
Abstract
Introduction
A previous study examined the effects of laser irradiation on wound healing in diabetic and nondiabetic mice, in which wounds were covered with Tegaderm HP dressing (greater adhesiveness than Tegaderm W) and with newer adhesive agents. 11 The dressing and adhesive agents held the wounds open in a large proportion of mice, and healing occurred mainly by reepithelization and granulation tissue formation. Such wounds were referred to as being splinted. Effects of two levels of laser irradiation on healing were compared with those of wounds not irradiated (controls). Wounds were irradiated by using a laser (660 nm, continuous wave; Lasotronic GmbH, Hengersberg, Switzerland), average output 18 or 80 mW, 20 sec/day for 7 days; for an irradiated area of 32–43 mm2, this represents an energy density of about 1 J/cm2/day or between 3.7 and 5.0 J/cm2/day, respectively. 11 The procedure used for dressing the wounds was developed from a pilot study. This article describes the methods tested for dressing excisional wounds in the pilot study and a statistical analysis of wound outcomes from histologic sections of wounds, in control diabetic and nondiabetic mice, covered with Tegaderm HP dressing.
Materials and Methods
Mice
Diabetic and nondiabetic mice (BKS.Cg-m+/+ Leprdb , The Jackson Laboratory, Bar Harbor, ME; stock number 000642) were used from a small breeding colony at the University of Otago. Both male and female mice were included. Diabetic mice were selected on the basis of age and body weight: the majority were 11–16 weeks old and weighed ≥40g. Nondiabetic mice were similarly selected: most were 14–16 weeks old and weighed ≥27 g. Diabetic mice are leptin receptor deficient and represent a model of type 2 diabetes characterized by hyperglycemia, obesity, and impaired wound healing. 7,12 Nondiabetic mice are lean, and wound healing is not impaired. 7
Before surgery, mice were housed together according to date of birth and sex; after surgery, they were housed in individual cages. Mice were kept under standard laboratory conditions (20–22°C, 12 h/12 h light/dark cycle), supplied with food and water ad libitum. Procedures were approved by the Animal Ethics Committee, University of Otago.
Experimental wound model
Mice were anesthetized with halothane (4% induction, 2% maintenance), and the left flank was shaved, depilated by using Veet cream (Reckitt Benckiser, West Ryde, New South Wales, Australia), and skin disinfected with povidone iodine (Betadine). A full-thickness wound was made on the left flank in each animal by using a sterile 5-mm-diameter biopsy punch (Miltex Inc., York, PA; product ref. 33–35), and the wound extended down to the fascial layer over the abdominal musculature. Wounds were covered with Tegaderm HP dressing (3M New Zealand Ltd, Auckland, New Zealand), and buprenorphine (Temgesic) (0.1 mg/kg body weight) given subcutaneously for pain relief. Mice were returned to their cages and kept warm by placing the cages on a heating pad until the mice were fully recovered from the anesthetic. Day of wounding was day 1. All steps in creating and covering the wounds were performed under aseptic conditions by the same operator to minimize variability.
In early studies, some mice died under halothane anesthesia. On veterinary advice, all mice were subsequently given atropine (0.05 mg/kg body weight) subcutaneously at least 10 min before exposing to halothane. No further instances occurred of mice dying under halothane.
Methods of covering wounds with Tegaderm HP dressing
A pilot study was performed with six male diabetic and six male nondiabetic mice, aged 11–16 and 14–16 weeks, respectively. Tegaderm HP dressing (25 × 25 mm) was used to cover the wound, by using one of five methods described subsequently and illustrated in Fig. 1. After placing the Tegaderm dressing over the wound and adjacent skin, gentle pressure was applied to the edges of the dressing to maximize its adherence to the skin. Adhesives used were Cavilon No Sting Barrier Film (3M New Zealand Ltd., Auckland, New Zealand) and Mastisol (Ferndale Laboratories Inc., Ferndale, MI). Both have been used clinically to improve the attachment of Tegaderm dressings; Mastisol was reported by the manufacturer to have 7 to 10 times the stickiness of benzoin compound tincture.
