
Abstract
Introduction
To prevent the ingress of new pathogens from the oral cavity and to maintain the success of the endodontic procedure, an adequate three-dimensional obturation and coronal seal, after meticulous cleaning and shaping of the root-canal space, are required. 17,18 The removal of the smear layer plays an important role in this success, with the use of EDTA as a determining parameter. EDTA rinsing solution used as a final rinse provides effective smear-layer removal. 19,20 Irrigants that can remove the smear layer allow penetration of sealers into dentinal tubules. 21,22 Sealer penetration may serve an important role by preventing reinfection and by incarcerating and depriving residual microorganisms of a nutrient source. 23,24 It will increase the interface between materials and dentin, thus improving the sealing ability and retention of the material by mechanical interlocking. 25 The obturation technique apparently plays a minor role in the degree of interlocking and penetration of the sealer into the dentinal tubules. 25 A first aim of this study was hence to investigate whether smear-layer removal by the use of EDTA in association with the Nd:YAG laser would affect microleakage differently. With limited information available regarding the morphologic changes after Nd:YAG laser irradiation in root canals after irrigation with both NaOCl and EDTA, SEM analysis was performed in addition on all experimental groups to visualize the effect of the cleaning protocol on the root-canal walls.
Evidence suggests that laser-activated irrigation with an erbium laser may induce cavitation when the laser is activated in the irrigant itself. 26,27 The result is an enhanced removal of the smear layer as compared with passive irrigation with the endodontic needle. 28 Laser interaction with matter generating cavitation and subsequent pressure waves has also been described for the Nd:YAG. 29 A second aim of this study was then to investigate the effect of laser activation into the root-canal irrigant on root-canal wall cleanliness and the final seal obtained with the root filling.
To eliminate the effect of morphologic changes at the most apical preparation point just above the apical constriction on the seal of the root filling, 16 all roots were also tested on through-and-through leakage after resection of the root tip, thus exposing the gutta-percha root filling.
Materials and Methods
Tooth selection
This study used 75 extracted human straight single-rooted teeth with mature apices for the leakage experiments (five groups of 15 teeth) and 15 teeth (five groups of three teeth) for scanning electron microscopic evaluation. The experimental protocol was approved by the ethical committee of the Ghent University Hospital (Belgium) (2008/186). All teeth were stored in 10% formalin until each experimental subgroup was complete. The preservation time before root-canal treatment did not exceed 6 weeks. To exclude teeth with multiple root canals, all teeth were radiographed from two angles before root-canal treatment. Organic debris was removed by submerging the teeth in 2.5% sodium hypochlorite for 8 h. Subsequently, they were washed with tap water for 1 h and stored in saline solution until used.
Root-canal treatment
Crowns were removed 2 mm above the cementoenamel junction by using a high-speed fissure burr and water spray. After gross removal of pulp tissues, a size 10 Flexofile (Dentsply Maillefer, Baillaigues, Switzerland) was introduced into the canal until it could be seen in the major apical foramen. The working length was determined by subtracting 1 mm from this length. The root canals were prepared by means of a crowndown/stepback technique, by one operator. The coronal half of the root canals was preflared with Gates Glidden drills (Dentsply Maillefer) in a larger-to-smaller sequence (numbers 4-3-2), and the canals were copiously irrigated with 2.5% sodium hypochlorite solution by using a 27-gauge endodontic needle (Monoject; Sherwood Medical, St. Louis, MO). The apical half of the canal was then prepared with the stepback technique up to a master file size 40. The canals were dried with paper points, and the patency of the apical foramen was confirmed with a size 10 Flexofile. The assignment of the teeth to the specific experimental groups was determined by the final cleaning of the root canal: a final rinse with 3 ml 17% EDTA solution (Pulpdent EDTA Solution 17%; Pulpdent Corporation, Watertown, MA) for 3 min, or lasing with the Nd:YAG laser (FidelisPlus II; Fotona, Ljubljana, Slovenia), or the combination of a 17% EDTA rinse followed by Nd:YAG lasing. When the EDTA solution was used as final rinse, an additional rinse with 2.5% NaOCl was performed.
