
Abstract
Introduction
It has been shown that low-power lasers induce morphological alterations in different structures by promoting changes in RNA synthesis, increase in vascularization, 7 positive effects on cell proliferation, 8 and differentiation and calcification of osteoblastic clone cells. 9 These alterations occur in response to photobiomodulation, which may stimulate or inhibit a target tissue treated with laser irradiation. 10
Tissue responses triggered by laser irradiation are related to parameters such as wavelength, amount of energy delivered to the tissue, number of sessions, and exposure time, among others. 11,12 The type of laser used in physical therapy is not harmful since the power output is below 1 W. 9
Many authors have suggested the use of laser irradiation in children 13 –15 based on the study by Cheetham and colleagues, 6 who irradiated the knee joint of rats three times per week at an energy density of 5 J/cm2, evaluated the epiphyseal cartilage on days 6 and 12 of treatment, and demonstrated that this energy was not sufficient to change the structure of the epiphyseal cartilage.
Different dosimetric parameters may produce different photobiomodulatory effects, so it is necessary to vary these parameters to demonstrate that laser irradiation can be safely applied to epiphyseal growth plates. 10
The aim of this study was to verify the effect of an 830-nm GaAlAs diode laser at two different energy densities (5 and 15 J/cm2) on the epiphyseal cartilage of rats by evaluating the bone length and the number of chondrocytes and thickness of each zone of the epiphyseal cartilage.
Materials and Methods
This research was approved by the Research Ethics Committee (CAPPesp) at the University of São Paulo Medical School General Hospital, São Paulo, Brazil, under the process number 0942/07. All animals received humane care in strict compliance with the Guide for the Care and Use of Laboratory Animals (National Research Council, 1996).
Animals
A total of 30 male Wistar rats at 23 days of age and weighing 90 g on average was used in this study. The animals were obtained from the Central Laboratory Animal Facility at the São Paulo State University, College of Medical and Biological Sciences, Botucatu, São, Brazil, and maintained in the Laboratory Animal Facility at the Department of Physical Education, UNESP Institute of Biological Sciences, Rio Claro, São Paulo, Brazil. The rats were housed in groups, with a maximum of five animals per cage, at a mean temperature of 25°C and with controlled air flow, on a 12-h by 12-h light–dark cycle, and were fed a nutritionally balanced rat chow and water ad libitum.
Experimental groups
The 30 rats were randomly divided into 3 groups of 10 animals each, as follows: The control group (CG) consisted of animals that did not undergo laser treatment. The G5 group consisted of animals that underwent laser treatment at an energy density of 5 J/cm2. The G15 group consisted of animals that underwent laser treatment at an energy density of 15 J/cm2.
Treatment site
According to the planned protocol, the animals were weighed at the beginning and end of the experiment. The knees of the animals were shaved prior to treatment. Laser irradiation was then applied to the anterior, medial, and lateral faces of the proximal tibial epiphysis of each rat.
Laser equipment
The 830-nm GaAlAs diode laser power meter (Bioset, Rio Claro, São Paulo, Brazil) used in this study was previously calibrated (Ophir 30A-P-Dif ).
Treatment protocol
The rats were treated with an 830-nm GaAlAs diode laser operating in a continuous pulse mode, with a peak output power of 0.04 W, power density of 5.128 mW/cm2, beam diameter of 3 mm, and beam area of 0.078 cm2. Laser therapy was applied to 3 treatment points on each knee by placing the probe in direct contact with the skin of the animal. In the G5 group, laser irradiation was applied at an energy density of 5 J/cm2, 10 sec/point, to deliver 0.4 J/point, corresponding to a total dose of 1.2 J per treatment session. In the G15 group, laser irradiation was applied at an energy density of 15 J/cm2, 30 sec/point, to deliver 1.2 J/point, corresponding to a total dose of 3.6 J treatment session. After the first application, treatment sessions were conducted at regular intervals of 48 h. 16 The laser probe was positioned perpendicularly to the surface to be irradiated to minimize reflections. 17 The probe tip was cleaned with sterile cotton and 70% alcohol before every application.
