
Abstract
Introduction
More recently, curcumin has again received much interest in a wide variety of inflammatory and non-inflammatory diseases including diabetes, cardiovascular diseases, 8 arthritis, and psoriasis, among others. And most recently, because curcumin exerts immunomodulatory, pro-apoptotic, and antiangiogenic properties, 9,10 it has also received tremendous interest as cancer chemopreventative 11 –13 and neuroprotective agents. 14
Vitiligo is a common depigmenting skin condition of which pathogenesis involves a greatly varied array of mechanisms. One of the currently held theories is the overloading of oxidative stress within melanocytes, resulting in the disappearance of these important cells from the epidermis. The anti-inflammatory effect of curcumin mediated through its ability to inhibit cyclooxygenase-2 (COX-2), lipoxygenase, and inducible nitric oxide synthase (iNOS), 5 plus the fact that it also protects the skin by quenching free radicals and reducing inflammation through nuclear factor-KB inhibition, makes this compound attractive as a treatment for this depigmenting condition.
Curcumin is safe even when consumed in large quantities. 15,16 However, due to poor absorption, rapid metabolism, and rapid systemic elimination, very small amounts may reach the skin. 16 Moreover, when applied topically, curcumin's yellow-orange color makes it cosmetically unappealing. Recently, a colorless derivative of curcuminoid, tetrahydrocurcuminoid (THC), could be produced. The anti-oxidative properties of THC have been demonstrated using different in vitro systems. 17 –19 Importantly, when compared, the anti-peroxidation effect of THC was greater than that of curcumin, 17,20 other curcuminoids, and vitamin E. 21 To overcome its water-solubility issues, it was encapsulated in phosphatidylcholine liposomes.
We questioned whether the combined repigmenting action of targeted narrowband UVB phototherapy (TNB-UVB) and the antioxidant properties of topical tetrahydrocurcuminoid cream could result in synergistic therapeutic effects. Therefore, a preliminary randomized evaluator-blind study was conducted to evaluate the efficacy of this combination with that of TNB-UVB monotherapy in stable vitiliginous lesions.
Materials and Methods
The study protocol was approved by the ethics committee of the Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand. Informed consent was obtained from each participant prior to the start of treatment.
Patients
Patients with stable vitiligo, defined as lesions that had not shown either repigmentation or depigmentation within 2 mo prior to enrollment, were eligible for this study. The inclusion criteria were: aged 18 years or older, presence of two similar patches of nonsegmental vitiligo, and an understanding of all information given by a written consent form. A history of skin cancer or photosensitive conditions of any kind, as well as a known allergy to curcuminoids, were our exclusion criteria.
Treatment
The irradiation source used in this study, DuaLightTM (TheraLight Inc., Carlsbad, CA), was a high-pressure mercury lamp, which has been reported elsewhere. 22,23 We used the narrowband handpiece, which emits ultraviolet light primarily in the 311–313 nm waveband.
For each subject, two target lesions within the same anatomical area and preferably on the same side of the body were chosen. One patch was randomly assigned to be treated with combination therapy (group A) and the other with targeted narrowband UVB alone (group B). No placebos were used. Phototherapy took place twice a week, with an interval of at least 1 day, for a maximum of 24 sessions or 12 weeks. The initial fluences were 100 mJ/cm2, followed by 50 mJ/cm2 increments at each successive session, until the very first sign of repigmentation or minimal asymptomatic erythema was observed.
The commercially available curcuminoid cream (GPO curmin, Government Pharmaceutical Organization, Bangkok, Thailand) was purchased in a single batch. Its major ingredient is tetrahydrocurcuminoid (THC) in phosphatidylcholine liposomes. Subjects in group A applied this preparation twice daily and not before UV light treatment.
Assessment
Lesions were mapped and digitally photographed (Fujifilm, FINEPIX S3 Pro, Tokyo, Japan) at baseline and every 4 wk thereafter. Photographs were taken with exactly the same camera settings. The evaluator blinded to the treatment assignment graded the lesions through projections of the digital images. Depigmentation and repigmentation were graded using 9-point scores as follows: − 4, 76–100% depigmentation; − 3, 51–75% depigmentation; − 2, 26–50% depigmentation; − 1, 1–25% depigmentation; 0, no change; 1, 1–25% repigmentation; 2, 26–50% repigmentation; 3, 51–75% repigmentation; and 4, 76–100% repigmentation.
Statistical analysis
Results are presented as mean ± SD. The Wilcoxon signed-rank test was used to compare the degree of repigmentation between the two groups. The level of statistical significant was defined as p < 0.05 (one-tailed). Analyses were performed using SPSS for Windows (V16; SPSS Inc., Chicago, IL).
