
Abstract
The common consequences of radiotherapy (RT) to the head and neck are oral mucositis, xerostomia, and severe pain. The aim of this study was to verify how laser phototherapy (LPT) used for oral mucositis could influence xerostomia symptoms and hyposalivation of patients undergiong RT. Patients were divided into two groups: 12 individuals receiving three laser irradiations per week (G1) and 10 patients receiving one laser irradiation per week (G2). A diode laser (660 nm, 6 J/cm2, 0.24 J, 40 mW) was used until completely healing of the lesions or the end of the RT. At the first and last laser sessions, whole resting and stimulated saliva were collected, and questionnaires were administered. According to Wilcoxon and Student statistical test, xerostomia for G1 was lower than for G2 (p < 0.05), and salivary flow rate was no different before and after RT, except for stimulated collection of G2, which was lower (p < 0.05). Our results suggest that LPT can be beneficial as an auxiliary therapy for hypofunction of salivary glands.
Introduction
Radiotherapy (RT), medication, immunological and rheumatic diseases, 2 and some genetic disorders such as Down Syndrome 3 cause a marked reduction in salivary flow rate. 2,3 Radiation effects on salivary glands are of particular interest in clinical RT of head and neck tumors, where the reduced flow rate and the altered composition of saliva result in distress, oral dryness, hampered oral functioning, nocturnal oral discomfort, burning mouth, impeded social activities, and a susceptibility to oral infections and dental caries. 4 –6 Saliva turns into a white, yellow, or brown viscous fluid, with reduced pH and buffering capacity and altered salivary electrolyte. 6
Wetting agents or saliva substitutes have a palliative effect but are not well accepted by patients. 7 Therapies for hyposalivation also include systemic sialagogues, which stimulate salivary flow rate, but they can be associated with side effects. 8,9
Ionizing radiation may affect the secretory salivary gland cells, the blood supply and the nerves. 6 Secondary complications related to hyposalivation include difficulty speaking and chewing, deglutition, reduction of the taste, mucositis, opportunist infection, fungal infection, and fast progression of caries. It is important to highlight that pain and discomfort associated with hyposalivation and mucositis may affect these patients' quality of life, 10 –12 and they are associated with greater morbidity in addition to significant additional hospital costs. 13,14
Oral mucositis is the name given to ulcerations in the oral cavity as a consequence of the cytotoxic effects of RT or chemotherapy. Strategies to reduce oral mucositis to address this serious impediment to cure have proven to be inadequate, leaving an important unmet medical need. Recently, laser phototherapy (LPT) has been used because of its potential to induce basic biological effects, such as tissue biomodulation, analgesia, and modulation of the inflammatory process. 15 –20
The effect produced by LPT is based on the capacity of modulation of diverse metabolic processes through the conversion of light energy in biochemical and photophysical processes, which transforms laser light into useful energy for cells. 21 Chromophores in the respiratory chain of the mitochondria absorb visible laser light, which causes an increment in adenosine triphosphate production, resulting in an increase in cellular proliferation and protein synthesis. 21
In addition to the basic effects of LPT on patients with oral mucositis, improvement of xerostomia after LPT has also been reported in the literature. 10,11,22 Cowen et al. reported improvement in saliva production and the ability to swallow in patients with cancer who received red LPT (1.5 J/cm2, 60 mW). 22 Our previous studies demonstrated that infrared LPT, in doses of 4 and 8 J/cm2, can stimulate salivary glands of rats 23 and increase total protein concentration in the parotid glands. 24 In addition, an improvement in xerostomia symptoms of a patient diagnosed with Sjögren's syndrome was also observed. 25
Based on all data and information available, the purpose of the present study was to analyze the effect of LPT on salivary flow rate, xerostomia symptoms, and saliva composition of oncologic patients undergoing RT for cancer treatment and LPT for oral mucositis.
Materials and Methods
Patients
A prospective study was conducted at the Special Laboratory of Lasers in Dentistry (LELO) from November 2005 to March 2008. Twenty-two patients with head and neck cancer undergoing RT treatment (cobalt machine, gamma radiation) in which the radiation field reached the major salivary glands were selected. Patients were referred to LELO from the Instituto do Câncer Arnaldo Vieira de Carvalho (Santa Casa). Approximately 90% of patients were diagnosed with squamous cell carcinoma; the main locations were the pharynx (40%) and tongue (25%).
