
Abstract
Introduction
Treatment regimens reflect the multifactor nature of the condition and include antifungal therapy, provision of new dentures, and maintenance of good denture hygiene and removal of dentures for sleeping. Different treatment methods have been suggested to treat this type of stomatitis. Topical nystatin, amphotericin B, miconazole, and systemically administered fluconazole have been used in the management of DS, but all have been associated with a high rate of relapse. 6
A potential noninvasive treatment for DS patients is laser phototherapy (LPT). In recent studies, many authors have reported a significant reduction in pain and inflammation with LPT for radiotherapy-induced oral mucositis and xerostomia in oral-cancer patients, 7 –9 and a reduction in severe pain in patients subjected to hematopoetic stem-cell transplantation. 10,11
Proinflammatory cytokines such as tumor necrosis factor-α (TNF-α) and interleukins are important mediators of inflammation, immunity, proteolysis, and cell recruitment and proliferation. TNF-α is a multifunctional cytokine that plays a prominent role in immune and host defense responses to infection. 12 It stimulates angiogenesis, 13 influences tissue remodeling, 14 and takes part in the regulation of cell proliferation and differentiation. It has been identified as an important mediator of cancer development 15 and a powerful activator not only of apoptotic but also anti-apoptotic signaling cascades. 16
Interleukin-6 (IL-6) is known to be a proinflammatory cytokine, and it may be produced by various activated cells, including monocytes, macrophages, endothelial cells, fibroblasts, keratinocytes, and T and B lymphocytes.
Saliva has been widely used in disease monitoring and the detection of various oral and systemic diseases. 17 In our previous investigation, we found that TNF-α can be detected at significantly higher levels in saliva from patients with oral lichen planus. 18 Our analysis has also shown that saliva has been successfully used in the detection of IL-2 and IL-6 in patients with burning mouth syndrome. 19
The aim of this study was to monitor therapeutic response by determining the level of proinflammatory cytokines TNF-α and IL-6 in whole unstimulated saliva in patients with DS, before and after LPT.
Materials and Methods
A sample consisting of 40 consecutive subjects was selected on a voluntary basis from patients who presented for the diagnosis and treatment of DS at the Oral Medicine Unit of the Medical Faculty at the University of Rijeka. Demographic characteristics are shown in Table 1. All subjects were informed of the aims and procedures of the research, as well as the fact that their medical data would be later used in the analysis. The Ethics Committee of Medical Faculty of Rijeka (University of Rijeka) approved this study protocol. Only those subjects who gave written permission in the form of an informed consent were included. Each subject completed a questionnaire for demographic and health information.
A clinical examination was performed according to the standard clinical criteria. The clinical conditions of the palatal mucosa were evaluated using Newton 20 criteria: 0, no inflammation; 1, pin-point hyperemia; 2, diffuse erythema; and 3, papillary hyperplasia. Lesions described as palatal inflammation were diagnosed as Newton type II denture stomatitis. After initial evaluation and diagnosis, the patients were divided in two groups: group 1 – 20 patients receiving real LPT (experimental group); group 2 – 20 patients receiving inactive/placebo laser treatment (control group).
Whole unstimulated saliva was collected between 9:00 and 11:00 a.m. using standard techniques described by Navazesh. 21 Participants refrained from eating, drinking, using chewing gum, etc, for at least an hour-and-a-half prior to evaluation. Saliva specimens were collected in the sitting position from each participant of both groups, before and after LPT. Samples were obtained by requesting subjects to swallow first, tilt their head forward, and expectorate all saliva into 50-mL tubes for 5 min without swallowing. The final volume and flow rate of saliva were determined gravimetrically (Analytical Balance, Model WTS-6001, Sartorius Corp., Long Island, NY). 22 The entire procedure was repeated after the final treatment, 4 wk later.
Saliva specimens were stored at −80°C until the beginning of analysis. For determination of salivary levels of TNF-α and IL-6, ELISA (Sigma Immunochemicals, St Louis, MO) was performed. Assay was performed according to the manufacturer's instructions, and the results are expressed in pg/ml. The test was performed in duplicate and repeated three times. Protein content was expressed in pg/ml. Elutions were performed at 4°C over a 30-min period, with mixing before centrifugation for 2 min at 9880g. Standard human TNF-α and IL-6 ELISA kit and eluted saliva samples were applied to 96-well microtiter plates. All tests were performed in duplicate, repeated three times, and assayed according to ELISA procedure as follows: (1) 50 μL of assay diluents IF(D-1550) was added to each well; (2) 200 μL of sample was added per well, covered with the provided plate cover (C-5697), and incubated for 1 h in the shaker (Red rotor Hoefer Pharmacia Biotech, Inc., San Francisco, CA); (3) 200 μL of TNF-α and IL-6 conjugate was added, covered with a new plate cover, and incubated for 1 h in the shaker; (4) substrate solution was prepared by mixing equal volumes of color reagent A and color reagent B; (5) 200 μL substrate solution was added to each well and incubated for 20 min at room temperature; (6) 50 μL of stop solution (S-0416) was added to each well and gently mixed; and (7) optical densities (OD) of individual wells were obtained spectrophotometrically (450 nm) within 30 min. Using standard dilution concentrate and OD, a standard curve was prepared for each plate, and the amount of TNF-α and IL-6 (units/μL) was calculated by linear regression analysis for each saliva sample.
