
Abstract
Introduction
Our group has developed a simple, easily performed procedure for covering full-thickness excisional skin wounds in diabetic mice. 3 Covering wounds with a Tegaderm HP film dressing and using an adhesive agent led to a very high proportion of wounds in diabetic mice showing a retardation of contraction and hence wound splinting. 3 Splinted wounds healed mainly by re-epithelization and granulation tissue formation. This preliminary study was undertaken to test the effects of two regimens of laser irradiation (660 nm) on a murine model of diabetic-impaired wound healing in which wounds were covered with a Tegaderm HP dressing.
Materials and Methods
Mice
Diabetic and non-diabetic litter mates (BKS.Cg-m+/+Leprdb /J, The Jackson Laboratories, Bar Harbor, ME, USA, stock #000642) were used from a small breeding colony at the University of Otago. Diabetic mice were selected on the basis of age and body weight: the majority were 11–16 weeks and at least 40 g. Non-diabetic mice were similarly selected: most were 14–16 weeks and at least 27 g. Both males and females were included. Diabetic mice are leptin receptor deficient and represent a model of type-2 diabetes characterized by hyperglycemia, obesity, and impaired wound healing. 4 Non-diabetic mice are lean, and wound healing is not impaired.
Prior to surgery, animals were housed together according to date of birth and sex, and post-surgery in individual cages. The experimental protocol was approved by the Animal Ethics Committee, University of Otago.
Experimental wound model
All mice received atropine 0.05 mg/kg body weight subcutaneously at least 10 minutes before inducing anaesthesia with halothane to provide cardiorespiratory protection. Mice were anaesthetized with halothane (4% induction, 2% maintenance). The left flank was shaved, using Veet cream (Reckitt Benckiser, West Ryde, New South Wales, Australia), and the skin disinfected with betadine. A full-thickness circular wound was made on the left flank in each mouse using a sterile 5 mm diameter skin punch. The wound extended down to the fascial layer over abdominal musculature. Wounds were covered with Tegaderm HP (3 M New Zealand, Inc., Auckland, New Zealand), and Temgesic (buprenorphine) 0.1 mg/kg body weight given subcutaneously for pain relief. Mice were returned to their cages and kept warm by placing the cage on a heating pad until fully recovered from the anaesthetic. Day 1 was defined as the day of wounding. All steps involved in creating and covering wounds were performed by the same operator to minimize variability. The depth of the wounds was confirmed by histological sections of skin excisional samples collected at surgery. 3 The total number of animals used was 47 diabetic (22 males, 25 females) and 20 non-diabetic (18 males, 2 females) mice.
Method of attaching Tegaderm dressing over the wound
Based on a preliminary study, the first Tegaderm HP dressing (3 M New Zealand, Inc., 25 × 25 mm) was attached using Cavilon No Sting Barrier Film (3 M) and two Fixomull Stretch strips (BSN Medical GmbH, Hamburg, Germany, 6–7 × 30–35 mm), the second dressing using Mastisol (Ferndale Labs, Ferndale, MI, USA), and the third and any subsequent dressings using Mastisol with or without Fixomull Stretch strips. 3 Renewal of dressings was performed as required to keep the wounds covered for the study period. 3 This procedure resulted in a high proportion of wounds in diabetic mice being splinted (79% to Day 10, 73% to Day 14), and a lower proportion in non-diabetic mice (50% to Day 8, 40% to Day 10, 25% to Day 14). 3 It was much more difficult to keep the wounds covered in non-diabetic mice due to their smaller size, different body shape, and greater activity.
Laser irradiation of wounds
The lasers (660 nm, continuous wave) used were obtained from Lasotronic GmbH (Hengersberg, Switzerland). Average outputs were 18 mW and 80 mW, measured using a power meter PM-30 and detector 400–1100 nm (ThorLabs, Newton, New Jersey) or a second power meter (Coherent Inc., Santa Clara, California), and delivered energy doses of 0.36 and 1.6 J for 20 s irradiation, respectively.
