and octreotide LAR have been tested for the treatment of NF-PitNET (Batista et al., 2019; Fusco et al., 2012; Greenman et al., 2016). Patients treated with cabergoline showed shrinkage of residual tumor (28.8%) and tumor stabilization (66.1%) after transsphenoidal surgery (Batista et al., 2019). In another study, DAs therapy was associated with a reduced prevalence of residual tumor size after surgery (Greenman et al., 2016). Stabilization of residual tumor was achieved in 81% of patients treated with octreotide LAR. However, tumor shrinkage, change in visual status, and improvement in pituitary function were not observed (Fusco et al., 2012).
TBR-760, a chimeric compound of DA and SSA (dopastatin), is another therapeutic agent that was used to treat NF-PitNET in a mouse model of aggressive NF-PitNET (POMC-KO) and showed complete tumor growth arrest. TBR-760 has been suggested as a candidate for drug treatment of NF-PitNETs since it causes tumor shrinkage (Halem et al., 2020). Vázquez-Borrego et al. (2020c) have shown that SST3 can mediate a reduction in tumor growth in vivo in POMC-KO mice. Another study by the same group reported that BIM-065, a novel chimeric agonist for SSTR2/SSTR5/DR2, increased apoptosis in primary cell cultures of NF-PitNETs (Vázquez-Borrego et al., 2020a). Clinical trials with these potential agents are needed to clarify the efficacy and safety of these candidates as therapeutic options for the treatment of NF-PitNETs.
APTs and PCs
The APTs are neoplasms that have a rapid growth rate or progression tumor growth despite currently used treatment options such as surgery, radiotherapy, and chemotherapy (Lamb et al., 2020). According to the classification by WHO (2017), the evaluation of histological markers provides clues to potential tumor behavior. For example, if Ki67 is above 3%, the tumor may have the potential to exhibit aggressive clinical behavior (Lloyd et al., 2017).
The PCs are defined by the presence of metastatic spread of an adenohypophyseal tumor, which may be craniospinal or systemic (Trouillas et al., 2020). The mortality rate for these tumors is quite high (McCormack et al., 2018).
The current first-line strategy for APTs and PCs is to treat these patients chemotherapeutically with temozolomide, an alkylating drug that has shown modest activity against these tumors with an intermediate response rate and improves survival in responders (Lasolle et al., 2017; McCormack et al., 2018). However, a significant proportion of patients with APTs and PCs showed progression despite temozolomide treatment (McCormack et al., 2018). Temozolomide is also recommended for aggressive gonadotrophic tumors and prolactinomas, but it has not shown sufficient long-term efficacy (Elbelt et al., 2020; Ilie and Raverot, 2020; McCormack et al., 2018).
Targeted therapy with antibodies is another proposed option for the treatment of APTs and carcinomas (Cooper et al., 2021; McCormack et al., 2018). Bevacizumab is a humanized anti-vascular endothelial growth factor (VEGF) monoclonal antibody that demonstrated suppression of angiogenesis by blocking VEGF A and inhibiting mitogen-activated protein and inositol triphosphate. Touma et al. (2017) reported the successful treatment of a patient with ACTH-secreting PC by concurrent chemoradiation and combined temozolomide/bevacizumab therapy with long-term follow-up and no recurrence.
Lapatinib, a synthetic quinazoline and a tyrosine kinase inhibitor (TKI) that reversibly blocks epidermal growth factor receptor (EGFR), Erb-B2 receptor tyrosine kinase 2 (ErbB2), extracellular signal-regulated kinases (Erk-1 and Erk-2), and AKT kinases, has potential antineoplastic properties (Cooper et al., 2021). Prolactinoma ErbB receptor expression and targeted therapy is observed in aggressive tumors. Short-term therapy with lapatinib has been proposed as an effective strategy to control tumor growth and lower PRL levels in patients with aggressive prolactinomas (Cooper et al., 2014, 2021).