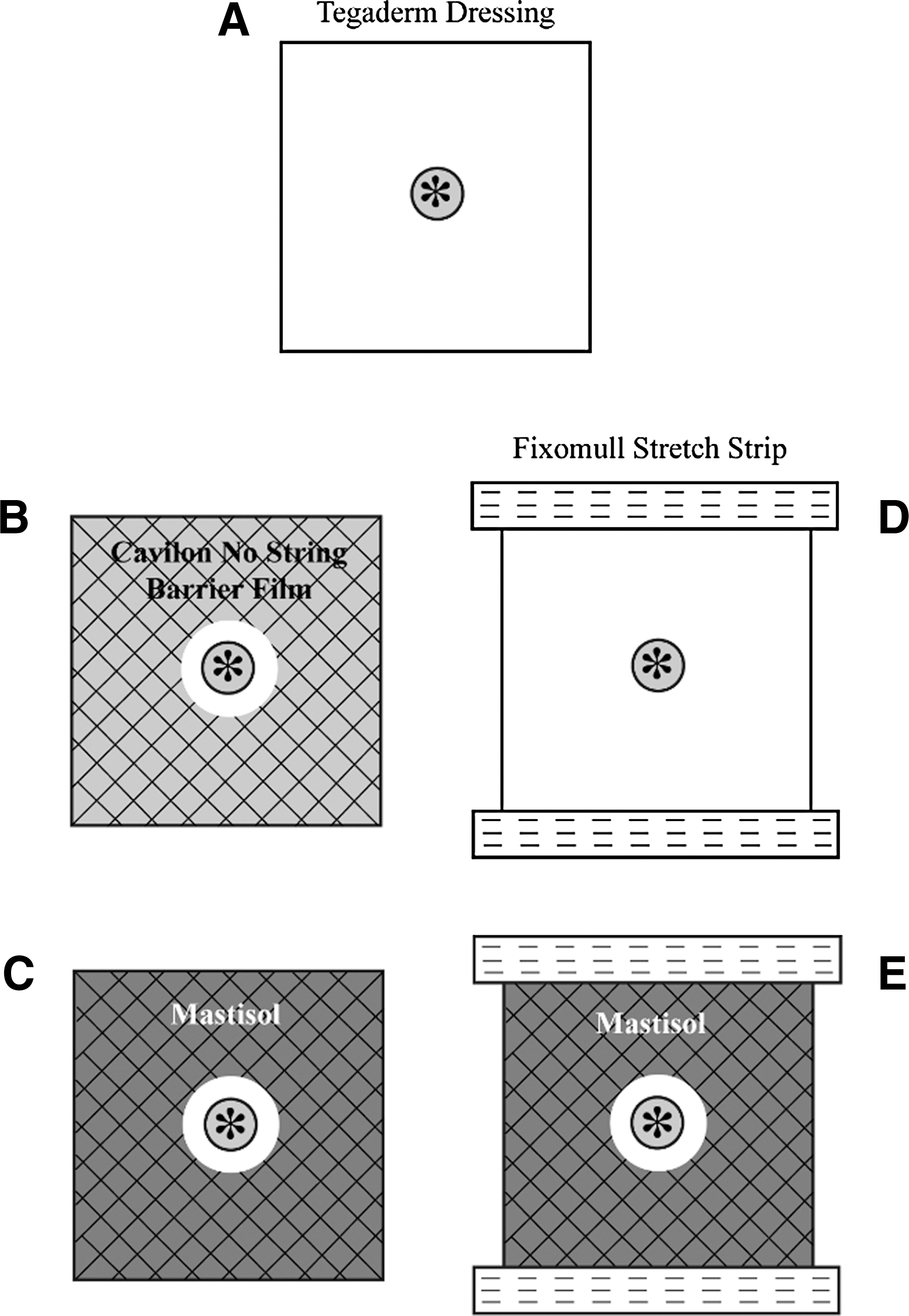
Schematic representation of the five methods trialed for covering full-thickness excisional wounds in mice with Tegaderm HP dressing (25 × 25 mm). (
Method A: Tegaderm dressing alone
Method B: Cavilon No Sting Barrier Film and Tegaderm dressing.