Three different treatments were tested: no treatment (referred to as control treatment); laser irradiation at lower power (18 mW, 660 nm, referred to as laser treatment 0.36 J/day); and laser irradiation at higher power (80 mW, 660 nm. referred to as laser treatment 1.6 J/day). Wounds in diabetic mice were subjected to one of the three treatments; for wounds in non-diabetic mice, only control or lower power laser treatment was used. Laser treatment with higher power laser was only performed with diabetic mice as testing for laser-stimulated wound healing in these animals was the main focus of our study. The first laser probe (18 mW) was powered using a rechargeable battery which was fully charged before beginning to irradiate wounds on each day (maximum of six mice each day). The second laser device operated from a 240 volt supply using a transformer. For laser treatment groups, wounds were irradiated for 20 s each day for seven consecutive days commencing immediately post-wounding.
To irradiate the wound, the mouse was held gently, with the laser probe positioned over the centre of the wound. The laser probe was held static with its tip lightly touching the Tegaderm dressing. This maximized wound irradiation and the dressing prevented introducing any contaminating material. The whole wound area was irradiated together with a narrow margin of skin. The irradiated area was estimated to be between 32 and 43 mm2 for both of the lasers as a narrow margin of skin about 0.5 to 1.0 mm was also irradiated for wounds in the diabetic mice on Day 1, which had a mean wound area of 23 mm2 (corresponding to 5.41 mm diameter). All mice tolerated this procedure extremely well and did not show any physical signs of stress or discomfort.
Wound repair and analysis
Photographs of wounds were taken on Days 1, 4, 7, 10, and 14 using a Fujifilm FinePix S3 Pro digital camera (Fuji Xerox, Auckland, New Zealand) with a micro-Nikkor 60 mm f/2.8D lens (Nikon, Tokyo, Japan). Wound area (mm2) was determined by tracing the wound margin with a fine-resolution computer mouse and using Image J digital analysis software (U.S. National Institutes of Health, Bethesda, Maryland).
Mice were euthanized on Day 8 (for some non-diabetic animals), 10, or 14, and the wounds excised with sharp scissors and fixed in 10% neutral buffered formalin. Wound specimens were divided along the greatest diameter and underwent routine histologic processing: embedding in paraffin wax, cutting of sections at 4 μm, and staining with haematoxylin and eosin. Sections were examined under Olympus, AX 70 light microscope (Olympus, Auckland, New Zealand) and photographed using a mounted Spot RX color camera (Diagnostic Instruments, Sterling Heights, MI, USA). The histologic appearance of sections was reported and a semi-quantitative analysis (score 1–15) was determined using a previous method. 5 Photographic images were analyzed for dermal gap (DG) and epithelial gap (EG). DG was defined as the distance across the wound between edges of the intact dermis, and EG as the distance between the advancing edges of epithelial regrowth at the wound edges. The extent of epithelial regrowth was determined as DG–EG and percentage (%) epithelization as 100 × (DG–EG)/DG. Evaluation and analysis of wound sections was performed by two independent examiners and checked by a pathologist blinded to the coding of sections. Values for DG, EG, and histologic score were measured in consecutive sections of wound specimens for two or three mice in each treatment group to validate the procedure. In addition, sections from several splinted and unsplinted wound specimens for the different treatments of diabetic and non-diabetic mice were cut at 7 μm and stained with picrosirius red. 6 These were examined for collagen birefringence under polarized light microscopy and photographed.
Statistical analyses
An analysis of variance (ANOVA) was used to test for differences in mean values of DG, EG, DG–EG, % epithelization, and histologic score between diabetic and non-diabetic mice. A Student's t-test was also used to compare mean values where ANOVA was considered to be less appropriate. Significant findings are reported at the level of p < 0.05.
Results
Splinting of wounds
It was found that the Tegaderm dressings had covered the wounds during the whole study period for some diabetic mice, and the wounds were moist and had not been air-exposed. Measurements on histologic sections of these wounds stained with haematoxylin and eosin revealed very large dermal gaps, which showed that wound contraction had been retarded and wounds splinted by the dressing and adhesive. A very high rate of splinting was obtained in the later studies with diabetic mice (16 out of 18, 89%). Although much more difficult, it was possible to splint the wounds in some non-diabetic mice.