Other TKIs have also been reported for the treatment of APTs, including apatinib and everolimus (Donovan et al., 2016; Wang et al., 2019; Zhang et al., 2019). A patient with GH-secreting recurrent PitNET was successfully treated with a combination of temozolomide and apatinib for 31.5 months without recurrence (Wang et al., 2019). Again, a patient with nonmetastatic aggressive prolactinoma was treated with everolimus, a mammalian target of rapamycin (mTOR) inhibitor, and cabergoline. As a result of treatment, tumor regression occurred, and it remained stable for 12 months. In addition, a decrease in serum prolactin levels was observed (Zhang et al., 2019).
The effects of the combined use of cabergoline and everolimus were also tested on GH3 cells. Cell proliferation was not affected, but prolactin secretion was affected by the synergistic inhibition of cabergoline and everolimus.
A female patient with an ACTH-secreting PC with an STK11(F298L) mutation and systemic metastases was treated with everolimus, which stabilized the disease, but the patient died due to the systemic metastases (Donovan et al., 2016). Pembrolizumab, a humanized IgG4-κ monoclonal antibody against programmed death-1 receptor, was used to treat aggressive ACTH-secreting PitNET and resulted in tumor progression and poor efficacy (Caccese et al., 2020).
As with all onco-therapeutics, the aforementioned treatments can have notorious side effects and affect patients' quality of life. In addition, only temozolomide has efficient treatment response results compared with other case studies tested in larger groups. However, temozolomide has serious and notorious side effects such as fatigue, cytopenias, headache, nausea, hearing loss, adrenal crisis, and abnormal liver function (McCormack et al., 2018; Raverot et al., 2018). Therefore, there is an urgent and unmet need for the development of alternative and effective therapeutics to support the treatment of these challenging neoplasms.
Current Clinical Trials for the Management of PitNETs
There are recently completed clinical trials investigating potential drugs to treat specific subtypes of PitNET (Table 2). Regarding the treatment of patients with corticotrophic PitNETs, osilodrostate is a new treatment option approved in Europe based on the results of a prospective phase III clinical trial (Pivonello et al., 2020). Another clinical trial shows that a new SSA, somatoprim, suppressed GH secretion in a large number of somatotroph adenomas that did not respond to octreotide.
Drugs in the Ongoing Clinical Investigational Phase for the Treatment of Pituitary Neuroendocrine Tumors
Represented recently finished clinical trials.
EGFR, epidermal growth factor receptor; ERBB2, Erb-B2 receptor tyrosine kinase 2.
Moreover, the weak effect of somatoprim on the potential for insulin suppression is an advantage to be an alternative to octreotide (Plockinger et al., 2012). According to a prospective small single-arm, multicenter phase IIa study, treatment with lapatinib may show significant efficacy in controlling tumor growth and lowering prolactin levels in patients with aggressive prolactinomas (Cooper et al., 2021).
There are also a large number of ongoing clinical trials focused on finding effective drugs for the treatment of PitNETs. An open-label clinical trial is currently underway to evaluate the efficacy and safety of capecitabine in patients with recurrent PitNETs (https://clinicaltrials.gov/: NCT03930771). Two clinical trials are ongoing for the combination of immune checkpoint inhibitors, namely nivolumab and ipilimumab. A phase II clinical trial of the combination of nivolumab and ipilimumab in patients with APTs is ongoing (https://clinicaltrials.gov/: NCT04042753). Another phase II trial of nivolumab and ipilimumab in the treatment of patients with rare tumors is ongoing (https://clinicaltrials.gov/: NCT02834013). The results of these clinical trials may provide insight into the efficacy of immune checkpoint inhibitors in aggressive PitNETs.
An open-label phase II clinical trial is being conducted in patients with somatotrophic PitNETs to evaluate the safety, tolerability, and efficacy of IONIS-GHR-LRx, an antisense inhibitor of the GH receptor (https://clinicaltrials.gov/: NCT04522180). A multicenter trial of R-roscovitine, known to reduce ACTH levels and tumor growth in previous animal studies [89], is currently underway to treat patients with Cushing's syndrome (https://clinicaltrials.gov/: NCT03774446).