This protocol resulted in five groups of 15 teeth (Groups 1 to 5): (1) 2.5% NaOCl rinses during root-canal preparation and a final rinse with 17% EDTA (standard protocol), followed by the rinsing out of the 17% EDTA with 2.5% NaOCl; (2) standard protocol + Nd:YAG lasing in a dried root canal; (3) 2.5% NaOCl rinses during root-canal preparation followed by Nd:YAG lasing in a dried root canal; (4) standard protocol + Nd:YAG lasing in a wet root canal; and (5) 2.5% NaOCl rinses during root-canal preparation followed by Nd:YAG lasing in a wet root canal. These five groups consisted of the nonresected teeth. The same teeth were then horizontally resected up to the most apical point of the canal preparation after leakage measurement, so that the root-canal filling was exposed, and leakage could be performed in the resected roots. This resulted in an additional five experimental groups: Groups 1r to 5r.
Laser treatment
Root canals in the lased groups were irradiated with an Nd:YAG laser (1.064 μm) (FidelisPlus II; Fotona) with a flexible fiber (diameter, 300 μm) at 1.5 W, 15 Hz, 100 mJ. The flexible fiber was inserted into the root canal 1 mm short of the working length. During irradiation, the fiber tip was moved in a spiral motion along the root-canal walls. The procedure was repeated 4 times for 5 s, with a time interval of 20 s. All apical foramina remained patent (control with a file ISO 15).
Root-canal filling
All root canals were dried with paper points before filling. A standard size gutta-percha cone (Dentsply Maillefer) that matched the master apical file was fitted to the working length with tug back. Root canal sealer AH 26 (Dentsply Detrey, Konstanz, Germany) was mixed according to the manufacturer's instructions and placed in the canal with the gutta-percha to working length. The master cone was then coated again with root-canal sealer and gently seated at the working length.
Lateral condensation was carried out by using size 20 and 25 accessory gutta-percha cones with endodontic finger spreaders (Dentsply Maillefer) placed, in the first instance, to within 1 mm of the working length. The gutta-percha cones coated with sealer were laterally condensed until they could not be introduced > 3 mm into the root canal. After obturation, the gutta-percha was removed from the coronal cavity up to the level of the cementoenamel junction with a warm instrument (PK Thomas Waxing Instrument, PKT-2; Hu Friedy, Leimen, Germany) and vertically condensed with Machtou pluggers (Dentsply Maillefer).
After the root-filling procedure, a small cotton pellet was sealed in the access cavity of all root-filled teeth by using Ketac-Fil (3MEspe, Seefeld, Germany). The samples were then stored in Vacutainers at 80% relative humidity for 48 h at 37°C (start of the first capillary-flow porometry measurements). Before storing the teeth, radiographs were taken from the buccal and mesial sides of every tooth.
Measurement of capillary flow
Capillary-flow porometry (CFP, 1200 A; PMI, New York, NY) provides fully automated through-pores analysis including bubble-point pressure, pore-size distribution, and mean pore size. A wetting liquid (Galwick: 15.9 dynes/cm, PMI) was used to fill the pores of the sample. The fully wetted teeth were attached in the sample chamber (Tubepack; Legris Connectic, France), with adhesive epoxy (Loctite 3430; Loctite, Kontich, Belgium), after which the sample chamber was sealed. Gas was then allowed to flow into the chamber behind the sample. When the pressure reaches a point that can overcome the capillary action of the fluid within a pore (maximum pore), the equivalent bubble-point pressure has been found. After determination of the bubble-point pressure, the pressure is increased, and the flow is measured until all pores are empty, and the sample is considered dry. Pressure ranges from 0 to 200 PSI, and the pore size range that can be measured lies between 0.035 and 500 μm. Measurements for this study were performed at VITO (Vlaamse Instelling voor Technologisch Onderzoek, Mol, Belgium).
After 48 h, all nonresected teeth were measured after removal of the Ketac-Fil filling and cotton pellet, to assess the minimal, mean, and maximal through-pore diameters of each experimental tooth. Voids responsible for leakage were supposed to be present between the root-canal filling and the root itself.