Results
Ten patients, four male and six female, of skin phototypes III–IV, enrolled and completed the study. The same group of subjects also participated in another study comparing topical tacrolimus and TNB-UVB and TNB-UVB reported elsewhere. 24 The demographic data of these subjects are detailed in Table 1. Four of them had generalized vitiligo, while six had focal vitiligo. The skin phototypes and characteristics of study lesions are outlined in Table 2.
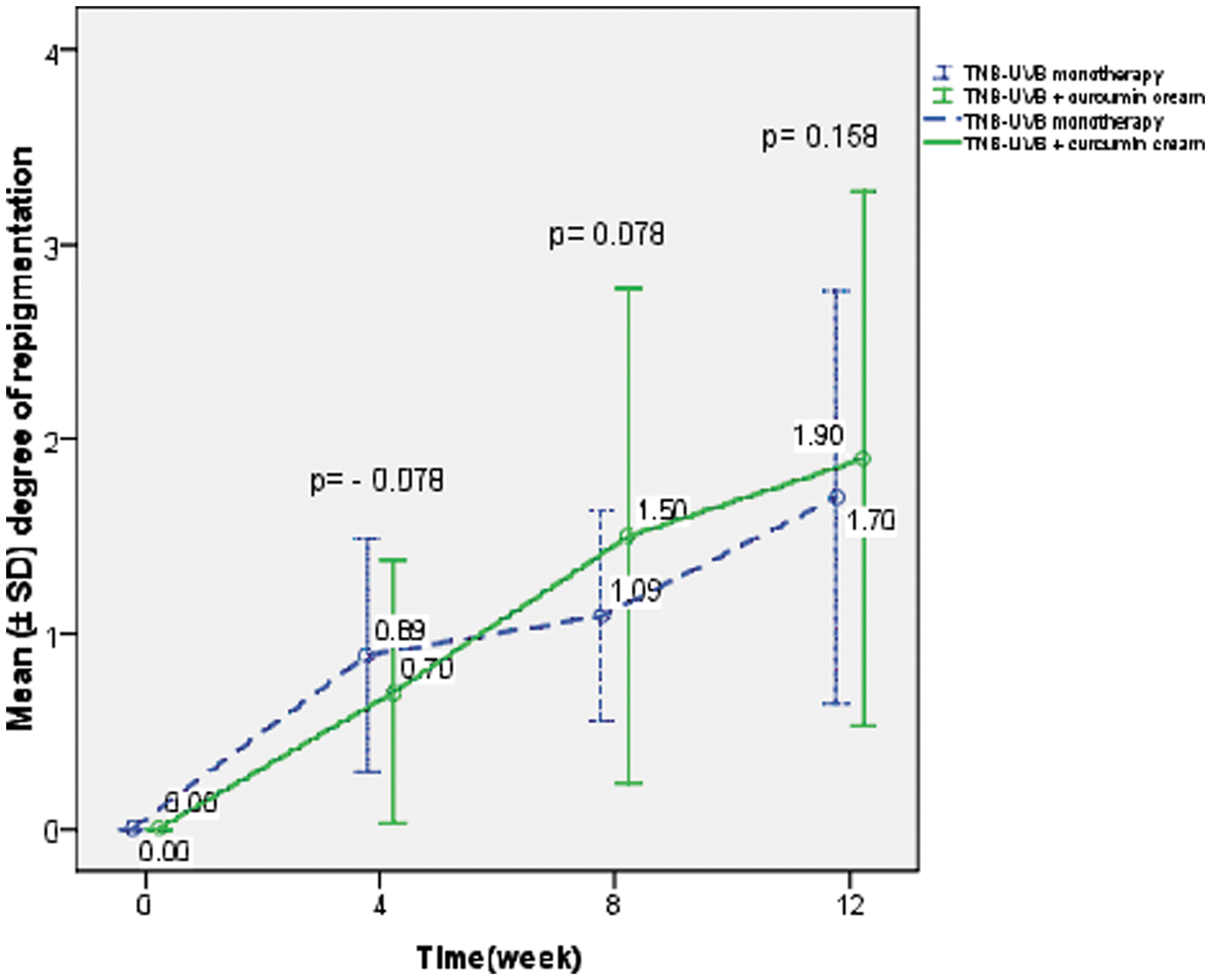
Repigmentation took place in all but one patch, namely in all lesions (100%) receiving TNB-UVB monotherapy (group B) and in 9 of the 10 (90%) lesions that received combination treatment (group A). When compared with baseline, the repigmentation acquired at week 12 was statistically significant in both groups, i.e., an increase of scores by 1.9 ± 1.37 in group A (solid line in Fig. 1; p = 0.001) and 1.7 ± 0.10 in group B (dotted line in Fig. 1; p = 0.006). In most instances, the repigmentation was clearly appreciated by week 4. Interestingly, at this point, the repigmentation was slightly better in the TNB-UVB monotherapy group, where scores improved by 0.70 ± 0.68 and 0.89 ± 0.57 in groups A and B respectively (p = 0.078, Wilcoxon signed-rank test). However, from week 8 onwards, the mean repigmentation scores in group A were better than those of group B, i.e., 1.50 ± 1.27 vs. 1.09 ± 0.57 (p = 0.078, Wilcoxon signed-rank test), and at week 12, the respective values were 1.90 ± 1.37 and 1.70 ± 0.10 (p = 0.158, Wilcoxon signed-rank test).