Collection of the tibia
The animals were killed 24 h after the last treatment session (21 days after the first application) with a lethal dose of sodium pentobarbitone (200 mg/kg).
The tibiae were disarticulated at the knee and ankle, cleaned of soft tissue, and fixed by immersion in 10% formaldehyde solution for 72 h. Then they were transferred to a solution of 5% nitric acid for decalcification. After the decalcification period, the tibiae were dehydrated in an ascending series of alcohol concentrations, cleared in xylol, and embedded in paraffin blocks in an orientation that allowed coronal sectioning.
Histological sections and techniques
A rotary microtome was used to cut 6-μm longitudinal sections of the tibiae. These sections, containing a sample of the epiphyseal cartilage, were stained with hematoxylin–eosin (HE) so that the cartilage elements could be identified and measured. The sections were mounted onto slides, which were photographed with a Zeiss photomicroscope.
Histomorphometric analysis
Histomorphometric analysis was performed with the aid of a camera coupled to the microscope. Images were sent to a monitor, through which the total thickness of the epiphyseal cartilage, the number of chondrocytes, and the thickness of the resting, proliferative, hypertrophic, and degenerative zones were measured using a 0.01-mm slide micrometer (Olympus).
X-ray image analysis
Prior to the first laser application and after the last application, x-ray radiographs of the tibia of the animals were taken with a dental x-ray unit in latero-lateral projection. By analyzing the radiographs, the presence and integrity of the epiphyseal cartilage was verified and measured using AutoCAD® software. To obtain the mean thickness of the epiphyseal cartilage, five measurements were taken from each radiograph. These images were also used to measure the initial and final length of the tibia, that is, its length before and after laser treatment (Fig. 1).

X-ray measurements of the epiphyseal cartilage and length of the tibia.
Statistical analysis
Statistical analysis was performed using one-way analysis of variance (ANOVA), followed by Tukey's post hoc test. All statistical tests were performed at a significance level of 0.05.
Results
Qualitative and histomorphometric analyses
No important differences were found in the results of qualitative macroscopic analysis of the morphological and radiographic appearance of the epiphyseal cartilage after laser treatment in all experimental groups. However, a more detailed analysis based on linear measurements of the chondrocyte layers that form the epiphyseal cartilage revealed that the resting cells, which are located on the boundary between the epiphyseal growth plate and osseous epiphysis, had a small number of chondrocytes (Table 1) distributed in the extracellular matrix. The general aspect of the cells suggested a small mitotic activity; also, cells were surrounded by reduced lacunar spaces, which is indicative of reduced cell activity.
Same letters in the same column indicate no statistical difference (p > 0.05); different letters in the same column indicate statistical difference (p < 0.05).
In the proliferative zone, isogenous groups form aggregates or “piles” of chondrocytes with evident mitotic activity and uniform morphology (Figs. 2, 3, and 4). No morphological differences between groups were found either in the size of the piles of chondrocytes or in the direction of their distribution, which was longitudinal to the bone.