Ethical considerations
The local ethics committee approved the protocols for this study, and written informed consent was obtained from all patients. The care of the patients throughout the study period was conducted in accordance with the principles of the Helsinki Declaration of 1975, as revised in 2000.
Clinical procedures
Patients were divided into one group irradiated three times a week (G1, n = 12) and one group irradiated once a week (G2, n = 10), according to Simões et al. 26 Table 1 shows the characteristics of the patients in each group. The RT was bilateral, with total dosing over 60 Gy. The subjects' mean age was 51 for G1 and 48 for G2. Each patient underwent a complete oral examination with a subsequent treatment plan formulated to include oral care guidelines. (After receiving a kit containing a tooth brush, tooth paste, and an alcohol-free mouthwash, the patients received hygiene orientation.) Oral and dental infections and focus were identified and treated.
For the total group.
During clinical examination, the medical history of each patient was recorded. Data related to patient age, sex, diagnosis, coexisting chronic diseases, type and stage of RT treatment, and whether they were receiving chemotherapy were collected.
Laser phototherapeutic trials
Two laser phototherapeutic protocols were used. Two trained dentists performed laser irradiations. Radiations was administered three times (G1, n = 12) or one time (G2, n = 10) per week using a low-power laser.
The therapeutic protocols were initiated at the first visit (within 14 days after the first RT session) and ended when any signs of oral mucositis had disappeared.
An aluminium gallium indium phosphide diode laser (Twin Laser, MMOptics Ltda, São Carlos, SP, Brazil) with a wavelength of 660 nm was used, according to Campos et al. 10 and Eduardo et al. 15 The irradiation mode was punctual and in contact, perpendicular to the oral mucosa. The power used was 40 mW, energy density of 6 J/cm2, energy per point of 0.24 J, and total energy per session of approximately 21 J. Irradiation time was 6 s per point based on the laser beam spot size of 0.036 cm2. Irradiations were done intra-orally, avoiding the tumor site, as follows: 12 points on each buccal mucosa (right and left), eight on the superior and inferior labial mucosa, 12 on the hard palate, four on the soft palate, 12 on the lingual dorsum, six on the lateral edge of the tongue bilaterally, two on the right and left pillar of the tongue, four on the floor of the mouth, and one in the labial commissure, bilaterally.
For all therapeutic protocols, before and after each session, power output was checked using a power meter (Coherent Molectron, Santa Clara, CA). The laser irradiations were administered following biosafety rules.
Saliva collection
Stimulated and unstimulated saliva were collected at the first and last laser session, always in the morning (between 8 a.m. and 11 a.m., to minimize the circadian effects of salivary glands) after at least 1 h of fasting. The patient was comfortably seated in a ventilated and lighted room, without interference from the external environment, for the saliva collection.
First, unstimulated saliva collection was performed. For resting saliva, the patient was requested to sit quietly; tilt the head slightly down; keep the eyes open; and not move the lips, tongue, cheeks, or any other body part. Immediately before the test, the patient swallowed any saliva in the mouth and then started to expectorate the saliva that was spontaneously produced into a plastic funnel that was connected to a plastic tube. The time of the collection was 10 min.
The stimulated saliva was collected using a solution of citric acid swabbed on the dorsum of the tongue every 30 s for 5 min. Immediately before the test, the patient swallowed any saliva in the mouth and then started to expectorate the saliva that was produced into another plastic funnel that was also connected to a plastic tube.
The saliva was gathered in a container, kept in crushed ice, and immediately taken to the Oral Biology Research Center, where the samples was centrifuged at 2000 × g for 10 min. The volume of saliva was measured and the flow rate calculated, and then the samples were classified, frozen, and stored at −80°C until the biochemical analysis was performed.
Subjective method of xerostomia analysis (questionnaires)
The xerostomia symptom (dry mouth) was registered and evaluated subjectively through questionnaire applications such as the Xerostomia Inventory (XI), 27,28 Visual Analog Scale (VAS), 29 and Treatment-Emergent Symptom Scale (TESS). 30
The XI has 11 items referring to diverse xerostomia-associated symptoms (e.g., “I get up at night to drink,” “I sip liquids to aid in swallowing food,”) and the patients replied to the questions in accordance with the frequency that they happened (never, hardly ever, occasionally, frequently, always), with higher scores (frequently and always) representative of more-severe symptoms.