A second series of measurements was performed after resection of the root end up to the most apical point of the preparation length, so that the gutta-percha was exposed. In most cases, this resulted in the resection of at least 1 mm from the physiological apex and almost 2 mm from the root tip seen as the radiologic apex on a radiograph. The resection was performed with a diamond-wheel saw. After this procedure, all teeth (now Groups 1r to 5r) were subjected again to CFP, so a comparison could be made from teeth with an apical constriction and those in which the apical gutta-percha is exposed, as is the case with resected teeth.
Statistical analysis
Results from both methods were analyzed statistically by using nonparametric tests: comparison between the leakage results according to the different additional cleaning protocols were made with Kruskal-Wallis and Mann-Whitney U tests. The level of significance was set at 0.05.
Scanning electron microscopic evaluation
Three additional teeth from each experimental group were analyzed with SEM. 30 These teeth were split longitudinally in the buccolingual plane. The samples were then dehydrated in ascending series of aqueous ethanol, critically point dried with liquid CO2, sputter coated with gold (JEOL JFC1200; JEOL, Japan), and examined under the scanning electron microscope (JEOL JSM-5600-LV; JEOL, Japan).
Representative microphotographs were taken at various magnifications of the apical, middle, and coronal third of the roots. SEM pictures at × 2,000 magnification were evaluated by an independent blinded investigator.
Results
Leakage assessment by means of capillary-flow porometry
Measurements were obtained for each sample at each point in time, confirming the presence of through pores regardless of which root-canal wall cleaning protocol was being tested. Exact values for minimum, mean flow, and maximum pore diameters (range and median) of each sample were obtained. The results of the study are summarized in Table 1.
Groups 1 to 5 consist of nonresected roots. Control group: 1. irrigation with NaOCl 2.5% and EDTA 17% or standard protocol (SP); Dry lasing protocol: 2. SP + Nd:YAG lasing (dried root canal, RC), 3. NaOCl 2.5% + Nd:YAG lasing (dried RC); wet lasing protocol: 4. SP + Nd:YAG lasing in EDTA (wet RC), 5. NaOCl 2.5% + Nd:YAG lasing in NaOCl (wet RC).
Leakage assessment: no laser treatment versus laser treatment
No statistically significant differences were found between Groups 1 through 5 of the nonresected teeth. In the group of the resected roots, statistically significant differences in mean flow pore diameter were observed between Groups 1r and 2r (p = 0.026), with Group 1r having the largest mean flow pore diameter. Statistically significant differences in maximum pore diameter were observed between Groups 1r and 3r (p = 0.016), and 1r and 5r (p = 0.023), with Group 1r having the largest maximum pore diameter in both comparisons. No significant differences were seen between Groups 1r and 4r.
Groups 1r to 5r consist of the filled teeth of Groups 1 to 5 with resected apices up to the most apical point of the preparation length and exposing the root-canal filling.
Leakage assessment: dry protocol versus wet lasing protocol
No statistically significant differences were found between any groups of the nonresected teeth. Statistically significant differences in mean flow pore diameter were observed between Groups 2r and 4r (p < 0.003), with Group 4r having the largest mean flow pore diameter. No significant differences were seen between Groups 3r and 5r.
Leakage assessment: nonresected roots and resected roots
No statistically significant differences were found between the groups with and without root tip and with identical cleaning protocols.
