
Abstract
Coronavirus disease 2019 (COVID-19) is a systemic disease that impacts multiple organ systems with a complex clinical presentation and outcomes that can vary from person to person and between populations. To optimize COVID-19 treatment outcomes, and in light of the availability of antiviral drugs, there is a need for greater attention to the field of theranostics, the fusion of therapeutics and diagnostics. Theranostics tests would be invaluable, we suggest in this expert review, so as to optimize the efficacy and safety of current and future antiviral drugs against COVID-19. Theranostics would also assist in the design and implementation of clinical trials with antiviral drug candidates. We discuss here theranostics considering drugs such as remdesivir, Paxlovid™, and molnupiravir. All in all, we underscore that theranostics as a concept and practice is essential for efficient and safe health interventions against COVID-19 and other ecological crises in the 21st century.
Introduction
In March 2020, the coronavirus disease 2019 (COVID-19) was declared a pandemic by the World Health Organization (WHO) due to the high infectivity rate and geographical spread of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus, which disseminated rapidly causing major global impacts (Hu et al, 2020). The virus spread led to challenges in managing health care systems, mainly given the emergence of new variants and the need to develop therapies to treat and prevent infections, besides preventing transmission (Dewan and Islam, 2022; Matrajt et al, 2022).
COVID-19 is characterized by heterogeneous symptoms and clinical outcomes regarding disease severity, as patients who test positive can either be asymptomatic or have multiple organ involvement (Pereira et al, 2021). Thus, the National Institutes of Health (NIH, 2022a) guidelines for COVID-19 treatment are broad and include antiviral drugs, cell-based therapy, anti-SARS-CoV-2 antibodies, corticosteroids and immunomodulators, antithrombotic therapy, and supplements.
Proper diagnosis is known to be one of the most critical aspects of containing coronavirus spread, as it allows the identification of infected patients, exclusion of suspect cases, contact tracing, and monitoring of the viral load during patients' treatment (Shih et al, 2020). In light of this, the NIH COVID-19 Treatment Guidelines Panel (2022) recommends employing nucleic acid amplification tests (NAATs) or antigen tests with a sample collected from the upper respiratory tract to diagnose acute SARS-CoV-2 viral infection. Moreover, it is recommended that the diagnosis of acute infection should not be based solely on the results of serological tests, which detect antibodies.
Thus, diagnostic tests based on reverse transcription polymerase chain reaction, which detect viral nucleic acids, are considered gold standard tests. They can detect virus ribonucleic acid (RNA) in samples collected days or weeks after symptom onset (Arons et al, 2020). On the other hand, diagnostic tests based on viral antigen detection, which are less sensitive than NAATs, have better performance at the beginning of symptomatic infection, when the viral load is considered to be higher. Since it may take 21 days or more after symptom onset for seroconversion (the development of detectable immunoglobulin IgM and/or IgG antibodies to SARS-CoV-2), serologic testing is not recommended as the sole basis for diagnosing acute coronavirus infection (Guo et al, 2020).
Aside from detecting the viral agent or its correspondent immunoglobulin, another important tool of diagnostics, which also envisages prognosis, is biomarkers: a functional variant or quantitative index of a biological process that predicts or reflects the evolution of or predisposition to a disease or a response to therapy (Aronson and Ferner, 2017). A review study that contemplated data from December 2019 to August 2020 found that common biomarker levels, such as elevated D-dimer, C-reactive protein, aspartate transaminase, and others, were correlated with poor outcome (Malik et al, 2021).