A VAS containing five items was used to measure symptom intensity, allowing patient to identify their condition related to deglutition and speaking difficulty, as well as the amount of saliva and oral dryness, indicating values between 0 and 10; the higher the number, the worse the xerostomia symptom. 29
According to the TESS questionnaire, the symptom of dry mouth is classified into grades 0, 1, 2, 3, and 4, in which 0 is no dry mouth symptoms, 1 is light dry mouth symptoms at night and immediately after waking up, 2 is light dry mouth symptoms all time, 3 is moderate dry mouth symptoms with some functional impairment, and is 4 severe dry mouth, with impairment of quality of life, swallowing difficulty, and the need to drink water all the time. 31
Salivary analysis
The salivary flow rate was expressed as mL/min and was calculated using the relationship between the volume of saliva collected and collection time. Protein concentration was determined using the method of Lowry et al., using bovine albumin as the standard. The readings were made at 660 nm in a Beckman DU-68 spectrophotometer (Fullerton, CA). 32
Sialic acid (free and total) concentration was determined using a thiobarbituric acid assay as described elsewhere. 33,34 Briefly, total sialic acid was determined after hydrolysis in 0.1N sulfuric acid at 80°C for 1 h. Samples were then treated with periodate reagent (25 mm of periodic acid in 0.125N sulfuric acid) and incubated at 37°C for 30 min. The reaction was terminated by adding sodium arsenite (2% sodium arsenite in 0.22M hydrochloric acid). After the iodine color disappeared, a solution of thiobarbituric acid (0.1M, pH 9.0) was added. The solution was heated in boiling water for 7.5 min and cooled. Dimethyl sulfoxide was added, and the intensity of the developing color was measured at 549 nm in a Beckman DU-68 spectrophotometer. The levels of free sialic acid in all samples were determined following the same steps, except for the hydrolysis of the sample. The difference between total and free sialic acid was expressed in the results as μg/mL.
The concentration of alpha-amylase and the activity of peroxidase were determined as described elsewhere. 24 For the determination of amylase activity, samples of saliva were incubated with 1% starch solution in 20 mM phosphate buffer, pH 7.0, for 5 min at 37°C. The reaction was interrupted by adding an alkaline solution of dinitrosalicylic acid, and the mixture was maintained in boiling water for 5 min. After dilution of the mixture with distilled water, the intensity of the developed color was measured at 530 nm in a Beckman DU-68 spectrophotometer. Peroxidase was measured on medium containing 10 mM phosphate buffer, pH 6.0, 10 mM o-dianisidine, 2.1 mM hydrogen peroxide (H2O2), and saliva samples. The absorbance was measured at 460 nm. A solution of lactoperoxidase was used as a standard.
The catalase activity was assayed in medium containing 50mM phosphate buffer, pH 7.0, supernatant, and 100 mM H2O2. The catalysis of H2O2, observed spectrophotometrically, was shown as the decrease in absorbance at 240 nm. The difference in absorbance per unit time was the measurement of the catalase activity. 35
Statistical analysis
The Wilcoxon statistical test was used to analyze subjective results, and the Student t-test was performed to compare quantitative data for both groups, setting the level of significance at 5%.
Results
Twenty-two patients were included in the statistical analysis; all of them had received RT for head and neck cancer, with the field of irradiation encompassing bilaterally the major salivary glands. Patient characteristics are summarized in Table 1. There were seven women (32%) and 15 men (68%), with a mean age of 51 for G1 (range 15–79) and 48 years for G2 (range 19–63). Hypertension was the most prevalent coexisting chronic disease. Forty percent of patients from G1 and 10% of patients from G2 were treated with concomitant chemotherapy; 58% of patients from G1 and 70% of patients from G2 underwent surgery followed by RT. The mean total dose was 66 and 65 Gy (range 60–70 Gy) for G1 and G2, respectively.
Xerostomia questionnaires
The results for all of the questionnaires showed that the symptoms of xerostomia decreased significantly for G1 after LPT (p < 0.05) (Fig. 1). For G2, only the XI showed a significant decrease in xerostomia symptoms after LPT (p < 0.05) (Fig. 2).