Based on measurements of dermal gap, wounds for both diabetic and non-diabetic mice were divided into two subgroups. 3 A DG value of 2.6 mm was chosen as a threshold for dividing into splinted and unsplinted wounds in diabetic mice and represented 63% of the measured diameter 4.12 ± 0.25 mm for the fixed skin excisional biopsies from diabetic mice (n = 6; 3 males and 3 females). For non-diabetic mice, a DG value of 2.0 mm was taken as the threshold based on a measured diameter for fixed skin excisional biopsies of 4.87 ± 0.17 mm (n = 3; 3 males) and represented 41% of this diameter. 3 A much higher rate of splinting occurred for diabetic mice compared with non-diabetic mice, and there was a significant difference in the proportion of wounds splinted up to Day 10. 3
Measurements of wound area
Mean values for wound areas of diabetic and non-diabetic mice are given in Table 1; these are presented for all wounds together (i.e. not divided into two subgroups), and are also presented separately for splinted and unsplinted wounds. Inspection of the data shows that wound closure in diabetic mice that had received control or laser treatment 0.36 J/day was delayed when compared with that of similarly treated non-diabetic mice. However, wound closure in diabetic mice was stimulated by laser treatment 1.6 J/day. Similar changes occurred for splinted wounds in diabetic mice.
n = sample size for each group or subgroup.
For diabetic mice control treatment: on days 1, 4, 7, 10, 14, n = 23, 23, 23, 23, 16 for all wounds; n = 18, 18, 18, 18, 11 for splinted wounds; n = 5, 5, 5, 5, 5 for unsplinted wounds, respectively.
For diabetic mice laser treatment 0.36 J/day: on days 1, 4, 7, 10, 14, n = 12, 12, 12, 12, 9 for all wounds; n = 9, 9, 9, 9, 6 for splinted wounds; n = 3, 3, 3, 3, 3 for unsplinted wounds, respectively.
For diabetic mice laser treatment 1.6 J/day: on each of days 1, 4, 7, 10, 14, n = 12 for all wounds.
For non-diabetic mice control treatment: on days 1, 4, 7, 10, 14, n = 13, 13, 13, 12, 2 for all wounds; and n = 6, 6, 6, 5, 0 for splinted wounds; n = 7, 7, 7, 7, 2 for unsplinted wounds, respectively.
For non-diabetic mice laser treatment 0.36 J/day: on days 1, 4, 7, 10, 14, n = 7, 7, 7, 3, 3 for all wounds; and n = 4, 4, 4, 1, 1 for splinted wounds; n = 3, 3, 3, 2, 2 for unsplinted wounds, respectively.
Using ANOVA with treatment as a factor and with wound area on Day 1 as covariate, there was a statistically significant difference in mean values for wound area in diabetic mice for the different treatments on Day 4 (p = 0.035), but not on Day 7 (p = 0.273) and Day 10 (p = 0.354). Owing to the unequal variances of mean values on Day 14, ANOVA was deemed to be less appropriate for testing of differences in mean values on that day. A Student's t-test showed a statistically significant difference (p < 0.05) between mean values for wound area in diabetic mice on Days 4 and 14 for laser treatment 1.6 J/day compared with the other two treatments. Laser treatment 1.6 J/day increased the mean value for wound area on Day 4, but decreased it on Day 14, compared with the other two treatments.
Using ANOVA with status (diabetic, non-diabetic), treatment, and splinting (Yes, No) as factors, and with wound area on Day 1 as covariate, to analyze the combined data for all wounds of diabetic and non-diabetic mice, there was no statistical significant difference in wound area for splinted wounds compared to unsplinted wounds on Days 4 (p = 0.095), 7 (p = 0.881), 10 (p = 0.925), and 14 (p = 0.483).
Measurements of wound outcomes from histologic sections
Mean values for DG, EG, DG–EG, % epithelization, and histologic score on Days 8 (non-diabetic mice), 10, and 14, first for all wounds together and then for wounds divided into splinted and unsplinted subgroups, for diabetic and non-diabetic mice, are given in Tables 2 and 3. Measurements of DG and EG from consecutive sections were consistent with one another for the chosen wound specimens in each treatment group, validating the histological procedures used.
For splinted wounds, DG ≥ 2.6 mm; for unsplinted wounds, DG < 2.6 mm.
n = sample size of each group.
n = sample size of each group. For splinted wounds, DG ≥ 2.0 mm; for unsplinted wounds, DG < 2.0 mm.
Allocation of wounds into splinted and unsplinted subgroups resulted in 1 mouse being a single member of a particular subgroup (Day 8, wound splinted) so values of wound outcomes for this subgroup were not reported.