As our knowledge grew and evidence started to show the wide spectrum that the infection of SARS-CoV-2 can clinically manifest in certain individuals, biomarkers showed great potential in helping physicians to make more accurate decisions on how to manage the symptoms and progress to recovery (Battaglini et al, 2022). Genetic polymorphisms that can alter the individual response to a certain pharmacological intervention may also be considered biomarkers, the so-called pharmacogenomics (Jeelani et al, 2014), which is also being considered an approach to individualize COVID-19 treatment and follow-up (Fricke-Galindo and Falfán-Valencia, 2021). An example is a study that analyzed pharmacogenomic variants and elevation of alanine aminotransferase (ALT) caused by remdesivir administration for COVID-19 treatment in 6910 individuals from the Million Veteran Program finding that remdesivir was associated with a 30% increase in ALT peak (Tuteja et al, 2022).
In addition to diagnostic methods, treatment is also crucial in controlling the spread of COVID-19. Personalized medicine, through pharmacogenomics, enables specific and efficient treatments, optimizing the spread control process and helping to reduce costs and side effects, as it seeks to improve drug efficacy and safety. Within this field is theranostics, which refers to the fusion of therapeutic and diagnostic studies to predict the outcomes of health interventions, such as the administration of antiviral drugs for the treatment of COVID-19, seeking effective and safer response (Biswas et al, 2022).
By bringing together information about an individual's genetic and phenotypic biomarkers along with therapeutic data, it is possible to make the outcome of prescriptions such as this more predictable (Ozdemir et al, 2006). Due to the symptomatic variability of COVID-19, precision medicine is a promising and facilitating alternative for its treatment. As each individual is unique and may respond differently than expected to treatments traditionally employed, considering interindividual variability may lead to important implications regarding drug therapy and care in clinical practice (Pereira et al, 2021).
Therefore, understanding the mechanisms and variations in the effectiveness of oral antiviral drugs through personalized medicine is a valuable tool in clinical practice and the fight against COVID-19 (Bajaj and Stanford, 2022). As antiviral therapies avert disease progression and play a key role in preventing virus transmission in high-risk individuals and treating infected patients, especially in the early stages of infection, these drugs have been an important tool in therapy (Usher, 2022).
According to NIH guidelines (2022b), remdesivir, an RNA-dependent RNA polymerase (RdRp) inhibitor, is the only antiviral agent approved by the United States Food and Drug Administration (FDA) for the COVID-19 treatment until November 2022 (Khiali et al 2022). However, drugs such as ritonavir+nirmatrelvir (Paxlovid™) and molnupiravir, which inhibit SARS-CoV-2 viral replication, have received FDA Emergency Use Authorizations licensed for COVID-19 treatment (EMA, 2022; Fan et al, 2022).
As stated in the recommendations, pharmacotherapy is more beneficial and impactful if applied in the early stages of the disease, when there is more active viral replication, rather than letting the infection progress to more advanced and critical stages, characterized by high inflammation (Siddiqi and Mehra, 2020). Hence, understanding the role of antiviral drugs in treating mild, moderate, severe, and critical symptoms to optimize the treatment of COVID-19 patients is primordial and, along with precision medicine, a promising path to fight the pandemic.
Remdesivir
Remdesivir is a monophosphate prodrug analog of 1′-cyano-substituted adenosine nucleotide, synthesized by Gilead Sciences, Inc., (Siegel et al, 2017). Through phosphorylation, remdesivir is converted in the intracellular environment and tissues to its active form (nucleoside triphosphate), which mimics the cell's natural adenosine triphosphate (ATP) (Avataneo et al, 2020; Brown et al, 2019; Fricke-Galindo and Falfán-Valencia, 2021; Rios et al, 2021; Tempestilli et al, 2020; Warren et al, 2016).
Nucleoside triphosphate competes with the cell's natural ATP to be added to the viral RNA chain by RdRp, inhibiting its action. Once incorporated into the chain in position i, the metabolite should inhibit the RNA synthesis in position i + 5. This inhibition hinders virus replication, thus showing antiviral activity (Fig. 1) (Barlow et al, 2020; Gordon et al, 2020; Lamb, 2020; Rios et al, 2021; Tchesnokov et al, 2019; Tempestilli et al, 2020).