Cavilon No Sting Barrier Film was applied as a thin film to the skin 4–5 mm from the wound margin and allowed to dry. This was to increase the adhesiveness of Tegaderm dressing to the skin and to reduce any skin sensitivity. This method mimics best hospital practice, where it might be difficult to keep the wound covered with Tegaderm dressing (e.g, diaphoretic patients).
Method C: Mastisol adhesive and Tegaderm dressing.
Mastisol was applied to the skin around the wound margin and allowed to dry for 30 sec to improve the adhesion of the dressing.
Method D: Tegaderm dressing and two strips of Fixomull Stretch.
Two narrow strips of Fixomull Stretch (BSN Medical GmbH & Co., Hamburg, Germany; 6–7 × 30–35 mm) were attached along the cranial and caudal edges of the dressing and to adjacent skin, and gently pressed down onto the skin, to prevent damage to the edges of the dressing by the mouse.
Method E: Mastisol adhesive and Tegaderm dressing and two strips of Fixomull Stretch.
Mastisol was applied to the skin around the wound margin and allowed to dry for 30 sec. Two narrow strips of Fixomull Stretch (6–7 × 30–35 mm) were attached along the cranial and the caudal edges of the dressing and to adjacent skin and gently pressed down onto the skin.
Daily monitoring of mice for the presence and condition of the Tegaderm dressing was performed and recorded. When necessary, dressing reattachment was carried out by applying Mastisol and Fixomull Stretch strips. When dressing renewal was required, the previous dressing was gently removed with forceps, and the skin around the wound cleaned before covering the wound with a new Tegaderm dressing by using one of the five methods.
Based on the pilot study, an optimized procedure was developed for covering wounds, and used for attachment and management of wound dressings in subsequent laser-irradiation studies. A total of 23 diabetic (13 males, 10 females) and 13 nondiabetic mice (all males) comprised the control (nonirradiated) animals, and the findings for these animals are described here. In a previous article, 24 diabetic (nine males, 15 females) and seven nondiabetic mice (six males, one female) were laser irradiated. 11
Wound repair and analysis
Photography of wounds.
Photographs were taken on days 1, 4, 7, 10, and 14 by using a Fujifilm FinePix S3 Pro digital camera (Fuji Xerox New Zealand, Auckland, New Zealand) with a micro-Nikkor 60-mm f/2.8D lens (Nikon Corporation, Tokyo, Japan). A stainless-steel ruler placed alongside the wound enabled the calibration of photographs.
Histology of wounds.
Mice were euthanized on days 10 or 14, and wounds were excised with sharp scissors and fixed in 10% neutral buffered formalin. Wound specimens were divided along the greatest diameter and underwent routine histologic processing, embedding in paraffin wax, and sections cut at 4 μm stained with hematoxylin and eosin. Sections were examined under an Olympus AX70 microscope (Olympus New Zealand Pty Ltd., Auckland, New Zealand) and photographed by using a mounted Spot RT color camera (Diagnostic Instruments, Inc., Sterling Heights, MI). Histologic appearance of sections was reported, and semiquantitative analysis (score, 1–15) was performed by using a previous scheme. 8 Images were analyzed for dermal gap (DG) and epithelial gap (EG). DG was defined as the distance across the wound between edges of the intact dermis, and EG as the distance between advancing edges of epithelial regrowth at the edges of the wound. Extent of epithelial regeneration was calculated as DG − EG, and percentage (%) epithelialization, as 100 × (DG − EG)/DG. Evaluation and analysis of wound sections was performed by two independent examiners and checked by a pathologist blinded to the coding of the sections. For two or three mice, values for DG, EG, and histologic score were measured in consecutive sections of wound specimens to validate the procedure.
Wound depth and diameter of excised skin samples from diabetic mice (males, n = 3; females, n = 3) and nondiabetic mice (males, n = 3) were measured from histologic sections prepared as described.