Another open-label phase II study is ongoing for the treatment of patients with Cushing's syndrome, to evaluate the pharmacokinetics, pharmacodynamics, and tolerability of osilodrostate (https://clinicaltrials.gov/: NCT03708900). An open-label study evaluating the efficacy and tolerability of the nonergoline DA ropinirole in the treatment of patients with lactotrophic PitNETs is ongoing (https://clinicaltrials.gov/: NCT03038308).
DR to Guide Upcoming Therapies for PitNETs
DR, also called drug repurposing, drug recycling, or drug retasking, is a strategy for identifying new therapeutic uses for existing drugs that holds promise for drug discovery and development. Drug discovery is a resource- and labor-intensive, time-consuming, and costly process. The global pharmaceutical industry faces many challenges, as the research and development of new drug molecules to market takes a long time and is also accompanied by changing regulatory requirements, all of which can lead to higher costs.
In addition, major issues would arise during clinical trials regarding the safety and efficacy of the new drug (Shim and Liu, 2014; Würth et al., 2016). These challenges make the pharmaceutical industry a less desirable choice for investors (Pushpakom et al., 2018). In contrast to the discovery of a new drug, the repositioning strategy offers many opportunities, such as known, established formulations, extensive safety data on pharmacokinetics, toxicity, clinical trials, and postmarketing surveillance (Deotarse et al., 2015).
Although this strategy is far from new, there is a growing interest in DR, as evidenced by the development of a large number of academic publications in the past decade (Talevi and Bellera, 2020). Moreover, numerous drug repurposing-focused companies or initiatives have been created in the past 20 years as well (Naylor et al., 2015).
Among the many examples of DR, one of the best known is sildenafil (also known as Viagra), which was manufactured for coronary heart disease. It failed after the phase II trial and is intended for the treatment of erectile dysfunction, which was a side effect in the late 1990s (Turanli et al., 2018a). Therefore, it can be said that this method has gained a lot of attention in recent decades, as repositioning drugs account for one-third of recent approvals and about 25% of pharmaceutical companies' annual sales come from repositioned drugs (Naylor et al., 2015).
Although we have focused on how DR has been achieved over time, most of the successful and best-known DR stories (e.g., sildenafil, minoxidil, aspirin, valproic acid) have come about either after serendipitous observations or already known pharmacology of a drug (e.g., an off-target side effect, retrospective clinical experience) to solve a clinical problem from another field (Talevi and Bellera, 2020). So far, it should be emphasized that most successful examples have not yet been elaborated through a systematic approach. On the other hand, serendipity is not yet sufficient to obtain new drugs. Therefore, successfully repurposed drugs have also stimulated the development of more systematic approaches to identify new drugs (Turanli et al., 2018b).
These systematic approaches can generally be divided into computational approaches and experimental approaches (Pushpakom et al., 2018), with both approaches used synergistically. As the example of using clinical data for DR illustrates, these two broad areas are interrelated. The availability of established clinical compound libraries and advances in omics technologies and bioinformatics have accelerated both experimental and computational repositioning of compounds. Accumulated biotechnological data on the metabolome, lipidome, and microbiome, as well as computational methods, make current DR efforts more rational in terms of identifying drug candidates for repositioning (Turanli et al., 2019a).
The experimental DR offers the use of actual drug applications for screening. In contrast to wet-lab experiments, computational DR uses biological databases and bioinformatics tools to systematically discover interaction networks between drugs and their protein targets. Both methods have their advantages and disadvantages. Computational DR is a potentially powerful technology, because it saves time and costs.
However, it requires high-resolution structural information of drugs and targets. It also requires disease/phenotype information or gene expression profiling, which means that in silico systems also need experimental data first. On the other hand, experimental DR is time and labor intensive. It requires a whole collection of existing drugs and the development of a screening assay, but it can be used without structural information on target proteins or a database, and it is easy to validate because false positive rates for in silico repositioning are low (Shim and Liu, 2014).