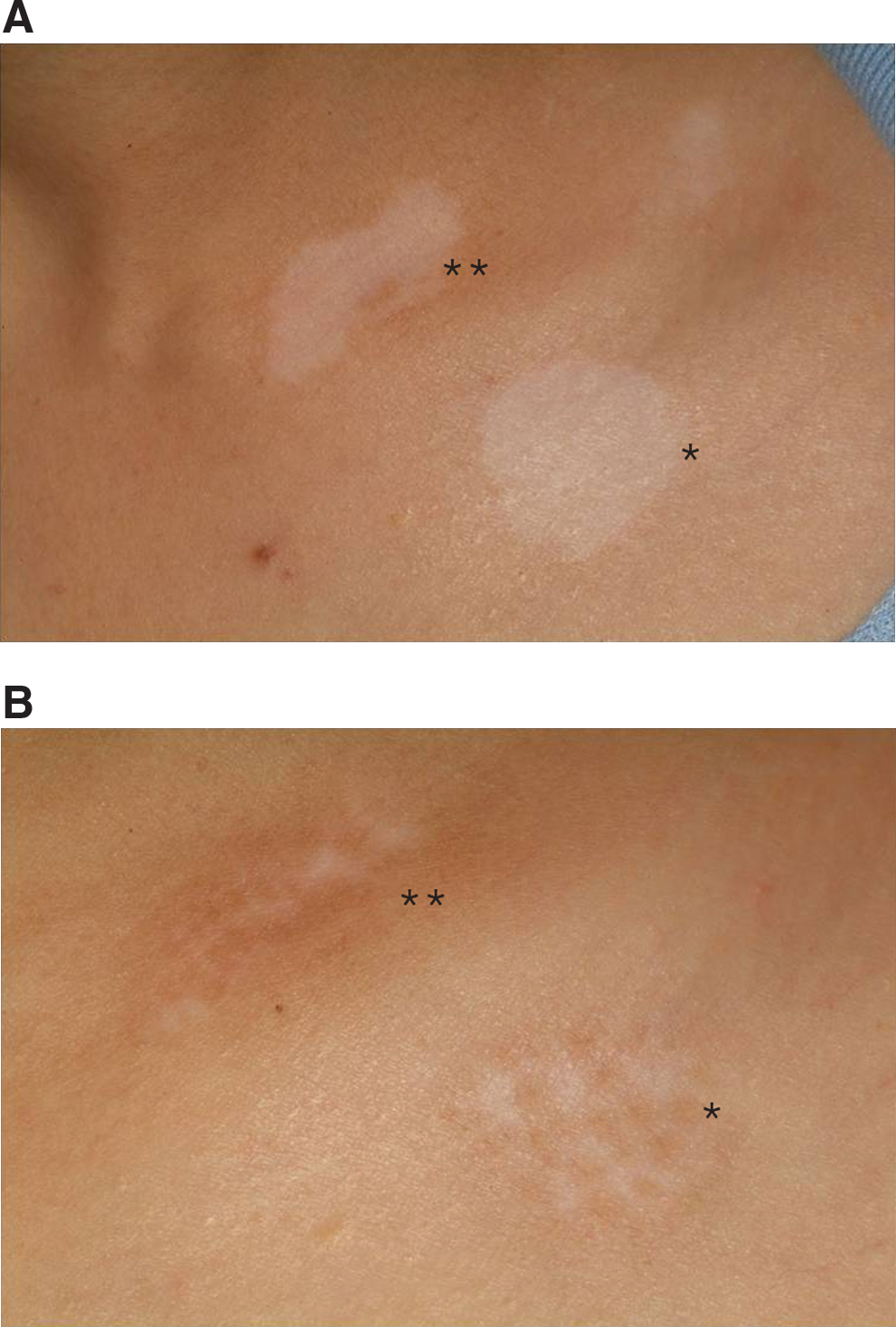
Overall repigmentation. (Color image can be found at
Fig. 2 shows almost complete (grade 4, 76–100%) repigmentation in a lesion receiving THC and 24 TNB-UVB sessions and grade 3 (51–75%) repigmentation in a nearby lesion receiving TNB-UVB monotherapy.