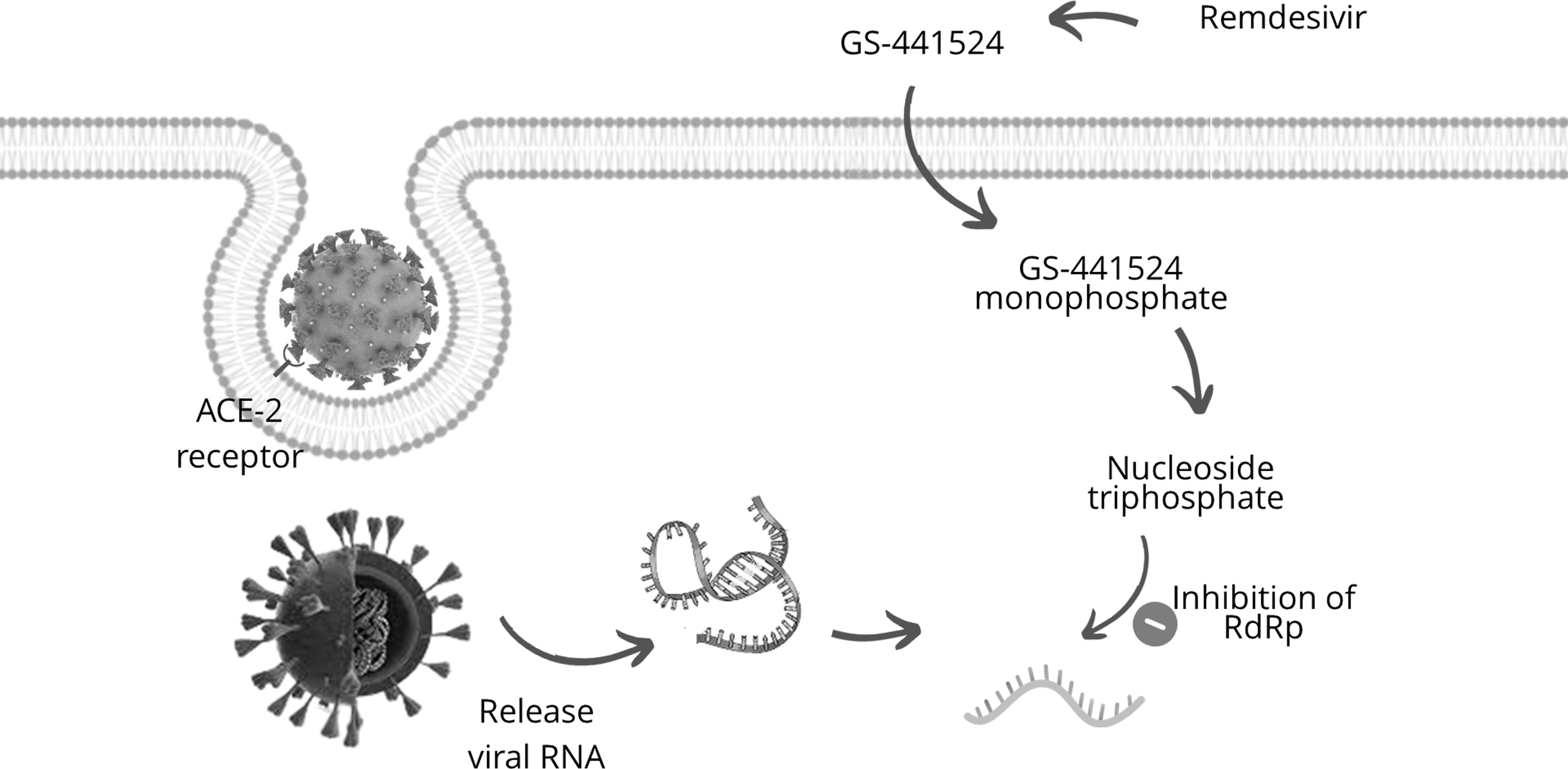
Diagram of remdesivir mechanism of action.