The 20 subjects in the experimental group were treated for 5 d a week for four consecutive weeks with a 685-nm GaAlAs (Gallium Aluminum Arsenide) diode laser (Medio LASER Combi Dental, Iskra Medical, Ljubljana, Slovenia). The 20 patients in the control group were also treated for four consecutive weeks but with an inactive (placebo) laser. The output power of the laser was measured every 7 min and found to be practically constant. The laser output power was controlled weekly using analogue power meters provided by the manufacturer. The laser light was delivered through an optical fiber (flexible fiber bundle with 2-mm circular aperture), and the output power was measured at the fiber aperture. The laser treatment was performed by holding the laser probe in light contact with the tissue. During each session, the laser treatment was delivered to the tissue by a straight optical fiber with a 2-mm spot size. The treatment areas, each being 1 cm2, included palatal mucosa. Laser was applied on palatal mucosa for 10 min (685 nm, continuous wave, 30 mW output power, 3.0 J/cm2). The treatment time (t) for each application point was given by the equation: t (s) = 3, 0 J/cm2 × 1 cm2/0, 03 (W). The laser treatment was performed in a punctual mode for 100 s per point. The average energy density delivered to the treatment areas was 3.0 J/cm2. The effect of laser light was evaluated after the final treatment. For the placebo group, the laser device was adjusted for the same time and applied to the same points, but without power.
Statistical Analysis
Statistical analysis of the data was performed using Statistica for Windows, release 7.1 (StatSoft, Inc., Tulsa, OK). Data of TNF-α and IL-6 were presented as the mean ±standard deviation. A t-test for dependent samples was used to compare the differences of both cytokine levels before and after treatment. The analysis of the differences, for both cytokine levels, between treated and control group was performed using a t-test for independent samples. All statistical values were considered significant at p < 0.05.
Results
Following treatment with LPT for 4 wk, the levels of TNF-α and IL-6 were measured in whole saliva samples using ELISA. Levels of TNF-α measured before LPT were significantly greater than TNF-α levels following therapy. Levels of IL-6 before LPT were also significantly greater than subsequent IL-6 levels (p < 0.001), and the levels of these proinflammatory cytokines were significantly different from controls (p < 0.001) (Table 2, and Figs. 1 and 2). The average age of patients in the experimental group was 60.5 ± 6.4 and 58.8 ± 5.8 years in control groups (p = 0.505). There was no difference in sex between the experimental group and the controls (p = 0.744).
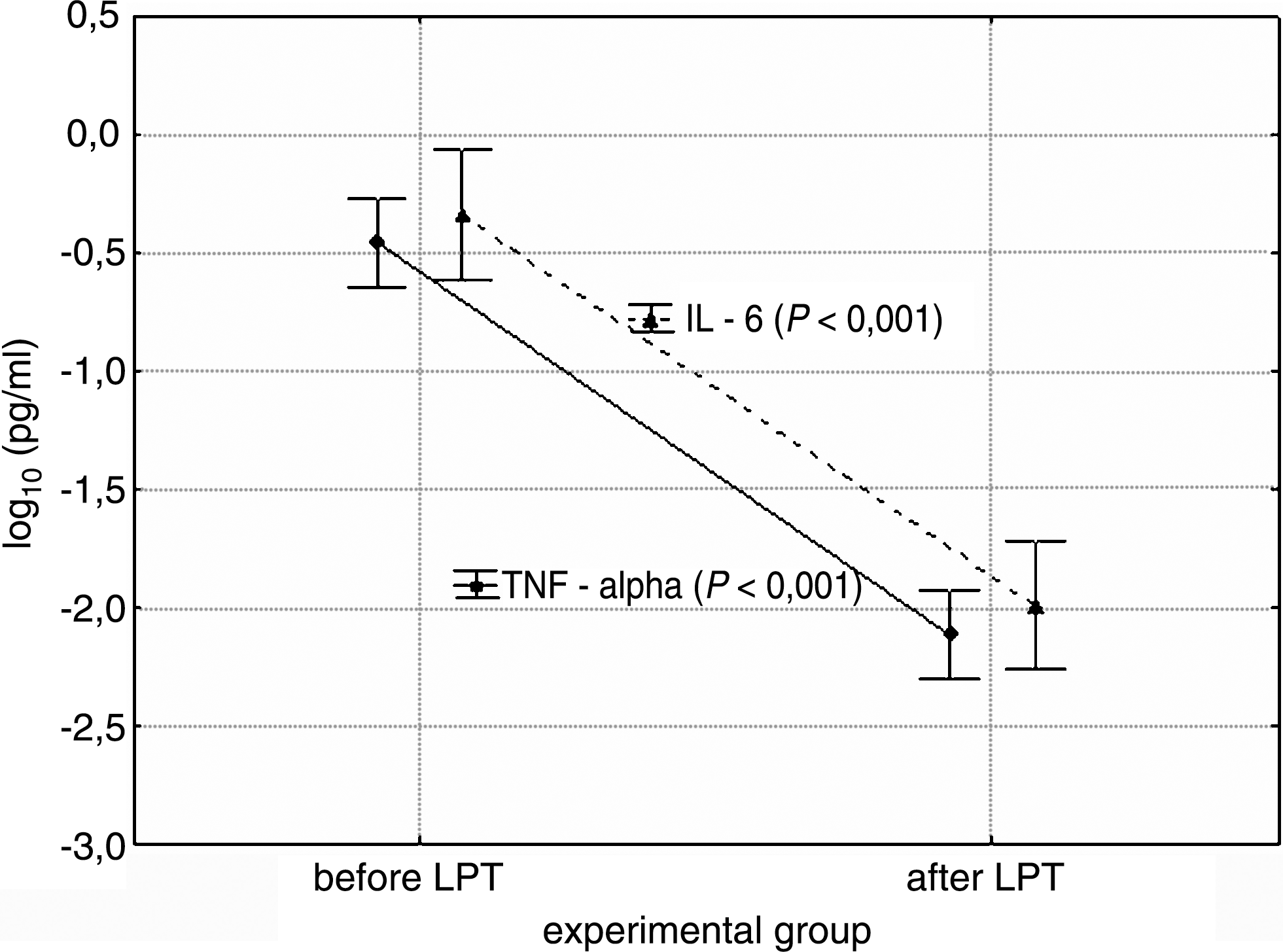
Graphic representation of detected values of TNF-α and IL-6 before and after LPT in the experimental group.

Graphic representation of detected values of TNF-α and IL-6 in the control group.
Discussion
LPT has been successfully applied to various painful oral mucosal diseases, although there have been few reports on LPT for DS patients. LPT is a noninvasive, quick, and safe nonpharmaceutical intervention that may be beneficial for patients with DS. A number of studies have compared the biological effect of coherent and incoherent light, and all of them indicate that the effect of light from lasers is superior to noncoherent light. 23
