
Abstract
Introduction
Various agents have been used as desensitizers for hypersensitive teeth, including toothpastes containing arginine and potassium ions; formulations containing sodium floride, silver nitrate, formaldehyde, strontium chloride, and potassium salts; oxalates, resin-bonding agents, and abrasive dentifrices. 9 –14 Conventional therapy for hypersensitive teeth is based on using topically applied desensitizing agents, either professionally or at home. However, most treatments are either ineffective or last for only a short time.
A variety of lasers such as He-Ne, GaAlAs (diode), CO2, Nd:YAG, and Er:YAG have been evaluated in DH treatment in the past. The first laser use for treatment of DH was reported by Matsumoto et al. 3 with Nd:YAG and the 780-nm diode lasers. The use of diode lasers in dental therapy has increased dramatically in recent years. Diode laser has been used as an efficient means for the treatment of DH by many investigators. 15 –26 Several wavelengths (ranging from 660 to 900 nm) of diode laser have been used for the treatment of DH. 3 It is postulated that this type of low-output power lasers mediates an analgesic effect related to depressed nerve transmission. 3 According to physiological experiments using the diode laser at 830 nm, this effect is caused by blocking the depolarization of C-fiber afferents. 20 GaAlAs laser emissions at 904 nm have an analgesic effect on the cat tongue, although the mechanism remains unclear. 25 Diode laser irradiation at a maximum power of 60 mW does not affect the enamel or dentin surface morphologically, but a small fraction of the laser energy at 830-nm wavelength is transmitted through enamel or dentin to reach the pulp tissue. 26 The treatment-effectiveness rate of these lasers was dependent on the output power, and ranged from 30% to 100%. 3 In most of them, despite varieties in methods and kinds of laser, a relative success was described.
Treatment of DH by the diode laser revealed that the laser interaction with the dental pulp causes a photobiomodulating effect, increasing the cellular metabolic activity of the odontoblast and obliterating the dentinal tubules with the intensification of tertiary dentin production. 15,18 Diode lasers provide cold thermal low-energy wavelengths with a minor temperature increase of <0.1°C. 19 These wavelengths are believed to stimulate circulation and cellular activity and to provide various effects such as antiinflammatory, vascular, muscle relaxation, analgesia, and tissue healing. 19 However, because of the great varieties in methods and types of lasers, it is impossible to propose a definitive method to treat DH.
Toothpastes containing potassium ions have been shown by several clinical studies to be effective in reducing DH. 11 –14 Potassium ions are thought to act by blocking the action potential generated in intradental nerves and to raise the pain threshold of pulpal nerves to hydrodynamic stimuli. 27 –29
New treatments for DH therapy must be developed. Although the individual desensitizing effects of diode laser and desensitizing dentifrice have been shown, the combined effect of diode laser and desensitizing dentifrice on DH remains uncertain; this determination was the main aim of the present study. Furthermore, it also isimportant to compare the efficiency of the lasers with that of commonly used agents. Therefore, the purpose of this study was to evaluate and compare clinically the efficacy of desensitizer toothpaste alone and in combination with the diode laser in the management of DH, as well as both the immediate and late therapeutic effects to teeth with gingival recessions.
Materials and Methods
The research protocol and consent form were initially submitted to the Ethics Committee, and The Institutional Internal Review and Ethics Board at the Atatürk University, Faculty of Dentistry approved the study (AU-IIREB reference code:021). All participants provided written informed consent.
The study population consisted of 13 patients with 52 hypersensitive teeth with Miller's Class I or Class II gingival recession (seven women and six men; aged 16–48 years; mean age, 31.2 ± 8.8 years) who visited the periodontology department of the Faculty of Dentistry at Atatürk University.
Selection of subjects and test teeth
Inclusion criteria
Patients in good systemic health with clinically elicitable DH who were reliable in their response to test measurements were included in the study. All experimental teeth had Miller's Class I or Class II recessions. 30
Exclusion criteria
Patients with chronic or debilitating disease with daily pain episodes; those who were taking any analgesic, anticonvulsive, antihistaminic, sedative, tranquilizing, or antiinflammatory medications in the 72 h preceding treatment; those who had used any desensitizing toothpaste or mouthwash in the last 3 months; and those who had been given periodontal surgery in the last 6 months were excluded from the study. Teeth with cracked structures, carious lesions, restorations, nonvital///, and active periodontal disease were excluded.