Allocation of wounds into splinted and unsplinted subgroups resulted in 2 mice that were found to be single members of particular subgroups (Day 8, wound unsplinted; Day 14, wound splinted) so values of wound outcomes for these two subgroups were not reported.
Data for diabetic and non-diabetic mice combined
An ANOVA was used to test for differences in mean values for males and females using status, treatment, day of euthanasia, and sex as factors. There was no statistically significant difference between males and females for mean values of DG (p = 0.430), EG (p = 0.497), % epithelization (p = 0.652), and histologic score (p = 0.733). Hence, further tests using ANOVA were performed without sex of mice as a factor. Using an ANOVA with status, treatment, and day of euthanasia as factors, mean values for diabetic mice were statistically significantly different from those of non-diabetic mice for DG (p < 0.0005), EG (p = 0.005), DG–EG (p = 0.002), % epithelization (p = 0.009), and histologic score (p = 0.001). Diabetic mice had a larger dermal gap, a larger epithelial gap, a lower percentage epithelization and a lower histologic score than non-diabetic mice, thereby indicating that wound healing was impaired in these animals. There was a significant effect of treatment on mean values for DG–EG (p = 0.030) and histologic score (p = 0.031).
Furthermore, an ANOVA was used to test for differences in values for splinted and unsplinted wounds using status, treatment, day of euthanasia, and splinting as factors. Mean values for splinted wounds were statistically significantly different to those of unsplinted wounds for DG (p < 0.0005), EG (p = 0.015), and histologic score (p = 0.023) but not for % epithelization (p = 0.206), while that for DG–EG was on the borderline of significance (p = 0.059). In addition, there was a statistically significant effect of treatment on histologic score for splinted and unsplinted wounds (p = 0.021).
Effect of laser treatment on wound healing
Diabetic mice
Using Duncan's Multiple Range Test, the mean value of DG–EG for diabetic mice receiving laser treatment 1.6 J/day was statistically significantly different from the value for controls (p < 0.05) but not from those receiving laser treatment 0.36 J/day (p > 0.05), and mean values for laser treatment 0.36 J/day and control treatment were not statistically significantly different (p > 0.05). Similar findings were observed when the test was limited to diabetic mice with splinted wounds on Day 14.
In addition, Duncan's Multiple Range Test showed that the mean histologic score for diabetic mice receiving laser treatment 1.6 J/day was statistically significantly different from those values for control treatment and laser treatment 0.36 J/day (p < 0.05). Mean values for controls and laser treatment 0.36 J/day were not statistically significantly different (p > 0.05). A similar finding was observed when analysis of data was restricted to splinted wounds on Day 14. There was no evidence for a difference in treatment effect with regard to mean values of histologic scores for unsplinted wounds of diabetic mice.
Non-diabetic mice
Using a two-way ANOVA (treatment and day of euthanasia as factors), no statistically significant difference in treatment effect with regard to mean histologic scores was found in non-diabetic mice. However, this may have been due to the smaller number of non-diabetic mice in the study and the use of only two treatments (control and laser treatment 0.36 J/day).
Histology of wounds
Histologic findings for all sections stained with haematoxylin and eosin were tabulated according to day of euthanasia and whether wounds were splinted or unsplinted. The most frequently reported findings are summarized in Tables 4 and 5. The most striking differences were for splinted wounds on Day 14 in diabetic mice that had received laser treatment 1.6 J/day compared to those not irradiated (control treatment). Nearly all the non-irradiated wounds were incompletely re-epithelized; about half had an inflammatory exudate, with the inflammatory response of most ranging from moderate to intense; almost all had edema; most had granulation tissue developed mainly at the wound edges; and about half had loosely arranged connective tissue in the wound bed (Figure 1). By contrast, nearly all the wounds that had been irradiated with higher power laser were completely re-epithelized; most had no inflammatory exudate and only minimal inflammatory response; granulation tissue with collagen fibers filled or almost filled the entire wound bed; and about half had a small amount of edema (Figure 2).