Because DR relies on data about existing drugs and diseases, a wealth of publicly available biomedical big data, along with high-throughput experimental techniques and high-performance computers, has accelerated the development of computational approaches to DR in recent years. Multidisciplinary researchers and scientists have conducted computational DR studies with varying degrees of efficiency and success (Jarada et al., 2020).
Computerized studies for DR can be classified into different categories depending on where the knowledge comes from: (i) drug-based strategies, where the discovery comes from knowledge about drugs, and (ii) disease-based strategies, where the discovery comes from knowledge about diseases (Jarada et al., 2020). There are also different approaches and efforts of computational DR. They can also be categorized according to which computational method is used, although they are not limited to these two general approaches: (i) signature-based strategies, where a common transcriptomic signature between two drugs could mean that they also have a common therapeutic application, and (ii) network-based strategies, where discovery comes from disease- and target-oriented networks (Turanli et al., 2019a).
Computational DR can also be achieved through molecular docking, pathway mapping, genome-wide association studies, adverse event profiling, and electronic health records (Turanli et al., 2021).
Rational DR methods are being investigated to identify target candidates and potential drugs considering data from different omics levels as well as the disease-gene-drug triad (Turanli et al., 2017). Recently, clinical genomic and/or transcriptomic data have been evaluated as part of a comprehensive, systematic, and integrative analysis applied to specific medical conditions, and numerous systems biology approaches based on gene expression data have been published for in silico drug discovery by using publicly available gene expression data (Aydin et al., 2020, 2021; Beklen et al., 2020).
In another study, a large set of drug-induced transcriptional modules was identified from genome-wide microarray data of drug-treated human cell lines (Iskar et al., 2012). In addition, bioinformatics tools and databases have been created to help researchers conduct effective DR studies, such as PharmDB (Lee et al., 2012), PROMISCUOUS (von Eichborn et al., 2011), DRUGSURV (Amelio et al., 2014), DrugMAP central (Fu et al., 2013), “RE:fine Drugs” (Moosavinasab et al., 2016), and geneXpharma (Turanli et al., 2017). Detailed information on databases and tools can also be found in the literature (Sercinoglu and Ozbek Sarıca, 2019; Turanli and Arga, 2019).
Moreover, genome-scale metabolic models are used effectively to predict potential drug targets and analyze drug responses at the molecular level (Turanli et al., 2019b).
Since DR is an important strategy in general, we can emphasize that it is an essential strategy for cancer patients, because chemotherapeutic drugs have notorious side effects that significantly reduce the quality of life. Therefore, drug switching can be a hope for cancer patients, as most noncancer drugs have minor or tolerable side effects on human health (Frantzi et al., 2020; Würth et al., 2016).
Another important point to mention here is that the tumor microenvironment (TME) could modulate processes associated with tumorigenesis, such as angiogenesis, cell proliferation, migration, and invasion (Arneth, 2020; Marques et al., 2020). The TME also influences patient response to treatment, metastasis, and clinical outcome (Dzobo et al., 2020; Wu and Dai, 2017). Not only in PitNETs (Marques et al., 2019, 2021; Sato et al., 2019), but also in various cancers, TME could provide a broader view of cases related to aggressiveness, invasion, and recurrence (Marques et al., 2019). Therefore, an approach that incorporates TME-driven DR could have significant potential for expanding drug design, selection, and targeting (Dzobo and Dandara, 2020).
In addition, the opportunities offered by switching drugs to meet the urgent need for treatment of the current coronavirus epidemic cannot be underestimated. Therefore, the pandemic is another condition where only DR can provide rapid medical solutions to treat patients during the pandemic. The specific DR options for coronavirus infections are discussed in detail (Harris et al., 2020; Islam et al., 2020).
Last but not least, current strategies for drug repurposing have evolved and new ones will be developed in the future as precision medicine deepens the characterization, understanding, and detection of disease subtypes (Tanoli et al., 2021; Turanli et al., 2017). In parallel, technological advances and methods to integrate multi-omics data will be required to efficiently extract and integrate heterogeneous Big Data, such as imaging and structural data or clinical trial documentation, electronic health records, etc., which can only be processed by machine learning in the near future (Tanoli et al., 2021; Arga and Sinha, 2021).