Pain and DH assessment
A visual analogue scale (VAS) was used to measure DH. The VAS was administered in a standard manner, with the initial explanation given by the same clinician. All patients were asked to define their level of DH by using a VAS consisting of equal units from 0 to 10 (a line of 10 cm). On this scale, 0 and 10 represented “no pain/discomfort” and “worst pain/discomfort imaginable,” respectively. All pain assessments were performed in the morning in the same clinic, free of extraneous noise, music, or conversation. Patients were asked to mark the degree of pain they experienced by directing an air blast to the root surface before and after treatment of DH. Before and after each session, we gave the patient a separate sheet of paper containing the printed interval scale (a line of 10 cm) so that he or she could not be influenced by the previous results. Data from the VAS were recorded by measuring in millimeters the distance between zero point and the sign marked by the patient on the 10-cm line. Reproducibility for the VAS was completed on two separate occasions by five patients. A strong correlation was found between the two responses in both procedures (Spearman's rho >0.93; p < 0.001).
DH was assessed by means of air stimulus. The clinician directed an air blast (60 pounds per square inch, 22°C) derived from a dental syringe to the root surface for 1 sec. He held the syringe perpendicularly 2–3 mm from the root surface. After this stimulation, the patient again scored the pain by using the VAS. The air pressure, temperature, and distance between the root surface and the tip of the air syringe were kept constant for all cases in both pretreatment and posttreatment diagnosis of DH. All stimuli were given by one investigator in the same dental chair with the same equipment, yielding similar air pressure and temperature each time.
Treatment
After the baseline pain assessment, the teeth were randomly assigned to test group: desensitizing toothpaste, and diode laser, or the control group: desensitizing toothpaste. Twenty-six test-group teeth, including six incisors, six canines, 11 premolars, and three molars, and 26 control-group teeth, including six incisors, seven canines, nine premolars, and four molars were subjected to one treatment modality in each group.
All the patients received a dental prophylaxis and instruction in brushing technique, and they used a standardized soft-filamented toothbrush and desensitizing toothpaste (Sensodyne F; GlaxoSmithKline Ltd, UK) during the 3 months of the trial. In addition, the patients were instructed to cover the entire length of the filament section of the toothbrush with the toothpaste and to brush their teeth twice daily, in the morning and in the evening, for 3 min each time throughout the study. Sensodyne F is a toothpaste containing a desensitizing agent [3.75% potassium chloride (KCl)], an anticaries agent [0.80% sodium monofluorphosphate (SMFP)], and an antiplaque-antiinflammatory agent (0.30 triclosan) for DH, gingival health, and plaque formation, currently marketed in Turkey. All participants completed the study and reported 100% compliance.
Before laser therapy, all of the teeth received scaling, root planing, polishing, and brushing with desensitizing toothpaste. Afterward, relative isolation of the region was carried out with the aid of a cotton roll and the drying of the buccal surface with gauze before each treatment session. The vitality of teeth was tested with a pulp tester (Digitest D626D; Parkell, Farmingdale, ) before and after each treatment session. The patients did not know what kind of therapy each tooth was receiving.
Lasing was performed by using Doctor Smile erbium & diode laser machine (Doctor Smile erbium&diode; Lambda Scientifica, Vicenza, Italy). Teeth subjected to diode laser treatment were radiated with a laser beam of 100 mW, 25 sec, (0.1W × 25 sec = 2.5 J), 808 nm (Optical Fiber, diameter: 300 μm, 2 J/cm2), with continuous-emission form, noncontact mode (2 mm from the surface), perpendicular to the surface for scanning movements in the region of exposed root surfaces. The laser application was performed according to the instructions given by the manufacturer. When the lasers were in use, protective eyewear of the appropriate optical density was worn by the investigators and patients.
The laser therapy was performed by one investigator, and the pain was assessed by another investigator.
Study design
The treatments were carried out in three sessions, with intervals of 14 days between sessions, during a period of 30 consecutive days. The measurements were performed before each treatment session and at 30 min after the laser application to verify the capacity, the extent, and the duration of desensitization after irradiation. This result was named the immediate effect. Additional measurements also were performed at 15, 30, and 60 days after the conclusion of treatment to assess the extent of desensitization obtained with the different therapies. This result was called the late effect.