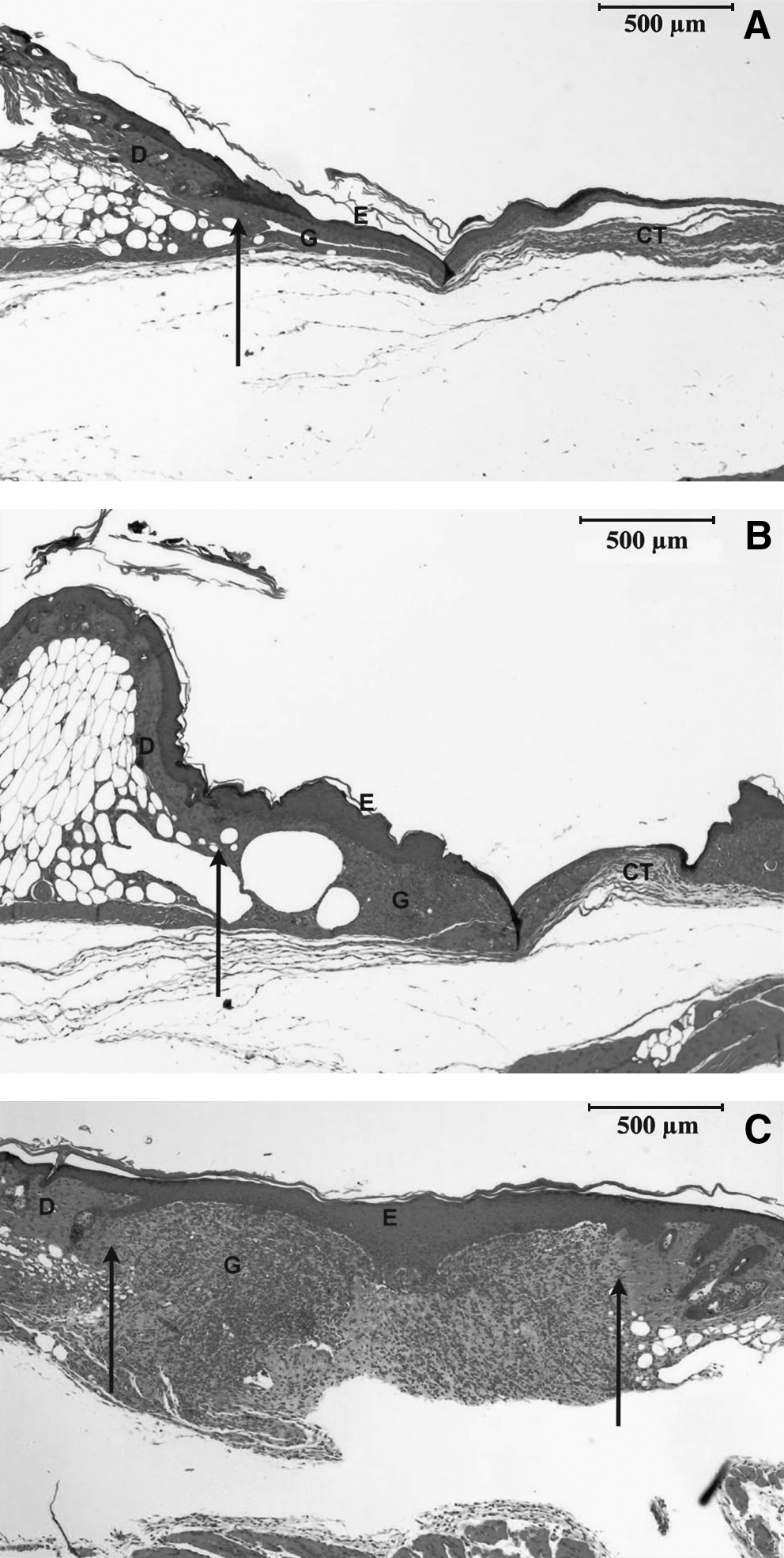
Histological sections of wounds for diabetic mice of the control treatment group (H&E).

Histological sections of wounds for diabetic mice of the 1.6 J/day laser treatment group (H&E).