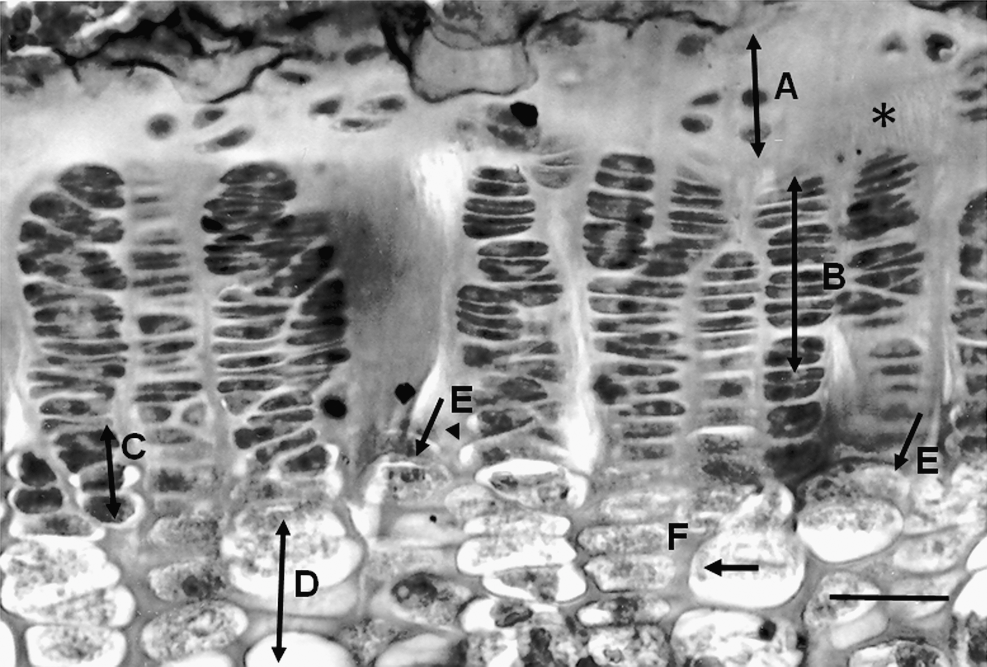
Epiphyseal cartilage from a rat in the control group (CG) showing the different chondrocyte layers (cartilage zones): resting zone (
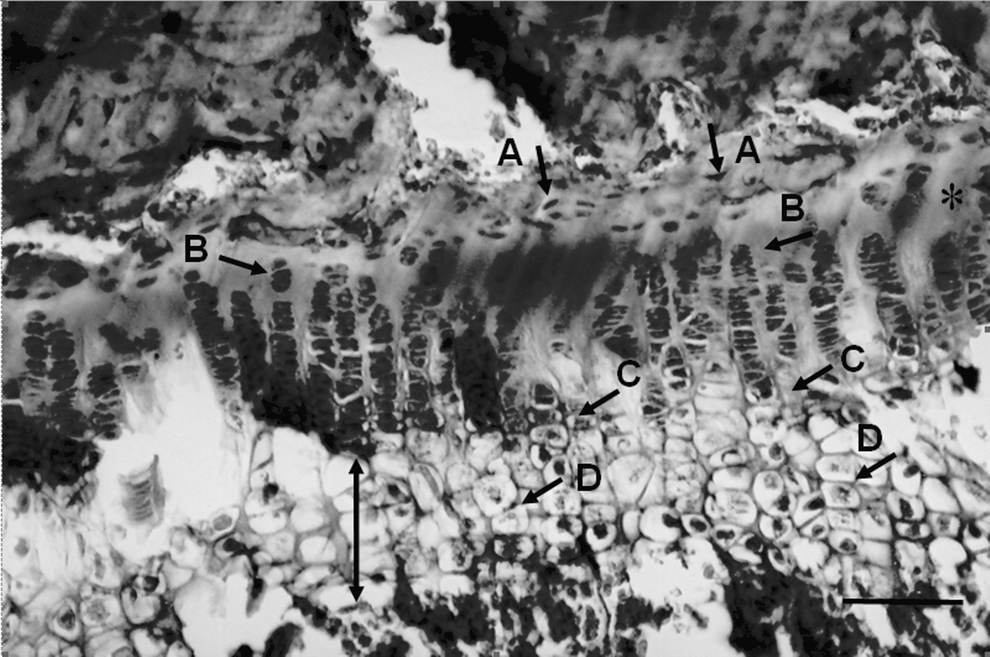
Epiphyseal cartilage from a rat in the G5 group showing, in the resting zone, a group of cells with low mitotic activity (
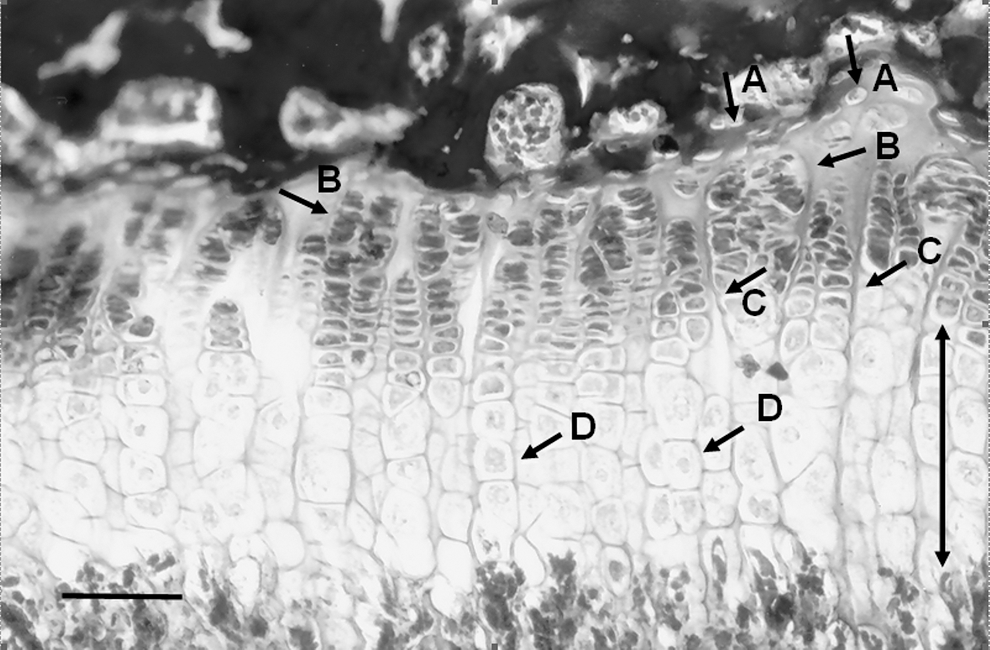
Epiphyseal cartilage from a rat in the G15 group showing, in the resting zone, a group of cells with low mitotic activity (
In group G15, the hypertrophic zone was slightly thinner than those in the other groups (Table 2; Figs. 3 and 4), and chondrocyte layers that form the epiphyseal cartilage had uniform thickness and morphology compared with those in the CG (Table 2).
,†,‡Same letters in the same column indicate no statistical difference (p > 0.05); different letters in the same column indicate statistical difference (p < 0.05).
The degenerative zone showed the presence of large vacuoles and retracted cytoplasm in all groups. However, in groups G5 and G15, the degenerative zone was slightly more disorganized compared with the CG, showing an increase in the number of degenerated chondrocytes (Table 1) with a consequent increase in the thickness of this zone, which was also verified by the x-ray images (Table 3).
,†,‡Same letters in the same column indicate no statistical difference (p > 0.05); different letters in the same column indicate statistical difference (p < 0.05).
Quantitative analysis
Statistical analysis was performed using one-way analysis of variance (ANOVA) followed by Tukey's post hoc test. All statistical tests were performed at a significance level of 0.05.
Discussion
Histological analysis and x-ray images revealed that irradiation with a GaAlAs diode laser, operating at a wavelength of 830 nm, induced an increase in the thickness of the epiphyseal cartilage in the G5 and G15 groups and increased the number of chondrocytes in the G15 group.
The different cartilage zones responded differently to laser therapy. There was a significant decrease in the thickness of the resting zone in both treatment groups compared with that in the CG. The thickness of the hypertrophic zone was reduced in the G15 group compared with that in the control group. Also, there was an increase in the thickness of the degenerative zone in the treatment groups compared with that in the control group, as well as in the G15 group compared with the G5 group. However, this increase in the thickness of the epiphyseal cartilage was not associated with changes in tibia length, according to analysis of x-ray images.
According to Iannotti, 1 the resting zone consists of a chondrocyte layer whose function is associated with storage of nutrients and substrate, such as lipids and glycogen, and since these cells are rich in endoplasmic reticulum, they produce proteins. The reduction in the thickness of the resting zone in both treatment groups may be caused by an increase in the metabolism of these cells, which, when stimulated by laser irradiation, began to consume more nutrients from the extracellular matrix for cellular activities. This should be examined in further studies.