Statistical analyses
Analysis of variance (ANOVA) was used to test for differences in means of DG, EG, DG − EG, percentage of epithelialization, and histologic score between diabetic and nondiabetic mice. A χ2 test was used to test for differences in numbers of splinted wounds compared with nonsplinted wounds. Significant findings are reported at the level of p < 0.05.
Results
Experimental wound model
Histologic sections of skin excisional biopsies confirmed that the wounds had been made down to the level of fascial plane just below the panniculus carnosus muscle.
Development of an optimized procedure for covering wounds
Methods for the initial covering and renewals of Tegaderm HP dressings for diabetic mice (n = 6) and nondiabetic mice (n = 6) in the pilot study are shown in Table 1. For all diabetic mice, an attempt was made to keep wounds covered with Tegaderm HP dressing for the whole length of the study (to day 14). For nondiabetic mice, wounds had almost completely closed by day 9, and no further attempt was made to keep wounds covered.
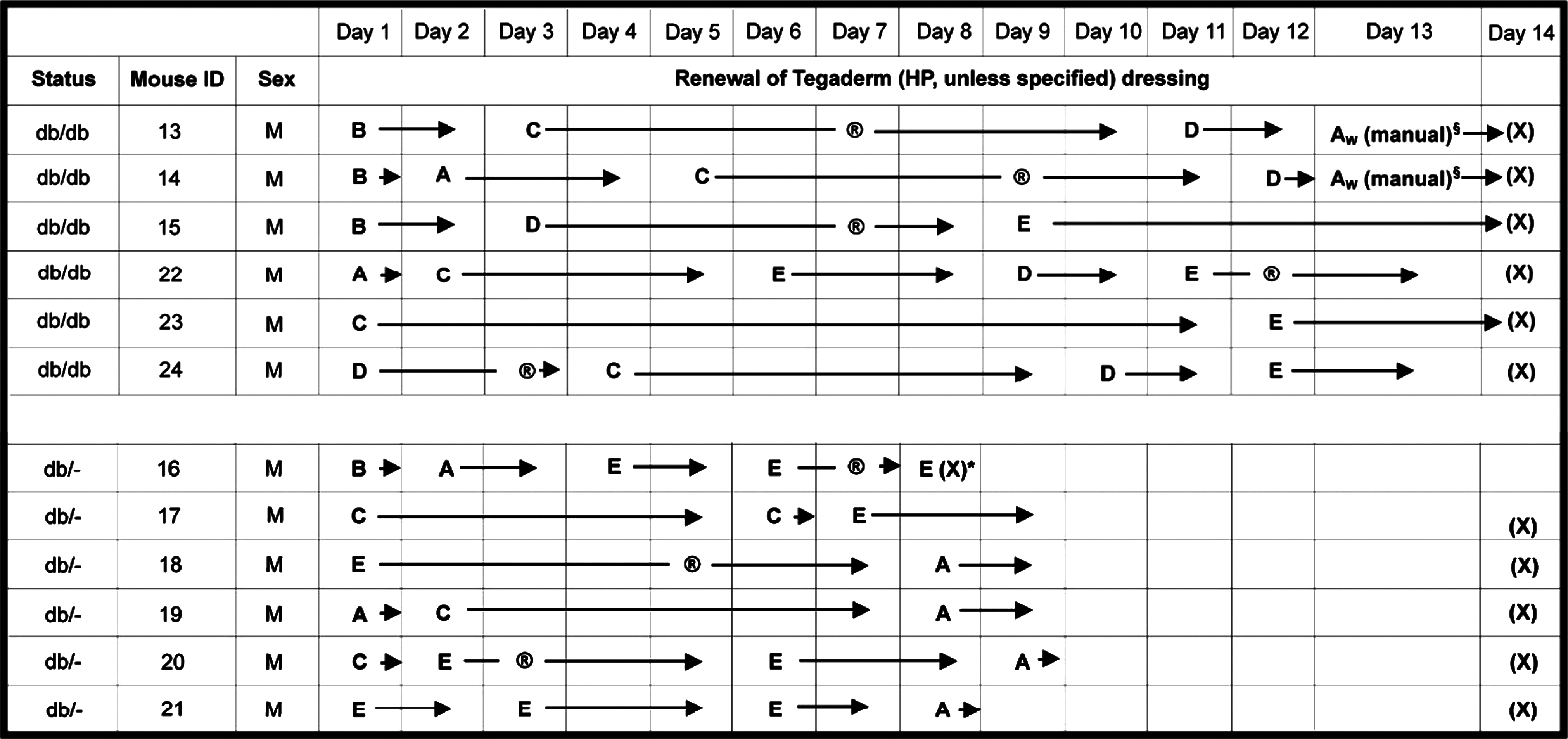
A, B, C, D, and E refer to the five methods used for covering wounds with Tegaderm dressing.