Remdesivir was initially developed for treating diseases caused by RNA viruses, such as the Filoviridae and Coronaviridae families (Carestiato and Weid, 2020). The first tests were conducted for Ebola treatment; no promising result was observed in phase III clinical trials, yet the drug continues to be tested as there are not many drug options for treating some hemorrhagic fevers. With the emergence of the COVID-19 pandemic, it has become a candidate drug for research regarding the treatment of the respiratory syndrome caused by SARS-CoV-2 (Avataneo et al, 2020; Lamb, 2020; Siegel et al, 2017; Walimbwa et al, 2021).
Remdesivir's antiviral activity has been observed in animal models, such as in Rhesus monkeys, and human cells in vitro, mainly lung cells (Fricke-Galindo and Falfán-Valencia, 2021; Lamb, 2020; Tempestilli et al, 2020). Warren et al (2016), using Rhesus monkeys, evidenced the drug's wide antiviral potential not only for the viruses caused by Ebola but also by Coronaviruses.
According to Ko et al (2020), remdesivir effectively reduced SARS-CoV viral load in murine lung cells. Due to such studies early in the pandemic, in 2020, several countries granted emergency permissions for the use of remdesivir to treat COVID-19 patients (Lamb, 2020). Thereafter, studies to increase the understanding of the pharmacokinetics, pharmacodynamics, and adverse effects of remdesivir in humans started to progress.
Remdesivir was first used to treat COVID-19 in humans as early as January 2020. The first COVID-19 case in Washington, United States, was treated intravenously with the drug for a pneumonia condition and after the seventh day of hospitalization, the patient showed clinical improvement. No apparent adverse effect was reported, and a gradual decrease in the patient's viral load was observed (Holshue et al, 2020; Ko et al, 2020).
Along with this case, an Italian research group conducted a study to evaluate remdesivir pharmacokinetics in two severe COVID-19 patients. They observed a high concentration of the prodrug at the time of administration, followed by its decrease and a subsequent increase in the active metabolite concentration. The authors reported an improvement in the clinical symptoms of both patients; however, one of them experienced transient renal failure during the treatment (Tempestilli et al, 2020).
Regarding randomized, double-blind, placebo-controlled phase III clinical trials evaluating the use of remdesivir to treat COVID-19, it is reported that no significant difference in clinical disease progression was observed in patients treated with the drug (Beigel et al, 2020; Wang, et al, 2020). However, clinical improvement and a reduction in the time to this improvement were evidenced in these patients, previously treated with remdesivir. The same studies also observed a reduction in the time to clinical improvement among the treated group compared to placebo, in addition to describing less respiratory tract infection in patients receiving remdesivir.
According to PharmGKB (2022) (https://www.pharmgkb.org) there is no evidence for the association of remdesivir with any gene in in vivo studies. However, based on in vitro results, the prodrug is metabolized by esterases and the CYP2D6, CYP2C8, and CYP3A4 enzymes, codified by homonymous genes. Also, it is known that it acts as a substrate for the OATP1B1 transporter and P-glycoprotein, encoded by SLCO1B1 and ABCB1 genes, respectively (EMA, 2020; Franczyk et al, 2022; Fricke-Galindo and Falfán-Valencia, 2021; Tempestilli et al, 2020; Tuteja et al, 2022). In addition, Tuteja et al (2022) have evidenced that CYP2C19 plays a role in the interindividual variation of remdesivir response: Non-Hispanic White (NHW) individuals with the CYP2C19 intermediate or poor metabolizer phenotype experienced a 9% higher ALT peak than NHW individuals with normal, rapid, or ultrarapid metabolizer phenotype.