As the original intention of the study was to test whether laser irradiation of wounds for seven days would stimulate wound healing in diabetic mice, a scoring system (1–5; higher scores reflecting better healing outcomes) was used to evaluate three important parameters of wound healing: inflammatory response, extent of granulation tissue formation, and collagen deposition in the wound bed. The first two parameters were scored from haematoxylin and eosin stained sections, while the third parameter was scored from orange-red birefringence under polarized light of sections stained with picrosirius red; photographs of the latter are shown in Figure 3. Mean scores are given in Table 6. The splinted wounds in diabetic mice had lower mean scores for inflammatory response and extent of granulation tissue formation compared with unsplinted wounds. This was consistent with splinting causing a delay in healing. Mean scores for inflammatory response and extent of granulation tissue formation for splinted wounds on Day 14 in diabetic mice that had received laser treatment 1.6 J/day were statistically significantly higher than controls. Also there was a much greater extent of collagen deposition for splinted wounds on Day 14 in response to laser treatment 1.6 J/day compared with control treatment.
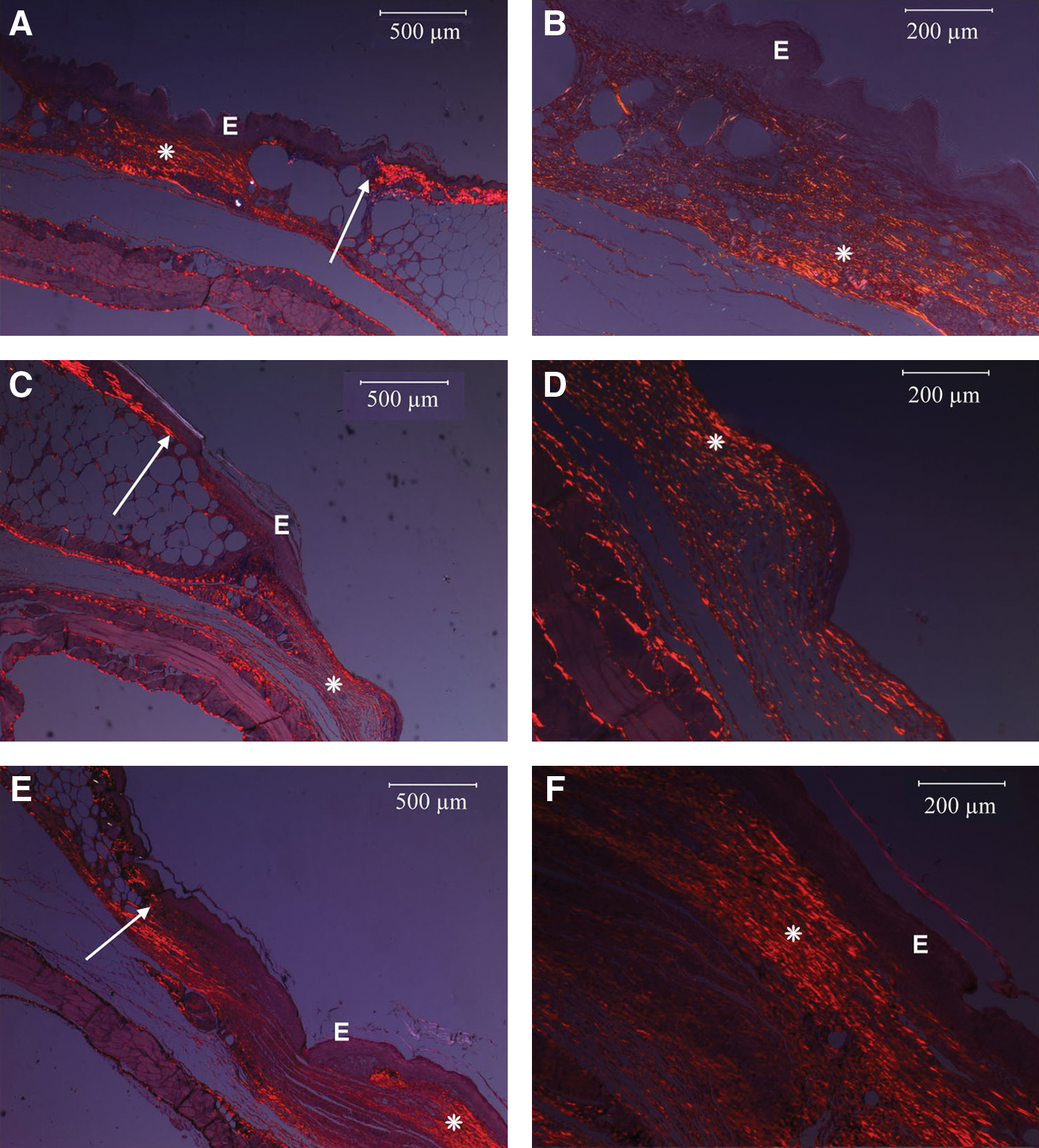
Histological sections of splinted wounds of diabetic mice on Day 14 (picrosirius red).