→ indicates the days that the dressings were observed visually to be covering the wounds (e.g., for mouse 13: first dressing covered wound from day 1 to day 2, second dressing from day 3 to day 10, third dressing from day 11 to day 12, and fourth dressing from day 13 to day 14).
® Reattachment of edges of dressing that had become detached by using Mastisol and Fixomull Stretch strips (e.g., for mouse 13 performed on day 7 and mouse 14 on day 9).
* Animal euthanized because of observed “in pain” behaviors.
§ Dressing replacement performed in conscious mice by using gentle restraint.
AWTegaderm W dressing used (method A) instead of Tegaderm HP.
(X), euthanasia.
The number of days that the Tegaderm HP dressing covered the wounds by using the various methods is presented in Table 2. The methods used for the first dressing of diabetic and nondiabetic mice were randomly chosen; as methods A and B did not appear to keep the dressing attached for more than 2 days. Methods using Mastisiol or Fixomull Stretch strips were largely used for subsequent dressings, which were randomly chosen. Inspection of data showed that for diabetic mice, method C kept the dressing attached for the longest time, followed by method E. These two methods were also the most successful for nondiabetic mice.
The values are expressed as mean ± SEM. The numbers of times the method was used are in brackets.
Although method B (which used Cavilon No-Sting Barrier Film alone) was only moderately successful in the pilot study, the use of Cavilon with Fixomull Stretch strips was chosen for first dressing in the optimized procedure, as this adhesive had been used to secure Tegaderm HP dressings in patients for whom it might otherwise have been difficult. Fixomull Stretch strips would help to prevent the dressings from becoming detached at cranial and caudal edges. When the first dressing needed renewing, the skin around the wound was free of any dried Cavilon, which made applying a second dressing with Mastisol very easy. Mastisol was used for all subsequent dressings, by using method C or E, the latter also using Fixomull Stretch strips. Any dried Mastisol remaining on the skin was removed by gentle cleaning with chlorhexidine gluconate (Hibitane). In later studies, dressing renewals were performed by using only method C.
Splinting of wounds
In the pilot and subsequent studies of control (nonirradiated) mice, it was found that Tegaderm HP dressings had covered wounds during whole study period for some of diabetic mice, and wounds had not been exposed to the air and were moist. Measurements on histologic sections of these wounds revealed a very large dermal gap, showing that wound contraction had been retarded by dressing and adhesives. These wounds have been described as being splinted.
Based on measurements of the dermal gap, wounds for both diabetic and nondiabetic mice were divided into two subgroups, splinted and unsplinted. For categorizing wounds in diabetic mice, a threshold dermal gap value was chosen at 2.6 mm and represented 63% of the measured diameter of skin specimens. For nondiabetic mice, a threshold dermal gap value of 2.0 mm was taken and represented 41% of this diameter. A dermal-gap value greater than or equal to the threshold value was indicative of the wound being splinted, whereas a value less than the threshold was indicative of an unsplinted wound. Allocation of wounds to splinted and unsplinted subgroups, together with percentage of wounds splinted, for control mice is shown in Table 3. A much higher rate of splinting occurred in diabetic mice compared with nondiabetic mice, and a significant difference was found in the proportion of wounds splinted to day 10 for diabetic mice compared with nondiabetic mice (2 × 2 test, χ2 = 4.69, p < 0.05).