However, this result was not significant among Non-Hispanic Black individuals, which suggests an interethnic variability in remdesivir response. CYP2C19 is a very well-known gene in pharmacogenomics, with alleles associated with variation in the response of many drugs, such as clopidogrel and citalopram (Botton et al, 2021); moreover, its interethnic variability is extensively described (Fricke-Galindo et al, 2016), and this recent remdesivir evidence can open a new study field about the association of this gene and antiviral metabolism.
Some CYP2D6 alleles are associated with null or slow enzyme function, such as CYP2D6*4 and *10, and increased function, such as CYP2D6*1xN and *2xN. In addition, it is one of the most polymorphic pharmacogenes (Franczyk et al, 2022; Fricke-Galindo and Falfán-Valencia, 2021). This variability in allele function leads to diverse metabolism phenotypes, which are called “predicted phenotypes”: poor, intermediate, normal, or ultrarapid metabolism, inferred according to the individual's alleles (Caudle et al, 2020). Interethnic variability was extensively described for CYP2D6 allele frequencies, for example, CYP2D6*4 (null function) is more frequent in European populations, whereas CYP2D6*10 (slow function) is prevalent in East Asia (Friedrich et al, 2014; LLerena et al, 2014; Naranjo et al, 2018). This interethnic diversity among allele frequencies, with different metabolism impact, may explain, at least in part, population differences in remdesivir response.
As reported by the Pharmacogene Variation Consortium (pharmvar.org), when compared to CYP2D6, CYP2C8 presents low allelic variability and has no robust evidence of nonfunction alleles (Franczyk et al, 2022). However, according to Fricke-Galindo and Falfán-Valencia (2021), CYP2C8 presents nonfunction alleles, which are well documented in the literature, such as CYP2C8*5, *7, and *11. Nonetheless, these variants do not present relevant interethnic variability.
PharmGKB (https://www.pharmgkb.org) states that there is no evidence for the association of CYP3A4 and remdesivir. Nevertheless, Tempestilli et al (2020) reports an influence of this gene on remdesivir metabolism, although it may be a smaller influence compared to other genes. CYP3A4 has a cytokine-mediated downregulation (Jover et al, 2002), which with the inflammatory process of COVID-19 may increase interleukin-6, decrease enzyme expression, and affect remdesivir metabolism (Franczyk et al, 2022; Fricke-Galindo and Falfán-Valencia, 2021; Jover et al, 2002). Despite there being no attributed allele function in PharmVar, some CYP3A4 alleles, such as *20 and *22, are associated with quetiapine response, but these variants do not present interethnic variability. The polymorphism rs2242480, present in CYP3A4*18 and *36, is associated with tacrolimus response, and its frequency varies among populations (https://www.pharmgkb.org; https://www.ncbi.nlm.nih.gov/snp/). This variant, together with CYP3A4*20 and *22, can be possible subjects of study to explain remdesivir interindividual/interethnic response variability.
Remdesivir is a substrate for both the OATP1B1 transporter and P-glycoprotein. OATP1B1 is responsible for substance absorption into cells of several organs, mainly the liver (Thomson et al, 2016). According to Franczyk et al (2022), genetic variability in transporters involved in drug metabolism may affect this function. The SLCO1B1 gene, which encodes OATP1B1, is highly polymorphic and presents nonfunction variants that may alter transport function (Fricke-Galindo and Falfán-Valencia, 2021; Franczyk et al, 2022; PharmVar).
Considering interethnic variability, rs2306286, a SLCO1B1 variant, presents high frequency differences among populations (from 0.18 to 0.60) and is associated with simvastatin response (https://www.pharmgkb.org; https://www.ncbi.nlm.nih.gov/snp/). Other SLCO1B1 SNPs are mostly associated with statin response, such as rs4149056 and rs59502379; however, there is few robust evidence about this gene and antivirals (e.g., rs4149056 and lopinavir), offering an open field to the conduction of future studies comprising this subject.