Statistical analysis
Descriptive statistics including means and standard deviations were calculated for both groups. The data thus collected were assessed by using SPSS 16.0 statistical software (SPSS, Chicago, IL). The Mann–Whitney U test was used to compare groups and controls, and the differences in the mean VAS scores were calculated. The differences in mean VAS scores between pretreatment and 30-min posttreatment were evaluated by using Wilcoxon's signed-ranks test. The Friedman test was used to assess the differences in mean VAS scores for the late effects of treatment (at 15, 30, and 60 d).
Results
The mean VAS scores before and after treatment with DH to the test group and control group at different times are showed in Table 1 (Fig. 1).
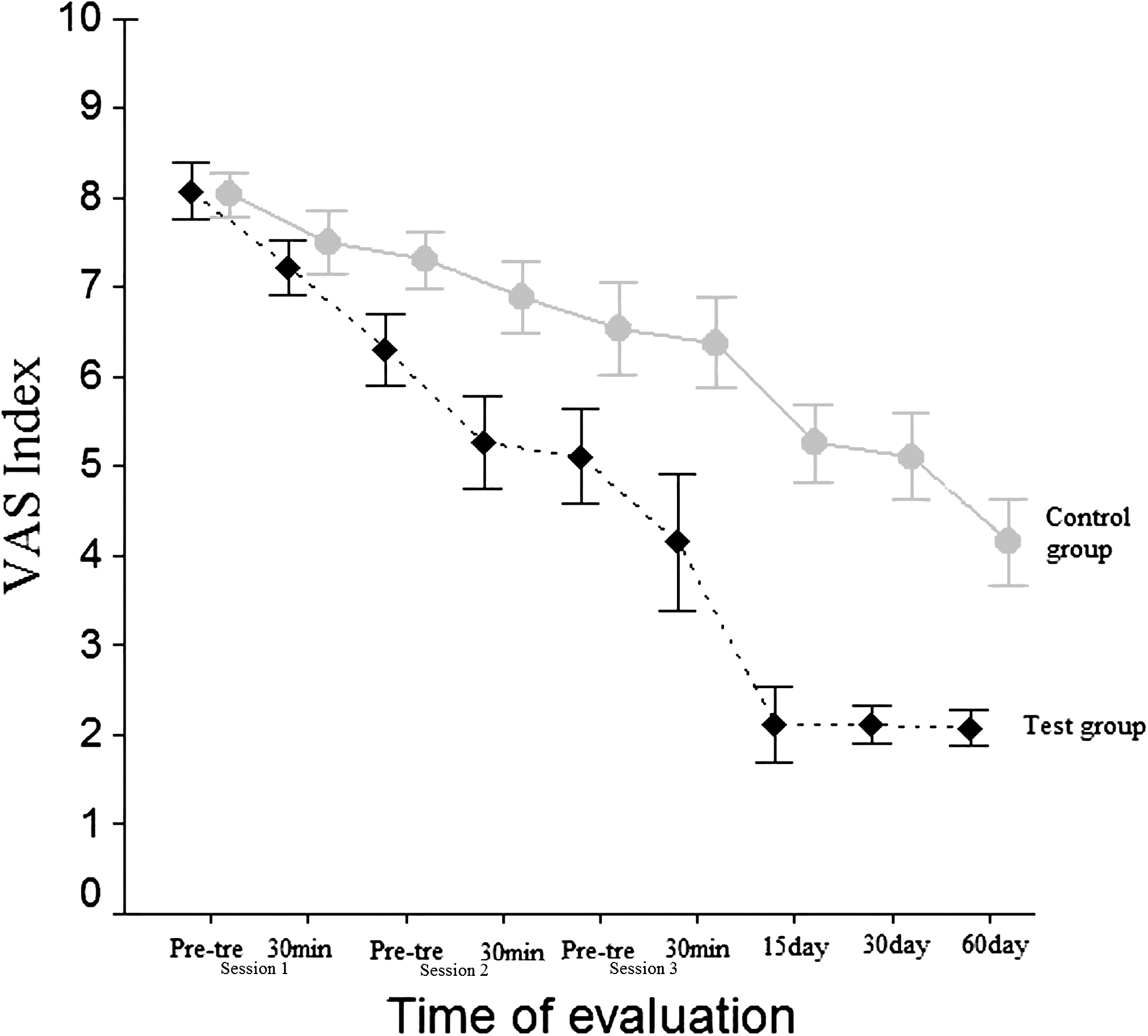
Visual Analogue Scale index changes in the two groups at different times.
p < 0.05; b p < 0.01; c p < 0.001: significant differences between pretreatment and 30 min (Wilcoxon's signed-ranks test).