Wound closure
Photographic images showed that for control diabetic mice on day 14, most of the splinted wounds (n = 11) had a moderate degree of reepithelization and were not closed, whereas all unsplinted wounds (n = 5) were completely reepithelialized and closed (Fig. 2A, B). Wounds in control nondiabetic mice on day 10 showed a similar difference in the extent of closure, with there being a moderate extent of reepithelization in splinted wounds (n = 5) but complete reepithelization in unsplinted wounds (n = 7) (Fig. 2C, D).

Photographs of wounds on the day of euthanasia for diabetic and nondiabetic mice. (
Mean values for wound areas of splinted and unsplinted wounds in control diabetic and nondiabetic mice on days 1, 4, 7, 10, and 14 were presented previously. 11
Measurements of wound outcomes from histologic sections
Consistent measurements were obtained from consecutive wound sections of both diabetic and nondiabetic mice, thereby validating the procedure.
Mean values for DG, EG, DG − EG, and percentage of epithelialization on days 10 and 14 for all control wounds in diabetic and nondiabetic mice were presented previously. 11 The statistical analyses of these findings are now described.
By using ANOVA with Status (diabetic, nondiabetic) and Day of euthanasia as factors to analyze the combined data on days 10 and 14 for all control wounds, the mean values of DG (p < 0.0005), DG − EG (p = 0.004), and histologic score (p = 0.034) were significantly different for diabetic mice compared with those of nondiabetic mice. No significant difference in mean values of EG (p = 0.060), and percentage of epithelialization (p = 0.087) was found between diabetic and nondiabetic mice, although this might be due to the low statistical power of the study; mean values of percentages are usually associated with higher variances compared with absolute values. Diabetic mice had a larger dermal gap, a larger extent of epithelial regeneration, and a lower histologic score than did nondiabetic mice.