P-glycoprotein is involved in cytokine transport, viral resistance, and viral envelopment. There are a few drugs that target this protein, including remdesivir, and it is noteworthy that variation in response to such drugs may occur (Hodges et al, 2011). This may be due to the fact that P-glycoprotein is encoded by ABCB1, which has alleles of pharmacogenomic interest (Franczyk et al, 2022; Fricke-Galindo and Falfán-Valencia, 2021). One of the most known ABCB1 SNPs is rs1045642, which some studies associate with efficacy in antiviral therapy in HIV infection treatment and presents interethnic variability (low frequency in African populations). This association still needs more evidence, but it may be a start point to guide future pharmacogenomic studies using remdesivir.
Some adverse effects associated with remdesivir use were described. According to Barlow et al (2020), patients in the United States have reported nausea, vomiting, gastroparesis, or rectal bleeding after using remdesivir. In addition to these adverse effects, it was observed that some patients showed a high aminotransferase rate 5 days after initiating the treatment, besides liver dysfunction. However, it is unclear if the test alterations were drug related as the studied patients were critically ill, that is, the severity of the disease may have caused the alterations.
As stated previously, ethnicity should be considered in the selection of treatments and throughout the process, but it is also important to emphasize that clinical trials should consider ethnicity and its genetic differences. In clinical trials evaluating remdesivir, it was observed that non-Finnish Europeans had better efficacy of remdesivir treatment compared to East Asians (Wang et al, 2021); however, there is still no robust evidence to explain this difference.
To this extent, remdesivir shows efficacy in containing SARS-CoV-2 replication and reducing patient recovery time. It is metabolized by highly polymorphic genes and differs in its metabolism possibly due to genetic variation. Even though it is very promising for treating COVID-19, clinical studies with larger sample sizes and evaluating ethnic and pharmacogenomic differences are still warranted.
Paxlovid™
Paxlovid™ is a combination of two antiretroviral drugs: nirmatrelvir and ritonavir. Ritonavir is used to treat acquired immunodeficiency syndrome (AIDS), caused by human deficiency virus (HIV) infection. This medication is a pharmacological enhancer able to decrease the activity of the CYP3A4 and CYP2D6 enzymes and, consequently, the metabolism of nirmatrelvir, a second generation protease inhibitor, which is primarily metabolized by these enzymes and acts by inhibiting the 3CL protease of SARS-CoV-2, preventing maturation of polyprotein chains in viral proteins (Fig. 2). Nirmatrelvir mechanism of action, therefore, is similar to molnupiravir, preventing viral replication (Eng et al, 2022; Hung et al, 2022; Vitiello et al, 2022).

Diagram of Paxlovid™ mechanism of action.
Due to the presence of ritonavir in the composition of Paxlovid™, CYP3A4 and CYP2D6 are important genes to be noticed. Their variability was already described in the previous section, as they are also associated with remdesivir metabolism. Still, particularly for ritonavir, CYP2D6 ultrarapid metabolizers may be notably important for personalized medicine. As ritonavir acts by decreasing this enzyme activity, individuals with a high amount of CYP2D6 (the gene is overexpressed in ultrarapid metabolizers) may not experience a satisfactory response using the usual dosage of this drug.
Gorny et al, (2010) reported an excellent example of pharmacogenomic-guided treatment in an HIV patient treated with highly active antiretroviral therapy (with lopinavir+ritonavir, lamivudine, abacavir, and nevirapine). At first, the patient was not responding to the treatment, which was administered according to the guidelines; so, they performed genotyping and confirmed that the patient was an ultrarapid metabolizer for CYP2D6. Due to this, ritonavir had no inhibitory effect on lopinavir metabolism, so the authors empirically increased ritonavir dosage threefold, based only in CYP2D6 genotype-based dosing recommendations for antidepressants and the viral load decreased effectively after 6 days of pharmacogenomic adaptation. This is an example of how pharmacogenomics can optimize treatments with antivirals such as ritonavir. CYP2D6 genotyping could be also a target of pharmacogenomic studies aiming to personalize Paxlovid™ treatment.