Saliva has some obvious advantages compared with blood-based analyses, such as easy access and non-invasive collection, and because of that oral fluids have been widely used in drug and disease monitoring and the detection of various and systemic maladies. 24 The significant increase in salivary TNF-α and IL-6 in patients with DS compared with normal controls may be due to local and systemic production of TNF-α by various cell types. TNF-α can be secreted by monocytes, macrophages, T and B lymphocytes, natural killer cells, endothelial cells, mast cells, fibroblasts, Langerhans cells, and keratinocytes. TNF-α can induce the secretion of IL-6.
In this preliminary study, with a small sample size, we found a statistically significant reduction in the salivary levels of the proinflammatory cytokines TNF-α and IL-6 in patients with DS following treatment for 4 wk with LPT. These results were supported by clinical changes. At the end of the study, the clinical conditions of the control group were the same as at the beginning of the study. In contrast, in the experimental group, the clinical conditions of the palatal mucosa showed an improvement. Correlations between TNF-α and IL-6 in the control group and clinical conditions were not statistically significant. The reasons why treatment with LPT can reduce the salivary TNF-α and IL-6 in patients with DS are not clear.
A study performed by Maver-Bišćanin et al. 25 showed that LPT may be valuable in the treatment of DS. In their investigation, LPT showed a significant antifungal effect that was more characteristic on the denture than on the palate. In contrast, some investigators claim that microbial cells in general are transparent to visible light produced by low-power lasers and are not affected by such radiation. 26 There is insufficient evidence either for or against the use of LPT for the treatment of DS and the effect on proinflammatory cytokines.
Whilst many authors presented opposite results for the effectiveness of laser in the treatment of pain or inflammation, the majority of studies (about 85%) demonstrate that the reduction of pain is effective. 27 Some studies, like that by Šimunović, 28 presented a reduction in tissue inflammation or a direct effect on nerve tissues. The doses used in this research are different, making comparisons difficult and limiting any conclusions. The most recent studies describe their methods, but they do not give a complete description for the choice of the dosage parameters. The recommendations are primarily based on positive clinical experience rather than classical placebo-controlled clinical trials. 27
We choose a 685-nm wavelength because beneficial results have been achieved at this wavelength in earlier studies. 29 We used 20 sessions and this represents a clinically reasonable number of treatments and reflects a consensus among laser-therapy clinicians and researchers that successful treatment typically requires multiple treatments. 29
Conclusion
LPT is a noninvasive, quick, and safe nonpharmaceutical intervention that may be beneficial for patients with DS. In the present study, LPT resulted in a significant decrease in salivary TNF-α and IL-6 in patients with DS. Based on the presence of TNF-α and IL-6 in whole saliva, we think that saliva analysis is useful. Salivary TNF-α and IL-6 are important indicators, showing a statistically significant difference before and after laser therapy. Our results may suggest that LPT may be an efficacious choice of therapy in patients with DS.
Footnotes
Acknowledgments
This research was supported by a grant from the Ministry of Science and Technology (062-0650444-0442), Republic Croatia.
Author Disclosure Statement
No competing financial interests exist.