By using ANOVA with Status, Day of euthanasia, and Splinting (Yes or No) as factors, significant differences were noted in mean values of DG (p < 0.0005), EG (p = 0.015), DG − EG (p = 0.008), percentage of epithelialization (p =0.005), and histologic score (p < 0.0005) for splinted wounds compared with unsplinted wounds, and no significant interactions between Status and Splinting as factors. The finding for the mean value of DG was expected, because the division into splinted and unsplinted wounds was made by using a chosen value of DG as threshold. Splinted wounds of diabetic and nondiabetic mice had a greater epithelial gap and extent of epithelial regeneration, but lower percentage of epithelialization and histologic score than did unsplinted wounds.
Histology of wounds
The main histologic features of splinted and unsplinted wounds in control (nonirradiated) diabetic and nondiabetic mice have been summarized 11 and are illustrated in Fig. 3.
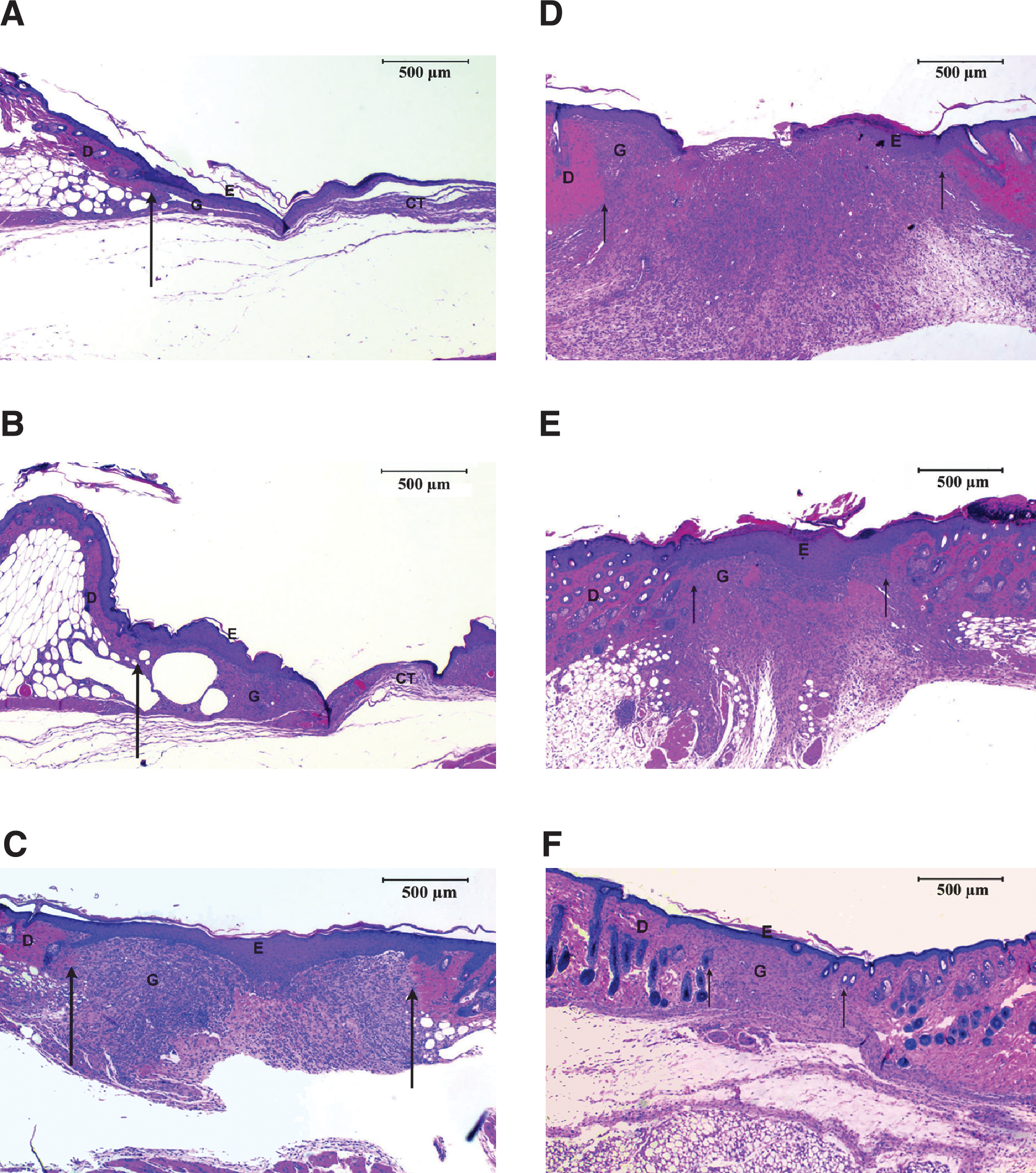
Histologic sections of wounds from diabetic and nondiabetic mice. Diabetic mice: (
Discussion
A recent review of research studies published from January 2003 to August 2008 on laser photobiomodulation of wound healing in mouse and rat revealed that in most studies, the wounds were not reported to be covered with an occlusive dressing. 5 For the few studies in which a transparent adhesive dressing had been used, the dressing remained in place for only a few days. 9 This indicates that covering wounds for extended periods in mice or rats is not easily achieved, and presumably in earlier studies, the dressing often would have become detached, leaving the wound exposed to the air and the healing compromised. Many earlier studies used Tegaderm W or OpSite dressings with or without benzoin compound tincture as the adhesive agent. 6 –10 Covering wounds with a transparent dressing is necessary when performing laser irradiation of wounds by a contact procedure to minimize damage to the wound caused by the tip of the laser probe, to prevent cross contamination if irradiating multiple wounds, and to maximize irradiation.