In a pharmacological context, drug-drug interaction was observed between drugs that are extensively metabolized by the enzymes inhibited by ritonavir. Feingold et al (2022) suggested suspending lovastatin, atorvastatin, and simvastatin use, indicated for patients with cholesterol disorders, during treatment with Paxlovid™, as these drugs are primarily metabolized by CYP3A4. On the other hand, the use of rosuvastatin requires dose adjustment to be administered in combination with Paxlovid™. As Paxlovid™ is used for a short period (≤5 days), it is possible to do so as long as cholesterol fractions are observed.
Patients taking immunosuppressants, which are also mainly metabolized by CYP3A4, showed increased plasma concentrations of tacrolimus and cyclosporine; it was observed that tacrolimus use should be discontinued due to drug-drug interaction and cyclosporine dosage should be adjusted (Lemaitre et al, 2022; Young et al, 2022); therefore, it is important to pay attention to factors that may be related to drug-drug interaction to not overestimate the risk of worsening the patient's condition (Marzolini et al, 2022).
Wang et al (2021) observed that concomitant use of ritonavir and disulfiram may cause an increased plasma concentration of the latter, leading to adverse effects; in contrast, the authors point out that the combination of ritonavir and ranolazine increases the efficacy of ranolazine, similar to what is observed in the combination that composes Paxlovid™. However, Najjar-Debbiny et al (2022) showed that Paxlovid™ was more effective in cardiovascular and immunosuppressed patients, as well as elders and subjects with neurological disease.
Due to (1) ritonavir's ability to alter the rate of drug metabolism, (2) the wide phenotype diversity usually associated with viral infections, (3) the difficulty in treating these diseases due to the ease of virus mutation in contact with the environment and individuals; (4) and the recurrent intake of polypharmacy due to the patient's other comorbidities, there is a necessity to continue seeking to adapt COVID-19 treatment, especially considering those who are unvaccinated and have compromised immune systems (Singh et al, 2022; Wang et al, 2021).
Molnupiravir
Molnupiravir (MK-4482) is a nucleoside prodrug that is converted primarily to β-D-N4-hydroxycytidine (NHC) in the extracellular environment by plasma esterase, and later is phosphorylated into the active metabolite β-D-N4-hydroxycytidine-triphosphate (NHCtp), this time in the intracellular environment (Parsons et al, 2021). It acts by inhibiting viral replication by mutagenesis and because the tetramers formed can pair with the adenines or guanines of the viral RNA, a two-step RNA mutagenesis can be induced. First, NHCtp is incorporated in the negative strand, and then in step two, induced mutagenesis occurs by pairing NHCtp on the positive strand, resulting in viral apoptosis (Zarenezhad and Marzi, 2022) (Fig. 3). Given the emerging pandemic caused by SARS-CoV-2, an RNA virus, the need for studies regarding these antiretrovirals aiming to control the spread and treat COVID-19 patients has been heightened (Zhou et al, 2021).

Diagram of molnupiravir mechanism of action.
Clinical trials evaluating the efficacy of molnupiravir therapy and the existence and prevalence of treatment-related adverse events have been reported. In MoveOut, a phase II and III clinical trial, molnupiravir showed effectiveness in the analysis comparing the groups treated with 200, 400, or 800 mg of molnupiravir to the placebo group; the percentage of patients whose clinical condition progressed to hospitalization or death within 29 days of symptom onset was 7.3% in the treated group and 14.7% in the placebo group. Furthermore, it was observed that the treated group showed improvement in oxygen saturation 3 days after the treatment started and no death was reported, while patients receiving placebo reported improvement only 10 days later and eight patients died (Jayk Bernal et al, 2022; Johnson et al, 2022).