Studies have demonstrated that laser treatment induces changes in the number of components of the respiratory chain (cytochrome, cytochrome oxidase, and flavin dehydrogenase) by excitation of photoreceptors or chromophors. 18 It is also known that it may induce important metabolic changes that may affect cyclic nucleotide levels, which is a component involved in mRNA synthesis, which in turn is a marker of protein synthesis. 19
In our study, no changes were found in the proliferative zone in both G5 and G15 groups, because the function of the chondrocytes in this zone is related to the production of extracellular matrix, which contains collagen fibers and other substances, and to the production of new chondrocytes. 1 Chondrocyte proliferation is the only factor responsible for the linear growth of long bones. 20 No significant differences were found in the length of tibiae among the three groups; we believe that this is because the proliferative zone was not affected by laser treatment.
Lyon and colleagues 21 observed that the proliferative zone became disorganized after applying ultrasound to the epiphyseal growth plate, with high intensities (2.2 W/cm2) resulting in pathological changes in the epiphysis and metaphysis and low intensities (0.5 W/cm2) causing no changes in the epiphysis. Ogurtan and colleagues 22 used intensities of 0.2 and 0.5 W/cm2 and concluded that there was no partial or total closure of the growth plate in the carpal region, and no deformities were found.
Morein and colleagues 23 conducted a study on the epiphyseal cartilage of rabbits using a high-energy carbon dioxide (CO2) laser and demonstrated that a laser beam applied directly to the epiphyseal cartilage may damage the cartilage selectively without affecting the adjacent bone.
Clinical data show the deleterious effect of high-energy lasers on children. Peterson and Wood 24 reported a case of a child with tissue damage in two distal phalangeal epiphyseal plates associated with the use of a CO2 laser for wart removal that resulted in deformity and shortening of the digits, requiring corrective osteotomy.
In the present study, there was a reduction in the thickness of the hypertrophic zone in the G15 group. This may be related to a probable acceleration of the ossification phase in the septa, from when hypertrophic chondrocytes start to degenerate until their total disintegration. Empty lacunae formed by chondrocyte degeneration were later occupied by bone marrow.
Osteoclasts and osteoblasts, which are present in the bone marrow, work synchronously in bone resorption and bone formation as part of a process called remodeling. It seems that, in the treatment groups, the invasion of osteoclasts and osteoblasts may have occurred more slowly, since the lacunar spaces of chondrocytes remained empty and intact, showing an increase in the thickness of the degenerative zone proportional to the number of degenerated chondrocytes in the layer. The explanation for the fact that the degenerative zone remained for a longer time without being invaded by bone marrow should be addressed in a further study on the formation of septa and their remodeling by osteoclasts and osteoblasts under the influence of laser irradiation.
According to the collected data, the total thickness of the epiphyseal cartilage in the treatment groups increased, probably due to the increase in the number of chondrocytes in the degenerative zone.
Torricelli and colleagues 25 used a GaAlAs laser to evaluate in vitro the effect of biostimulation on the epiphyseal cartilage and observed that laser irradiation had a positive biostimulatory effect on chondrocytes and caused no damages.
In the present study, we believe that there was an increase in the thickness or density of the extracellular matrix that hindered and delayed the action of osteoclasts and lysosomal enzymes responsible for the resorption of the transverse septa of each chondrocyte column, allowing their further invasion by endothelial cells, osteoblasts, osteoclasts, and capillaries, as well as bone marrow cells (hematopoietic cells). This should be examined in further studies.
An increase in the thickness of the degenerative zone may be a risk factor for fractures in this region of the bone, because an increase in the size of a bone region that is not completely formed and calcified may render the bone more susceptible to injuries.
Further studies are needed in which dosimetric parameters (amount of energy delivered, laser wavelength, length of treatment and number of sessions, among others) are varied to verify possible changes in the epiphyseal cartilage.
Conclusion
We concluded that treatment with an 830-nm GaAlAs diode laser, within the parameters used in this study, induced changes in the thickness of the epiphyseal cartilage and increased the number of chondrocytes in the degenerative zone. However, these alterations were not sufficient to induce changes in total bone length.
Footnotes
Author Disclosure Statement
No competing financial interests exist.