Unpaired t-test was not performed because the values for the control and laser treatment 0.36 J/day groups were clearly different from that for laser treatment 1.6 J/day.
p < 0.05 by Student's t-test for laser treatment 1.6 J/day compared to control.
Scoring scale for inflammatory response:
1 = intense; 2 = moderate to intense; 3 = moderate; 4 = minimal to moderate; 5 = none to minimal.
Scoring scale for granulation tissue:
1 = none to minimal at wound edge; 2 = formed at wound edge; 3 = formed at wound edge and in other parts of wound bed; 4 = fills in most of wound bed; 5 = fills in whole of wound bed.
Scoring scale for collagen:
1 = none to minimal; 2 = minimal to moderate; 3 = moderate at wound edge and minimal to moderate in wound bed; 4 = moderate to extensive at both wound edge and in wound bed; 5 = extensive at both wound edge and in wound bed.
Discussion
A recent review of research papers on laser photobiomodulation of wound healing in mouse and rat indicated that a wide variety of wound models have been used, but with considerable variation and/or inadequate reporting of research design, methodology, and laser parameters that restrict comparison of findings. 1 Rodents such as the mouse and rat are widely used in wound healing studies. However, being loose-skinned animals, their mechanism of wound closure is mainly by contraction, and differs from that of fixed-skinned animals (e.g. humans) where re-epithelization and granulation tissue formation are the major processes. 7
In a separate paper, it was shown that contraction of wounds in a genetic diabetic mouse model could be retarded (hence splinted) by use of a Tegaderm dressing with increased adhesiveness together with a superior adhesive agent to attach the dressing to the skin. 3 The dressing and adhesive agent kept the wounds open to minimize the effects of wound contraction. Splinted wounds in both diabetic and non-diabetic mice had a larger dermal gap and epithelial gap, and a lower percentage epithelization and histologic score than unsplinted wounds, thereby indicating that splinting caused a retardation of healing. 3 Splinted wounds of diabetic mice also had a greater extent of epithelial regrowth than unsplinted wounds, confirming that re-epithelization plays a major role in the healing of these wounds. 3 Other approaches to splinting wounds in mice and rats used silicone or metal rings attached to the skin using adhesives and/or sutures. 8 –12 However, the model described by Chung et al. 3 and used in this study has the advantage that wounds can be splinted without recourse to invasive treatments such as suturing the skin, which would lead to inflammation at the suture sites and could influence healing through release of inflammatory mediators such as interleukin IL-1β, and tumor necrosis factor TNF−α. 13 –16
In this study, wound closure in diabetic mice that had received control treatment (not irradiated) was delayed when compared to control wounds of non-diabetic mice. Similar changes occurred for splinted wounds of diabetic mice. The wounds of diabetic mice had a larger dermal gap, a larger epithelial gap, a lower percentage of epithelization, and a lower histologic score than those of non-diabetic mice, confirming that wound healing was impaired in these animals. The finding of a larger extent of epithelial regrowth for diabetic mice compared to non-diabetic mice indicates that re-epithelization is a major contributor to the healing of wounds in diabetic mice.
Wound closure in diabetic mice was stimulated by laser treatment 1.6 J/day. Statistical analysis showed that this laser treatment (1.6 J/day, 7 days) increased the mean value for wound area on Day 4 compared with controls and lower power laser treatment (0.36 J/day, 7 days), but decreased it on Day 14. In addition, this laser treatment increased the mean histologic score on Day 14 compared with the other two treatments, and increased the extent of epithelial regrowth compared with control treatment. A possible explanation might be that higher power laser treatment inhibited wound closure in early stages of repair by increasing the inflammatory response, but then accelerated wound closure by promoting epithelial regrowth and granulation tissue formation. Similar findings were observed for the effect of higher power laser treatment when analysis of data was restricted to splinted wounds in diabetic mice.