In addition, Painter et al (2021) reported few treatment-related adverse effects. None of the patients experienced severe adverse effects, and headache among subjects who received a single dose of the drug (12.5% of subjects included) was the most common adverse effect observed; in this group, only 2 of 64 individuals had a moderate adverse effect (scale 2). Regarding the group that received multiple doses of molnupiravir, 56 (7.1%) patients experienced diarrhea; however, in general, patients receiving a placebo presented more adverse events than patients receiving single or multiple doses of the drug.
Given the mutagenic nature of the drug and its intracellular action, the possibility of incorporation and intracellular action of the compound in the host cell was studied. However, no clinical trial obtained results that demonstrated the occurrence of mutations in the host and, therefore, the drug was considered safe (Saravolatz et al, 2022). Nonetheless, according to the FDA recommendation, because the effectiveness of this drug in treating coronavirus infection was ∼30%, the lowest observed in clinical trials, its use is recommended only when there is contraindication or ineffectiveness of other available pharmacotherapeutic measures, such as Paxlovid and remdesivir (https://www.covid19treatmentguidelines.nih.gov/therapies/antiviral-therapy/molnupiravir/and https://www.fda.gov/media/155054/download).
No clinical trial evaluating the use of molnupiravir indicated that factors such as gender, age, ethnicity, and the individual's genetic variants influenced treatment efficacy. Nonetheless, the clinical trials reviewed in this study did not evaluate patients younger than 18 years and most individuals were self-reported white (Jayk Bernal et al, 2022; Painter et al, 2021). Also, it was observed that this drug is not metabolized or alters the enzymatic activity of cytochrome p450 complex enzymes, but as already discussed by Al-Taie et al (2022), the available results are scarce and further research is needed to decipher the genetic and environmental determinants of safety and efficacy as the studied concentrations do not match the indicated dosage.
According to Wang et al (2021), treatment prescriptions for COVID-19 should consider the patient's genetic differences, ethnicity, and disease severity status, thereby providing individual, safer, and more effective treatment. Furthermore, clinical trials must consider such factors in their design to better evaluate the safety and efficacy of remdesivir, Paxlovid, and molnupiravir.
Final Considerations
Remdesivir showed effectiveness in the treatment of COVID-19. The response to treatment, however, appears to show interethnic variability. It is hypothesized that this may be, at least partly, accounted for by candidate biomarkers such as the CYP2C19, CYP2D6, and CYP3A4 genes. According to in vitro studies, such genes are associated with remdesivir metabolism, and variant frequencies vary among different populations. This is of utmost importance, given the relevance of pharmacogenomics in the context of theranostics and, therefore, precision medicine. Besides remdesivir, Paxlovid and molnupiravir are potential drugs being evaluated for COVID-19 treatment regarding safety and effectiveness.
Nonetheless, clinical trials evaluating candidate drugs to treat COVID-19 must include diverse populations and ethnicities in their studied sample, besides including pharmacogenomic analysis. It is crucial to maximize efficacy and minimize potential adverse effects, and thus ensure that treatments employed for treating COVID-19 will be as safe and effective as they could be for all people worldwide. By addressing these challenges, we will walk toward achieving theranostic's promises and precision medicine's goal.
Footnotes
Authors' Contributions
The authors confirm contribution to the article as follows: conceptualization: F.R.-S. Data collection: C.M., S.T.-L., B.M., and F.C.S.-S. Writing—original draft: C.M., S.T.-L., B.M., and F.C.S.-S. Writing—review and editing: M.M.S. and F.R.-S. All authors made a significant intellectual contribution and approved the final version of the article.
Acknowledgments
We thank the Population Genetics and Pharmacogenetics research group for the valuable discussions. F.R.-S. is supported by the National Council for Scientific and Technological Development—CNPq.
Author Disclosure Statement
The authors declare they have no conflicting financial interests.
Funding Information
This research received no specific grant from any funding agency.