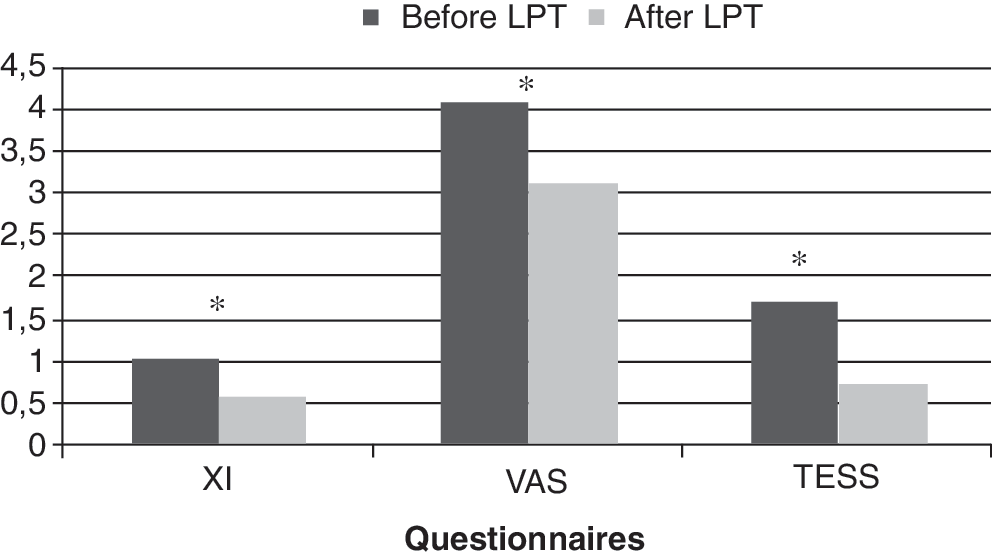
Subjective analysis of group 1. *Indicates that the answers of the specific questionnaires were different before and after LPT (p < 0.05).

Subjective analysis of group 2 before and after laser phototherapy. *Indicates that the answers of the specific questionnaires were different before and after LPT (p < 0.05).
Saliva collection
Unstimulated salivary flow rate (whole resting saliva; WRS) values revealed no statistically significant difference for either group before and after laser phototherapy (LPT); nevertheless, the flow rate of stimulated saliva (whole stimulated saliva; WSS) of G2 decreased significantly (p < 0.05) after LPT (from 0.66 to 0.40 mL/min) (Table 2).
Statistically significant difference considering the same group [group 1 (G1) or group 2 (G2)]. Numbers of samples are in parentheses.
Salivary biochemical analysis
Amylase content increased (p < 0.05) in G1 (216% for WRS, 333% for WSS) and G2 (400% for WRS, 450%, for WSS) (Table 2). Regarding, it showed There was an increase in the difference between total and free sialic acid in G1 (213% for WRS, 256% for WSS) and G2 (369% for WRS and WSS) (p < 0.05) (Table 2).
There were no significant differences in peroxidase or catalase after LPT in WSS and WRS for either groups, whereas protein concentration decreased (p < 0.05) in WRS for G1, although not statistically significantly so (p > 0.05) (Table 2).
Discussion
Until now, therapy for oral mucositis has been based on oral care, biological mucosal protectants, analgesics, antibiotics, growth factors and cytokines, antiinflammatory agents, and complementary and alternative medicines; 36 recently, LPT has been introduced. This investigation showed that LPT used to treat oral mucositis can be effective in easing xerostomia symptoms during RT.
Radiation-induced xerostomia is the most prevalent and prominent long-term side effect in patients after therapeutic radiation of tumors in the head and neck region, and it is usually related to a decrease in the patient's quality of life. 6,12 Moreover, deterioration of salivary function leads to a loss of taste acuity and to the reduction of salivary flow rate. 6 In addition, the increase in saliva viscosity can interfere with prosthetic rehabilitation efforts and also with deglutition, impairing the patient's appetite and leading to weight loss and immune suppression. 6 In this sense, a therapy capable of stimulating the production of saliva or of modifying saliva composition would be useful.
Studies have shown that LPT is an efficient treatment for oral mucositis in patients undergoing RT or chemotherapy. 10,15,20,36 –38 Moreover, other studies have shown that oncology patients undergoing LPT (1.5 J/cm2, 60 mW) to treat oral mucositis reported an improvement in saliva production and the ability to swallow. 22 In addition, our previous investigations demonstrated that LPT was able to stimulate salivary glands 23 and increase total protein concentration in the parotid glands of rats. 24 In humans, we also observed salivary gland stimulation and improvement of xerostomia symptoms of a patient with Sjögren's syndrome (data not shown).