Scanning electron microscopic evaluation
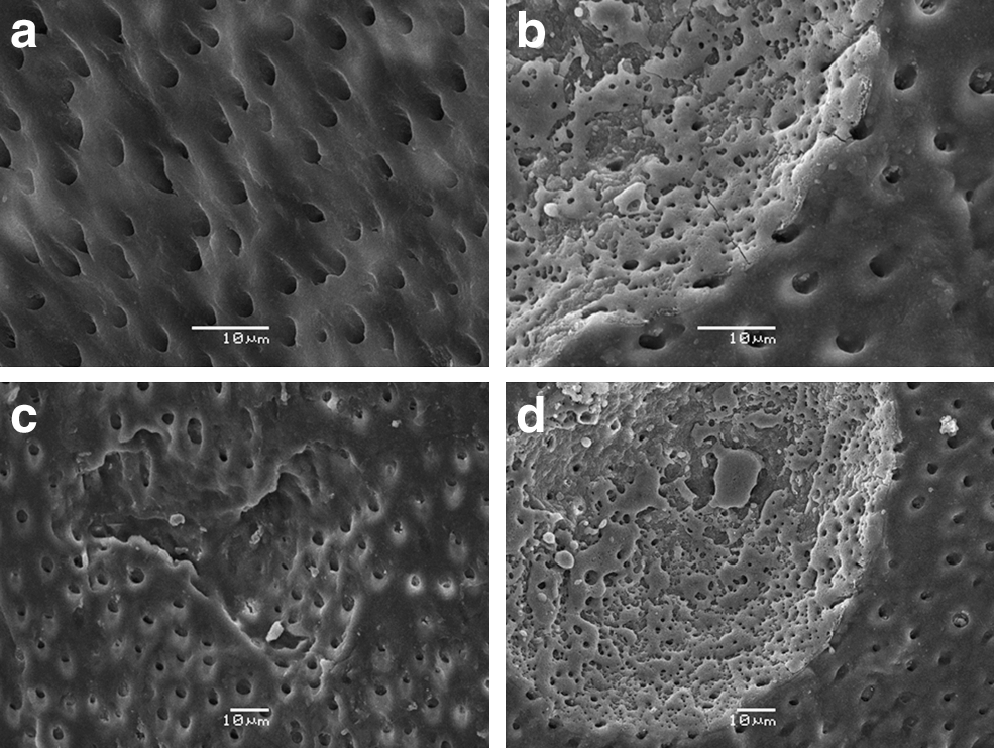
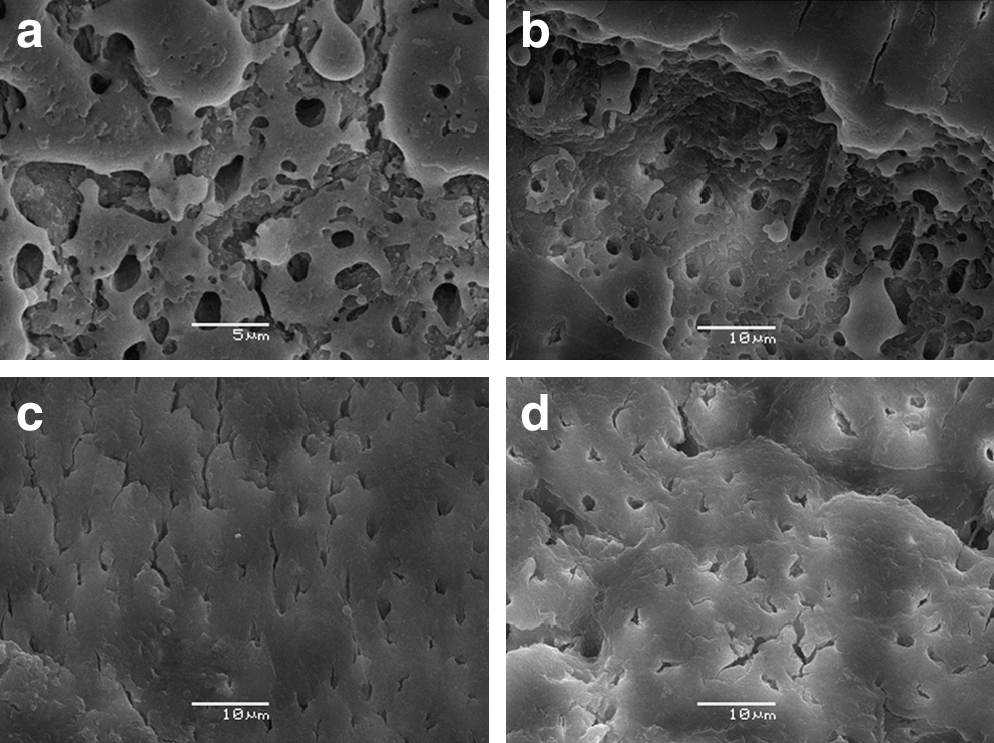
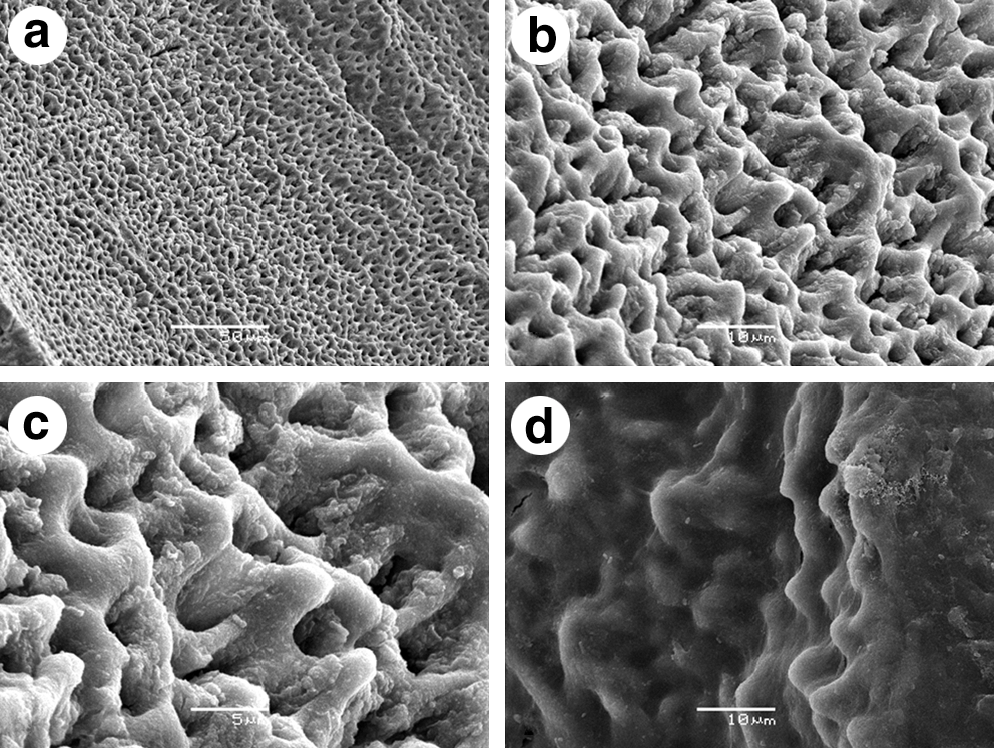
Representative images of the smear layer after conventional preparation supported with NaOCl irrigation and followed by a final rinse of EDTA are shown in Fig. 1 (Groups 1 and 1r). Abundant smear-layer removal is seen in the coronal (Fig 1a) and middle third (Fig. 1b). In the apical part, only a limited part of the dentinal tubules is opened (Fig. 1c and d), and an abundant smear layer is still present. Figure 2 shows the effect of exposure of the root-canal wall after final rinsing with EDTA to the Nd:YAG laser (Groups 2 and 2r). Areas with open tubules could be detected, especially in the coronal and middle third (Fig. 2a) and less in the apical third. Local areas of melted and evaporated dentin were found in areas where the fiber had touched the root canal walls (Fig. 2b and d). Localized areas with removal of root-canal wall dentin without glazing or melting effect were observed in the middle third (Fig. 2c). Figure 3a shows the classic image of the morphologic effect of a smear layer exposed to the Nd:YAG laser (image taken in the apical third); areas of melting, glazing, and recrystallization were seen in all thirds (Groups 3 and 3r). When the Nd:YAG laser was activated in the EDTA solution, clean root-canal walls to the same extent as when the canal was rinsed with EDTA solution were found, although the root-canal walls showed irregular dentin surfaces with round cuffs around the orifices of the dentinal tubules (Fig. 4a–c) (Groups 4 and 4r). These rounded areas, still covered with a smear layer, were also observed (Fig. 4d). In the group in which the Nd:YAG laser was used in NaOCl (Groups 5 and 5r), a smear layer was present at all sites, except for some areas where the fiber touched the root-canal wall, and a direct interaction with the root-canal wall led to localized removal of dentin and signs of carbonization and melting (Fig. 3b–d).