The mean VAS score in pretreatment for session 1 for test group was 8.08 ± 0.78. The corresponding score for the control group was 8.04 ± 0.59. These scores were not statistically different (p > 0.05). The mean VAS score for 30 min of session 1 for the test group was 7.23 ± 0.75, and the corresponding score for the control group was 7.50 ± 0.84, which were not statistically different (p > 0.05).
Compared with the pretreatment for session 1, a significant decrease in mean VAS score in 30 min of session 1 occurred for the test and control groups (7.23 ± 0.75 and 7.50 ± 0.84, respectively; p < 0.01).
The mean VAS score in pretreatment for session 2 for the test group was 6.31 ± 0.95, and in 30 min of session 2, the mean VAS score was 5.27 ± 1.26 (p < 0.001). The corresponding scores for session 3 were 5.12 ± 1.28 and 4.15 ± 1.85 (p < 0.05). In the control group, the corresponding scores were 7.31 ± 0.77 and 6.88 ± 0.97 for session 2 (p < 0.01) and 6.54 ± 1.25 and 6.38 ± 1.21 for session 3, respectively (p > 0.05).
Table 2 shows the mean VAS scores for late effect in the follow-up periods of 15, 30, and 60 days after the conclusion of the treatment for DH to the test and the control group (Fig. 1).
p < 0.05. Significant differences between 15, 30, and 60 days (Friedman test).
On the day 15, the test group had a mean VAS score of 2.12 ± 1.01, compared with the control group with a VAS score of 5.27 ± 1.08, which was statisticaly significant (p < 0.001). In addition, the control group had a significant decrease in mean VAS score on day 60 (p < 0.05).
The effects of treatment were demonstrated for both groups of testing sensitivity, and the effects were comparatively stronger. The vitality tests of the teeth were the same before and after laser treatment.
Discussion
DH is a frequently encountered enigma in dentistry. It can be a major problem for periodontal patients, who frequently have gingival recession and exposed root surfaces. This study provides information about the clinical effectiveness of diode laser and desensitizing toothpaste in the treatment of DH.
DH is a pain sensation and is difficult to quantify. In the present study, VAS was used to assess DH. In previous clinical studies, several investigators used VAS, because it is simple to understand by patients, more sensitive in discriminating between various treatments and changes in pain intensity, and suitable for use in the evaluation of the irritant response in hypersensitivity studies. 12,16,22
The results of the present clinical trial demonstrated that a significant decrease in DH in both groups over the 12-week study period compared with the baseline. The results especially illustrate the effectiveness after cold air-blast stimulation. In a previous clinical study, it was demonstrated that the GaAlAs (diode) laser is also an effective device in reducing DH with air spray. 22 A significant reduction of the VAS scores from 8.08 ± 0.78 to 2.08 ± 0.47 was shown in the present study (p < 0.001). Our findings confirm the data of the earlier studies in this field. 15 –19,22 –24
DH has a multifactorial etiology, and generally, more than one factor is found to be associated and active in this painful manifestation. Therefore, many products have been tested in DH, but the results have been variable. Currently available treatment involves multiple agents with varying degrees of effectiveness. Therefore, the evaluation of a further modality to substitute for or augment conventional dental therapy is warranted. Research is now beginning to focus on the use of lasers to manage DH.
The laser parameters contributing to its effect are as follows: power (W), exposure time (seconds), energy density (J/cm2), pulsed versus continuous wave, contact or defocused irradiation, laser-beam divergence, and energy per point and total. 3 As a laser beam strikes a target-tissue surface, the light energy can be effected in four ways: reflected, transmitted, absorbed, and scattered. 3
Various studies reported a lack of significant pulp damage or thermal alterations after irradiation of the root surface. 3,23,24 It has been reported that healthy pulp tissue is not injured thermally if the laser equipment is used at a correct parameter, so that any temperature increase within the pulp remains <5°C. 3 Matsumoto et al. 31 demonstrated that 780-nm diode laser, 30 mW for 3 min, caused no thermal or other damage to pulp tissues in monkeys. In addition, according to Arrastia et al., 32 GaAlAs laser irradiation at the parameters of 30 mW at 780-nm wavelength, 60 mW at 830-nm wavelength, and 10 W (pulsed) at 900-nm wavelength do not cause significant intrapulpal temperature increases. In our study, none of the teeth treated with laser showed collateral effects, which confirms the safety of this type of treatment.