Current repurposed drugs for PitNETs
As mentioned in the previous part, DR has an undeniable potential to establish candidates for the treatment of diseases that are outside their indications. Therefore, we carefully searched the literature for repositioned drugs for efficient treatment of PitNETs. In this section, we evaluated DR studies in two categories based on previous medical observations and systematic approaches to DR, both computational and experimental (Table 3).
Repurposed Drugs for the Management of Pituitary Neuroendocrine Tumors
Italic typed drugs represented studies that did not conduct a drug repositioning method.
ACTH, adrenocorticotropic hormone.
Notably, three drugs, artemisinin, simvastatin, and metformin, have been repositioned for the treatment of PitNETs based on previous medical observations rather than a rational DR methodology. Artemisinin is a sesquiterpene trioxane lactone with multiple pharmacological activities such as anti-malarial, anti-parasitic, and anti-cancer (Ho et al., 2014; So et al., 2017). An artemisinin derivative, artesunate, was investigated for its effect on the GH3 PitNET cell line. Mao et al. (2012) showed that artesunate inhibited proliferation of GH3 cells, induced apoptosis and cell cycle changes, decreased GH level and GH mRNA expression, and was proposed as a potential drug for the treatment of GH-secreting PitNETs.
Simvastatin belongs to the hexahydronaphthalene class of drugs and is a lipid-lowering agent commonly used to lower cholesterol and treat cardiovascular disease. Simvastatin has been reported to exhibit antitumor effects by reducing cell viability and hormone secretion in corticotropic, somatotropic, and NF-PitNETs and decreasing GH/PRL/ACTH/LH/FSH secretion but not their mRNA expression (Vázquez-Borrego et al., 2020b).
Metformin is a bioguinade, an antidiabetic and antihyperglycemic agent that has been studied in several trials outside its indication (An et al., 2017; Vázquez-Borrego et al., 2019). The repositioning of metformin and its potential associations with cancer treatment have been investigated in several studies (Kheirandish et al., 2018; Quinn et al., 2013). Metformin has also been described for PitNETs in terms of decreased tumor cell proliferation and decreased GH secretion in vivo (An et al., 2017; Vázquez-Borrego et al., 2019). It is the first repurposed therapeutic agent as a potentially promising for the treatment of PitNETs.
A potential treatment method using DR to treat corticotrophic PitNETs was performed by Yu et al. (2020). They constructed a protein–protein interaction (PPI) network that focused on the Nur77 protein (expressed by the NR4A1 gene) and used this PPI network as a query to search for related drug candidates. As a result, bexarotene, a retinoid that binds and activates retinoid X receptors, including RXRα, RXRβ, and RXRγ, was selected as a repurposed drug.
Then, another drug was selected for combinatorial use with bexarotene by investigating drugs targeting the PI3K/Akt pathway downstream of both Nur77 and RXRα. In the search for drugs targeting EGFR, the upstream regulator of AKT, several drugs were found. Of the drugs found, lapatinib was reported to impair AtT20 cell viability. Therefore, they combined bexarotene and lapatinib, which target the PI3K/Akt pathway and may have a cross-linked effect. Synergistic use of these drugs showed inhibitory effects on tumor growth and ACTH levels in vivo (Yu et al., 2020).
Recently, our research group published a study demonstrating the integration of omics data and the use of this integration to perform signature-based DR to identify potential drug candidates for the treatment of prolactinoma. In the earlier study, coding and noncoding transcriptome data were collected, analyzed, and integrated through a transcriptional regulatory network. Subsequently, the identified prolactinoma-specific signatures were used as a query for a signature-based DR technique using LINCs data and the L1000CDS2 tool.
As a result, drugs belonging to both onco-therapeutics and noncancer therapeutics were found. Their efficacy was confirmed by cell proliferation, cell cycle analysis, and protein level experiments using the prolactin-producing MMQ cell line. In summary, noncancer therapeutics such as 5-flourocytosine (antifungal), nortriptyline (a tricyclic antidepressant), puromycin (antibiotic), taxifolin (a flavonol with antioxidant activity), and zileuton (anti-asthma) have the potential to treat prolactinomas.