SEM photos of root-canal walls cleaned with 2.5% NaOCl during root canal preparation and a final rinse of 17% EDTA. Smear layer is removed in the coronal
SEM photos of root-canal walls cleaned with Nd:YAG after the sole use of NaOCl as irrigant. When Nd:YAG is used in dried canals, typical morphologic changes such as glazing, melting, and recrystallization are observed
SEM photos of root-canal walls cleaned with 2.5% NaOCl during root-canal preparation and a final rinse of 17% EDTA, followed by Nd:YAG lasing. Because of the absence of smear layer, the typical morphologic changes associated with Nd:YAG lasing are not seen [
SEM photos of root-canal walls where the Nd:YAG laser is activated in 17% EDTA solution. Areas with removal of smear layer
Discussion
In the present study, microleakage was investigated in association with different lasing and cleaning protocols. A comparison was also made for identical cleaning protocols between nonresected roots and resected roots to avoid the impact of root-canal wall modification with the Nd:YAG laser at the level of the apical stop and the apical constriction. In previous studies, it was demonstrated that morphologic changes at this point influenced the apical seal in a positive way. 13,16 So the impact of morphologic changes of the root-canal wall due to the Nd:YAG on the lateral seal of a root filling could be investigated.
Capillary-flow porometry (CFP) was used to assess leakage. The technique has been used extensively in industries worldwide, ranging from membrane filtration to nonwovens to battery industries for R & D and quality control. The method has been approved by the American Society of Testing and Materials (ASTM Designation 1999). The validity of this technique in dentistry has been verified by De Bruyne et al., 31,32 who consequently introduced this method into endodontics. CFP was chosen as the evaluation method because of its nondestructive nature and the highly reproducible and accurate data it generates. 33 –35 As such, the method can overcome the problem of limited reproducibility and comparability of conventional methods for evaluating leakage. 36,37
The removal of the smear layer is considered important: its removal results in a proper action of irrigants and intracanal medication, a deeper penetration of root-canal sealer, and more obturated lateral canals. 38 –41 It has been demonstrated that the alternate use of NaOCl and EDTA irrigants results in smear-layer removal and a dentin surface with open tubules. 42 This information has to be interpreted with care, as the removal of smear layer in the apical region remains unpredictable. 20,43 The latter was also the case in the present study (Fig. 1c and d).
Morphologic changes due to Nd:YAG laser irradiation, such as fusion and recrystallization of the dentin, were already demonstrated. 1 –7,13 These changes are confirmed on the SEM images in this study in Group 3 with Nd:YAG lasing, after the NaOCl supported root-canal preparation (Fig. 3a). For all other groups in which the Nd:YAG was used, the typical signs of glazing, melting, and recrystallization were not observed in the same manner. The effect of the Nd:YAG was seen only in the group with a final EDTA rinse, when a direct contact occurred with the root-canal wall (Fig. 2). Apparently the absence of the smear layer results only in a laser–root-canal wall interaction when the root-canal wall is touched. This means that widespread crystallization, glazing, or melting effects are seen only in situations with abundant smear layer before lasing. Hence, when the smear layer is absent, no evaporation or contraction of the smear layer occurs because of Nd:YAG lasing. It is only when direct contact with the root canal wall with the fiber occurs that the typical morphologic effects are found into the dentin. These alterations in the groups that were dried before laser application are more evident, which confirms the findings of Faria et al. 44 When the Nd:YAG is used in EDTA solution (Fig. 4), changes are found in the root-canal walls, although these are of another nature than those after lasing in dried root canals after rinsing with EDTA. Further research is needed to investigate the composition of this altered dentin. Nd:YAG lasing in NaOCl has no effect on the smear layer, unless the fiber touches the root-canal wall itself. With the present findings, no evidence supports that laser interaction with matter generates cavitation and subsequent pressure waves when the Nd:YAG laser is used in the classic endodontic irrigants (NaOCl or EDTA). In this study, the limitation of the unilateral emission of the laser beam is also substantiated. Only these areas that are exposed to the laser beam demonstrate the typical Nd:YAG morphologic changes of the root-canal wall. It is only when an abundant smear layer exists and in a dried root canal that widespread glazing is found. Hence, the latter can be the result only of heating of the smear layer, leading to evaporation and contraction. When the energy is high, glazing and melting will occur, with carbonization when the exposure to the Nd:YAG laser beam is too intense or too high for the target tissue.