In the present in vivo study, we used the combination of objective (measurement of salivary flow rate) and subjective (questionnaires) parameters to examine patient complaints about salivary dysfunction. 6 In addition, saliva composition and the activities of some enzymes were also performed for oncology patients receiving LPT.
Concerning the subjective analysis, the patients who received laser irradiation three times per week (G1) showed better results related to xerostomia symptoms than the individuals who received it once per week (G2), although 40% of the patients in G1s and 10% of patients in G2 were treated with concomitant chemo-RT. According to the literature, salivary gland damage due to RT doses lower than 30 Gy are reversible, whereas cumulative doses higher than 75 Gy cause extensive degeneration of acini, inflammation, and fibrosis in the interstitium, resulting in irreversible injuries. 39 The patients in the present study received approximately 70 Gy, and still G1 showed decreased xerostomia symptoms according to all questionnaires applied.
Regarding the objective analysis, although a drastic reduction in salivary flow rate was expected for both groups because patients were receiving ionizing RT, the salivary flow rate decreased statistically in comparison with the initial measurement only for stimulated saliva of G2 (laser once per week). On the other hand, although the salivary flow rate decreased for G1, it was not statistically significant, suggesting a biomodulatory action of LPT on the salivary glands, stimulating its proliferation to replace the secretory cells damaged by RT.
The present study also showed that RT affected stimulated saliva, which is secreted mainly by the parotid glands, more than unstimulated saliva, reflecting the inability of the irradiated glands to increase their production after stimulation. 40 –42 Parotid glands are more radiosensitive once they are compounded mainly of serous acinar cells, which are more affected by radiation than mucous or ductal cells. 6,43 However, other authors did not agree that submandibular glands are less radiosensitive than the parotid glands. 6 In the present study, we observed an increase in salivary α-amylase concentration during RT. α-amylase is a metallo-enzyme, a biomarker of parotid salivary glands, 44 which catalyzes the hydrolysis of glycosidic linkages in starch. 45 This result is contradictory with previously published data. 5,6
According to the conditions applied in this study, the patients who received laser irradiation three times per week (G1) did not show a significant decrease in salivary flow before and after LPT, even when the collection was done through stimulation of the salivary glands.
RT results in a change in saliva quality and in its composition. 5,6 The reason why the decrease in xerostomia symptoms in the present study can be related to modification of saliva composition is that the salivary flow rate was not increased. To obtain some important data, we examined some biochemical assays in the saliva of the patients analyzed.
Like the current investigation, only a few studies relating the effect of RT on the salivary gland parameters have been conducted. 5,46 In this sense, in the present study, there was difficulty in separating the effect of the laser and the ionizing radiation on salivary gland composition.
In the present study, the most significant differences found between these biochemical parameters was the increased sialic acid and amylase concentration in WRS and WSS after the LPT. However, these increases were less evident in the group in which individuals underwent laser irradiation three times per week (G1). We suggested that the decrease of xerostomia symptoms is related to acid sialic results, which is linked with saliva viscosity.
There was no significant difference between the groups in antioxidant enzymes peroxidase and catalase. On the other hand, protein concentration was decreased after LPT in all groups, being more pronounced in WSS of G2. Others authors have also reported a decrease in total protein concentration, which reflects the impairment of synthesis and secretion of salivary glands, when they are exposed to ionizing radiation. 5
More studies are necessary to confirm that LPT can be used as an auxiliary therapy in cases of salivary gland hypofunction. In this work, we analyzed whether LPT used for oral mucositis treatment could alter salivary flow rate and salivary composition, modifying xerostomia symptoms. Further studies are necessary usinga specific LPT protocol related to salivary gland areas.
Conclusion
The results of this study suggest that LPT could be a therapy to stimulate salivary glands and to decrease xerostomia symptoms in an attempt to improve patient quality of life during RT, although more studies are necessary.
Footnotes
Acknowledgments
The authors wish to express their gratitude to the Laboratório Especial de Laser em Odontologia, the Fundação do Amparo a Pesquisa do Estado de São Paulo (Grant 05/57578–8), and the Universidade de São Paulo for their financial support.
Author Disclosure Statement
No competing financial interests exist.