In clinical research by Sicilia et al., 23 they used a diode laser with a wavelength of 810 nm at an output power of 2.5 mW for 60 sec for the root surfaces of selected teeth, and they reported a significant reduction in DH after diode laser treatment. In a previous study, Pesevska et al. 24 used an 670-nm low-level diode laser at 100 mW of power, contact mode for 20 sec (0.1 W × 20 sec = 2 J), and they reported that low-level diode laser treatment can be successfully used for treatment of DH after scaling and root planing. In the current study, we used diode laser with a wavelength of 808 nm, and the laser energy was applied at 100-mW power for 25 sec, for a total dose of 2.5 J. The results of the present study indicate that noncontact-applied GaAlAs laser is effective in reducing DH. Marsilio et al. 18 performed a double-blind study on the effect of GaAlAs laser application at the maximum (5 J/cm2) and minimum energy densities (3 J/cm2) recommended by the manufacturer for the treatment of DH. They reported that the GaAlAs laser was effective in reducing the initial DH. No significant difference was found between minimum and maximum applied energy density. GaAlAs laser has been tested with different output-power levels, combining wavelengths ranging from 660 to 900 nm, and application periods from 60 to 150 sec. 3 The treatments performed with lasers at different bands of red and infrared wavelength demonstrated a certain degree of desensitizing capacity. Ladalardo et al. 16 performed a double-blind study on the effect of two types of diode-laser application for the treatment of DH. They reported that the immediate and late therapeutic effects of the 660-nm red-diode laser were more evident compared with those of the 830-nm infrared-diode laser. Matsumoto et al. 33 reported good results in patients treated with red and infrared lasers who initially had light and moderate pain levels. The treatment was not effective in the cases that had shown maximum initial levels of pain. The results of the present study are in agreement with the results of previous studies. 19,34,35 We can conclude that both red- and infrared-wavelength diode lasers have been effective in the treatment of DH.
In the control group, the mean VAS scores showed a decrease from pretreatment to posttreatment at all treatment durations, which was statistically significant. These findings are similar to results obtained by Pereira and Chava, 12 who used the desensitizing dentifrice and achieved a reduction in DH with air by 5.06 to 1.44. Similar observations were made by several investigators. 11,13,14 The results obtained in the present study seem to suggest that desensitization of teeth with gingival recession with the combination of diode laser and desensitizing dentifrice was more evident.
It has been assumed that DH may be reduced by different mechanisms during two treatments tested in the present study. For desensitizing toothpaste whose active ingredient is potassium chloride, potassium ions are thought to act by blocking the action potential generated in intradental nerves and to increase the pain threshold of pulpal nerves to hydrodynamic stimuli. 27 –29 Recently, the GaAlAs (diode) laser was introduced in treating DH by means of inducing changes in neural transmission networks within the dental pulp, which may stimulate the normal physiologic cellular functions. 15,17 In addition, these lasers stimulated the production of sclerotic dentin, thus promoting the internal obliteration of dentin tubules. 36 A previous study reported that GaAlAs (diode) laser blocks the depolarization of C-fiber afferents. 20 Moreover, besides the immediate analgesic effect, the laser therapy may stimulate the normal physiologic cellular functions. 21 It would be interesting to study the long-term effects of reducing DH from diode-laser treatment, because the mechanism induces the sclerotic dentin layer. In the test group, the mean VAS score showed a decrease from pretreatment to posttreatment at all treatment durations, which was statistically significant. Our findings confirm the data of the earliest studies in this field. 15 –20
Research is now beginning to focus on the use of lasers to manage DH on the grounds that laser treatment is more comfortable and faster than conventional methods. Nevertheless, the diode laser and desensitizing dentifrice could be clinically advantageous methods to reduce DH because of their rapid clinical effectiveness, with no adverse reactions observed. As such, they could be suitable for routine clinical treatment for DH. The diode laser treatment seems to be benefical and can be an alternative treatment for DH. However, the laser is found in only some clinics because of its high cost. Laser devices in dental clinics may become more widely used to relieve of several disorders of the oral and maxillofacial region.
Conclusions
Within the limitations of the present study, a significant effect of combined desensitiser toothpaste and diode laser therapy occurs in the treatment of desensitization of teeth with gingival recession. Desensitizer toothpaste appears to have therapeutic potential to alleviate DH. Conversely, diode laser can be used to reduce DH. Further studies are needed to evaluate the long-term stability of the obtained positive results.
Footnotes
Author Disclosure Statement
No competing financial interests exist.