In the present study, the fiber tip was held 1 mm short of the working length at the beginning of the lasing procedure to respect the clinical situation. He et al., 45 investigating the temperature at the outer surface of a root after Nd:YAG lasing at different power settings, clearly demonstrated and confirmed what others 13,16,44 had already pointed out: thermal and morphologic changes seen at the apical third of the roots were greater than those in the coronal third, suggesting that caution should be used when irradiating the apical part of the root, to prevent periodontal injury. They demonstrated that root dentin thickness, especially in the apical third, was an important parameter in the conductance of energy and hence temperature toward the periodontal ligament. 45 Based on their findings, the insertion of the laser fiber 1 mm short of the working length, as done in the present setup, does not interfere with the requested laser–tissue interaction and is a safe way to avoid periodontal damage. 13,16
All samples demonstrated leakage (Table 1). Differences between groups with different cleaning protocols became more obvious when the root tips were resected. In a previous study, a looser seal was observed after Nd:YAG lasing when the smear layer was thoroughly removed. 12,16 The uniform roughened surface left on the dentin walls after lasing of the smear layer appears to favor cement adhesion, and therefore improves marginal sealing. The morphologic changes, such as melting and the formation of glass droplets, also help in occluding the physiologic apex and limits apical ingress or apical leakage. Only when the root tip is removed is the evaluation of true through-and-through leakage along the root canal walls reliable. In this study, the best seal (mean flow and maximum pore diameters) in the resected groups was provided in Group 3r, when a canal was cleaned with NaOCl followed by Nd:YAG lasing. Based on the SEM photographs, a better cleaning was found for Groups 2 and 2r. Apparently the effects of smear-layer modification and evaporation with the Nd:YAG ensure a better seal than smear layer–free root-canal walls with open tubules, as a result of the chelating action of EDTA.
An adequate root-canal obturation is important to ensure a long-lasting successful endodontic result. 17 In a recent study, Hammad et al. 46 investigated the percentage of volume of voids and gaps in root canals obturated with different obturation materials by using a micro-computed tomography (micro-CT). All teeth were filled with a cold lateral condensation technique, and they found 1.02% gaps or voids in laterally condensed gutta-percha obturations. The maximum pore diameter is the most important determinant for the quality of the apical seal. The average length of bacteria varies between 0.2 and 1.5 μm, and toxins are even smaller. 47 Table 1 shows that none of the fillings in this study will inhibit bacterial passage along the root filling. Important is thus that Nd:YAG lasing not only can help to ensure a better seal because of its interaction with the root canal wall, 16,48 but also can enable a more profound disinfection of the root canal than with NaOCl rinses. 49 AH 26, a hydrophobic resin sealer, was used for the root-canal obturation. de Moura-Netto et al. 15 demonstrated that the use of a hydrophobic sealer is to be preferred above a hydrophilic resin sealer because of the dehydration and morphologic changes caused by the Nd:YAG laser irradiation. We must emphasize that not every type of sealer is to be used in association with this irradiation. More research, however, is needed in this field.
At present, an ongoing debate exists over how NaOCl and EDTA may interfere: a number of studies have shown that the combined use of irrigating solutions decreases the effectiveness of chelating agents and might enhance destruction of the dentinal surface. 50 Furthermore, it might have negative effects on the bond strength of adhesive cement to root-canal dentin. 51,52 Based on the present findings, an additional advantage of the Nd:YAG laser technique is therefore its cleaning efficacy and low tendency to produce mineral loss from the root-canal dentin. 53
Conclusion
The present study confirms the findings of a previous study, 16 indicating that an added value is to be gained in obtaining a tighter root-canal seal for the Nd:YAG laser as modifier of the root-canal wall in roots where the smear layer has not been removed by EDTA.
Better sealing results are also obtained after the use of the Nd:YAG laser in dried root canals. In this respect, no benefit accrues from using the Nd:YAG laser in irrigation solutions such as NaOCl and EDTA at the settings of 1.5 W, 100 mJ, and 15 Hz, and lasing 4 times for 5 s, with a dwell time of 20 s.
Author Disclosure Statement
No competing financial interests exist.