Onco-therapeutics such as neratinib (a TKI) and vorinostat (a histone deacetylase inhibitor) also showed anti-proliferative effects on MMQ cells. These drugs were evaluated for their effects on the cell cycle phases of MMQ cells. In addition to cell cycle analysis, the critical signaling pathway PI3K/Akt, which plays an important role in cell survival, cell cycle progression, cell proliferation, and angiogenesis, was tested for each drug.
The results of this study showed that these seven repositioned agents can affect tumor growth and progression, and therefore should be tested in vivo models (Aydin et al., 2021). The possibility of achieving efficient tumor inhibition with the proposed noncancer drugs gives us hope to treat patients with prolactinomas in a way that will result in fewer side effects compared with oncology drugs.
In summary, subsequent to the popular use of the concept of “drug repositioning” (Ashburn and Thor, 2004), 19 drugs were repurposed with their anti-neoplastic effects (Dueñas-González et al., 2008). The National Center for Advancing Translational Sciences (NCATS) by the National Institute of Health launched drug repurposing program in 2012 (Allison, 2012). In 2014, The Library of Integrated Cellular Signatures (LINCS) L1000 released pertubagen profiles consisting of ∼20,000 perturbagens, ∼15 cell lines, and ∼1,400,000 gene expression profiles (Duan et al., 2014).
The first drug repurposing study on endocrine tumors evaluated the role of anti-diabetic drug metformin in the treatment (An et al., 2017; Vázquez-Borrego et al., 2019). In 2020, the first network-based DR study for Cushing disease reported a combination of bexarotene and lapatinib for the treatment of this disease (Yu et al., 2020). Most recently, Aydin et al. (2021) reported that miRNA-oriented signature-based DR revealed seven repositioned drugs for the treatment of prolactinomas. As seen, all studies using systematic DR approaches have been conducted in the past 4 years (Fig. 3).
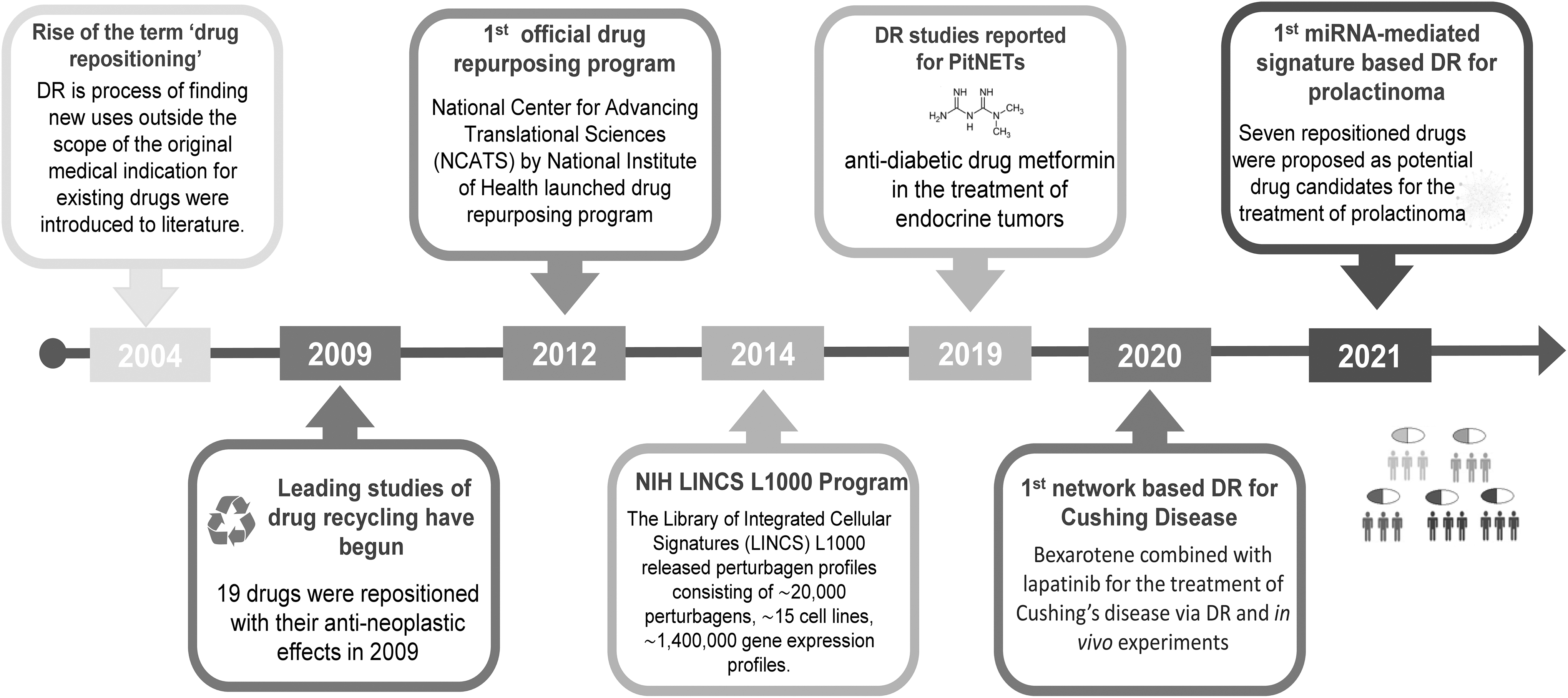
Timeline of drug repositioning including PitNET-associated milestones.
Conclusions and Outlook
Cutting-edge advances in molecular biology, pathology, and omics sciences have allowed us to make great strides in many areas of disease research. These developments enable us to understand the mechanisms of diseases and develop appropriate treatments to cure them. In this expert review, we provided an overview of the therapeutics currently used in the clinic and the ongoing clinical trials for the treatment of PitNETs. Although the drugs presented in the article reflect the efforts to reduce hormone hypersecretion and tumor volume, many studies have shown that some patients cannot or will not respond to the proposed treatments.