The stimulatory effects of laser treatment 1.6 J/day on splinted wounds of diabetic mice were observed in the histologic sections. Wound sections stained with haematoxylin and eosin showed a greater extent of re-epithelization and a greater amount of granulation tissue and collagen in the wound bed, with the collagen fibers exhibiting a higher degree of organization and maturation. The latter was also evident in wound sections stained with picrosirius red and examined for collagen birefringence using polarized light microscopy. Laser irradiation 1.6 J/day, 7 days of wounds in diabetic mice decreased the inflammatory response and stimulated wound healing by promoting formation of granulation tissue with deposition of collagen fibers in the wound bed on Day 14. This suggested that higher power laser treatment had advanced wound healing for diabetic mice throughout the repair process, from the inflammatory to the proliferative stage of repair.
There were very few previous studies in this area in which wounds were covered with a transparent adhesive film dressing; 1 this severely limited comparisons with findings in this study. Kawalec et al. 2 studied the effects of a 980 nm laser on wound healing in the same strain of genetic diabetic mice and reported enhanced healing in the 5 W (18 J/cm2) every two days subgroup. However, in addition to a different wavelength and a very high power laser being used, wounds were only covered with a Tegaderm dressing for a maximum of four days, after which closure due to contraction would have been a major factor (i.e. wounds not splinted). More closely related to the present study, Yu et al. 5 examined the effects of laser therapy (630 nm, 5 J/cm2/day for four days) on wound healing in genetic diabetic mice. In this study, wounds were covered by Tegaderm dressing until completely healed. They reported that wound closure, cellularity, granulation tissue formation, collagen deposition, vascularization, re-epithelization, and histologic scores were all improved by laser irradiation compared with the control group. However, the authors did not indicate what proportion of wounds were splinted. In both previous studies, a pair of wounds was made on the dorsum of each mouse, one of which in some or all of the mice served as a control. Such a research design had the disadvantage that treatments applied to one wound might affect the other as laser-mediated effects are not limited to the site of application. 17,18 The previous studies on splinting wounds in mice and rats using different methods 8 –12 have not investigated the effects of laser irradiation on wound healing.
The diabetic mouse model (BKS.Cg-m+/+Leprdb ) has the most impaired wound healing among a number of different diabetic mouse models. 12 This is the first reported study of the effects of laser irradiation on splinted wounds using this model, and the pronounced stimulation of wound healing by laser treatment 1.6 J/day is an important experimental finding. Laser treatment 1.6 J/day for an irradiated area of between 32 and 43 mm2 (see Materials and Methods) represented an energy density of between 3.7 and 5.0 J/cm2/day, while that for laser treatment 0.36 J/day represented an energy density of about 1 J/cm2/day. Because of the drop-off in power with the battery-operated lower power laser, the energy delivered to most of the wounds was likely to have been less than 0.36 J/day and consequently the energy density lower than 1 J/cm2/day. The marked stimulation of wound repair brought about by higher power laser treatment, but not lower power treatment, is consistent with previous studies. 18,19
In conclusion, splinted wounds of diabetic mice were shown to heal mainly by re-epithelization and granulation tissue formation, which mimics closely wound healing in human patients with type-2 diabetes. Thus, the presence of the Tegaderm dressing serves to more accurately represent fixed-skin attributes (as in humans) in these loose-skinned murine subjects. The finding that laser treatment at 1.6 J/day (3.7–5.0 J/cm2/day) promoted wound healing in splinted wounds in diabetic mice strongly supports further testing of other sets of laser parameters using this model of impaired healing. It would be important to develop an optimized set of laser parameters so that this might be used as a basis for laser therapies treating diabetes-related cutaneous pathologies in diabetic human subjects.
Footnotes
Acknowledgments
The technical assistance of Ms. M. Fisher and Ms. D. Potter, Histology Unit, University of Otago, is gratefully acknowledged, and we wish to thank Dr. N. Hung, Department of Pathology, University of Otago, for assistance with the histologic analysis of the wound sections.
We are grateful to Professor A. Wilson, Department of Physics, University of Otago, for measuring the power outputs of the two lasers.
Also, we thank Associate Professor P. Herbison, Department of Preventive and Social Medicine, University of Otago, for statistical advice.
Author Disclosure Statement
No competing financial interests exist.