(
Interestingly, we observed a statistically significant inverse association between degree of repigmentation and duration of disease in both group A (p = 0.011, r = − 0.757) and group B lesions (p = 0.005, r = − 0.803). No associations between the degree of repigmentation and sex, age, age of onset, type of vitiligo, skin phototypes, or anatomic location of lesions were demonstrated.
Minor and well-established adverse effects, such as asymptomatic erythema, itching, burning sensation, and hyperpigmentation at sites of treatment, were observed at approximately equal frequencies in both modalities. The cumulative UVB doses were essentially the same in the two treatment groups (Table 3).
Discussion
Our study demonstrated that the combination treatment of TNB-UVB plus THC cream was more effective than targeted narrowband UVB monotherapy for the treatment of vitiligo. To our knowledge, this is the first study of its kind to investigate the synergistic effect of this particular combination.
To date, NB-UVB therapy is one of the most effective treatment modalities for vitiligo. More recently, targeted UV therapies, including the 308-nm excimer laser 25 –38 and other targeted UVB light systems 22,23,39 –41 whereby UV fluence is delivered specifically to the lesional skin, are valued greatly because the unaffected skin is not exposed and because of the rapidity of repigmentation these modalities can induce. 22,23,42 –44
To improve the efficacies of targeted UV treatments further, several authors have combined light treatment with topical agents, most notably tacrolimus, and concluded that the combination treatment was faster and more effective at repigmenting vitiliginous lesions than targeted phototherapy alone. 42 –44
Most recently, in 2008, Lotti et al.
44
reported a study involving 458 vitiligo patients that evaluated the efficacy of various topical treatments, i.e., 0.1% tacrolimus ointment, 1% pimecrolimus cream, 0.05% betamethasone dipropionate cream, calcipotriol ointment, and 10%
Our study showed that the addition of THC to TNB-UVB enhanced the repigmenting capacity of the latter, although, due to the relatively small sample size, the difference did not quite reach statistically significant levels. This is probably due to several factors, which are discussed below.
As mentioned in the tacrolimus/excimer studies by Passeron et al. and Kawalek et al., lesions within the “UV-sensitive areas,” namely, the face, neck, and trunk, respond much more readily than those located over the bony prominences and extremities, the so-called UV-resistant areas. 42,43 When UV-sensitive areas were analyzed separately, Kawalek et al. found no statistically significant difference in clinical response between the combination treatment and laser monotherapy. 43 It is thus not surprising that our study lesions, all located in the UV-sensitive areas, responded well to the UV monotherapy and no significant difference was observed when THC was added. Another study by Ostovari et al. demonstrated that all lesions treated with the combination repigmented, while none on the tacrolimus arm did so. 45 Similarly, Lotti et al. found that all of the topical treatments, when applied alone, produced much less repigmentation than when UVB micro-phototherapy was combined, 44 lending further support that UV therapy may play a more significant role in such combination.
Second, the duration of our study was limited to 12 wk to investigate the role of this curcuminoid during the initial phase of repigmentation. As pointed out earlier, the combination treatment started to show efficacies from week 8 onwards. Thus extending the duration of treatment might have made this difference more pronounced, as seen in the 6-mo study of Lotti et al. 44
Another point worth discussing is an observation derived from a recent study conducted in India by Schallreuter and Rokos. In that study, the repigmentation effect of topical pseudocatalase and UVB phototherapy for vitiligo in their subjects was not as predictable compared with when such a combination was used elsewhere in the world. They proposed that curcumin consumed in large amounts in Indian food may paradoxically result in the overproduction of reactive oxygen species. Upon avoidance of turmeric in the diets, six of their eight subjects obtained excellent repigmentation. 46 Whether this is also true for topical application of THC is not clear at this point.
Our final speculation is whether curcuminoids, with their radioprotective properties, might allow better tolerance to UVB, as reported with other anti-inflammatory agents, such as Polypodium leucotomos. 47,48 In future studies, it will be most interesting to investigate a more aggressive treatment protocol involving larger increments of UV doses at each treatment.
Conclusion
We have demonstrated that topical THC cream might add benefits to the treatment of vitiligo with targeted NB-UVB phototherapy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.