A growing body of evidence shows that many attempts have been made to achieve treatment of these neoplasms. However, there is an urgent need for new innovation strategies and effective treatments for these difficult neoplasms.
The expected progress has been rather limited in the field while we think about efficient drug development and therapeutic strategies, as case reports and occasional case series contribute to the slow progression associated with PitNETs. Accordingly, the search for new therapeutic modalities to expand the pharmacological pool for the treatment of PitNETs patients is urgent. Therefore, promising avenues such as multi-omics-based DR hold great potential to advance the drug discovery process and application steps.
The DR also offers targeted therapies, as knowledge comes from multistep elucidation of the molecular profile of diseases and it facilitates the development of anti-cancer strategies and/or combination therapies by using noncancer drugs with fewer adverse effects.
In the short term, further improvement of DR-based treatment strategies, their individualized use, and logical combination therapies through their precise spatiotemporal application are expected to lead to better outcomes for PitNETs patients. Innovation roadmaps remain important as they are relevant to individual scientists, institutions, universities, and nation states as well as for effective collaboration across multiple countries and geographies.
Thus, the future of PitNET therapeutic innovation seems bright, but provided that rational and smarter approaches such as personalized-precision treatment of PitNETs are pursued. This analysis suggests that DR and omics research are well poised to pave the way for the exploration of known compounds as potential therapeutics for the treatment of PitNETs.
Footnotes
Acknowledgments
The scholarships under YOK 100/2000 Doctoral Fellowship Program and 2211-C Doctoral Fellowship Program of the Scientific and Technological Research Council of Turkey (TUBITAK) provided to B.A., and the scholarship provided to E.Y. and B.A. under project number 3629 from the Health Institutes of Turkey are greatly acknowledged.
Author Disclosure Statement
The authors declare they have no conflicting financial interests.
Funding Information
This research was financially supported by Health Institutes of Turkey (TUSEB) under project number 3629.