The present study examined several different methods for covering full-thickness excisional skin wounds in diabetic and nondiabetic mice with a Tegaderm dressing. Tegaderm HP was chosen rather than Tegaderm W, as it is specially manufactured to have greater adhesiveness. Cavilon No-Sting Barrier Film was used as adhesive to attach the first dressing, and Mastisol, for subsequent dressings. Cavilon protects the skin from adhesive stripping, and Mastisol has superior adhesive properties to benzoin compound tincture and has been used successfully with human patients. 13 Daily monitoring of mice to inspect the wounds and dressings was essential to identify those mice in which, although wounds were still covered, a high probability of their becoming uncovered would exist if left until the following day. Dressing renewal for wounds of such mice was therefore performed to prevent this occurring. The combined use of Tegaderm HP dressing and Cavilon and Mastisol adhesive agents was shown to be effective for keeping wounds of diabetic mice covered over 14 days. For all diabetic mice studied, which included laser-irradiated animals, the first dressing remained attached for 3.7 ± 0.3 days, whereas the second and third dressings covered wounds for 4.4 ± 0.3 and 2.5 ± 0.1 days, respectively (mean ± SEM). The latter is underestimated, as some diabetic mice were euthanized on day 10 rather than on day 14. This dressing model in later studies led to a very high proportion (89%) of wounds in diabetic mice showing a retardation of contraction and hence being described as splinted. 11 Although it was much more difficult owing to their smaller size and different body shape, it was possible to splint wounds in some nondiabetic mice. In handling mice for monitoring, photographing, and in subsequent studies, laser irradiation of wounds, care was taken to avoid damaging the dressing or wound.
The diabetic mouse model BKS.Cg-m+/+ Leprdb has the most impaired wound healing among different diabetic mouse models. 14 Splinting of wounds in this model was demonstrated in the present study by measurement of dermal gap in histologic sections, wound dressing records, and appearance of wounds on the day of euthanasia. Although in two previous studies, it was suggested that an adhesive dressing and adhesive agent might splint wounds in diabetic mice, 6,7 no definitive supporting data were presented. The procedure developed in the present study for covering wounds showed that a very high proportion of wounds in diabetic mice are splinted. Data were analyzed by combining all wounds and then identifying two subgroups based on a threshold value for dermal gap to characterize splinted and unsplinted wounds. Statistical analysis showed that the mean value of the dermal gap was significantly greater, and that of histologic score significantly lower, for control (non–laser-irradiated) wounds of diabetic mice compared with nondiabetic mice, indicating that wound healing was impaired in diabetic mice. The extent of epithelial regeneration was significantly greater for diabetic mice compared with nondiabetic mice. These changes might have been caused in part by a larger proportion of the wounds of diabetic mice having been splinted by dressing and adhesive.
Thus, epithelial regeneration is a major contributor to wound healing for diabetic mice compared with nondiabetic mice. A previous study involving measurement of wound areas showed that wound closure was delayed for diabetic mice compared with nondiabetic mice. 11
Splinted wounds had a significantly higher mean value for epithelial gap and extent of epithelial regeneration and significantly lower mean values for percentage of epithelialization and histologic score than did unsplinted wounds. The latter, together with higher mean value for the dermal gap, is consistent with splinting causing a delay in wound healing in both diabetic and nondiabetic control mice, and epithelial regeneration being a major contributor to the healing of splinted wounds. The delay in healing of splinted wounds was also demonstrated by histologic appearance of the wounds.
Mice are loose-skinned animals, so their skin elasticity and its lack of strong adherence to the underlying structures allows contraction to play a significant role in wound closure. 15 In this study, wound contraction had been retarded in splinted wounds. Healing of splinted wounds of diabetic mice by epithelial regeneration and granulation tissue formation closely mimics wound healing in human patients with type 2 diabetes. 16 This dressing model has the potential to allow testing of therapies that promote epithelial regeneration or granulation tissue formation or both (e.g., low-level laser therapy and topical application of growth factors). Tegaderm dressing is highly suited for laser irradiation and is reported to have a transmission of laser light of 93% and 94% at 532 and 1,064 nm, respectively. 17 A later reported transmission of 74% at 720–800 nm 18 could be due to a change in characteristics of laser light on passing through the dressing and also possible scattering of light with an increase in beam diameter.
The model also has implications regarding treatments for diabetes-related cutaneous pathologies in diabetic human subjects. Other approaches to splinting wounds in mice and rats have involved the use of silicone or metal rings attached to the skin with adhesives or sutures or both. 14,19 –22 However, no measurements of a dermal gap were reported in the mouse studies. 14,22 The dressing model described in the present study has the advantage that wounds can be splinted without recourse to invasive treatments such as suturing the skin, which would lead to inflammation at suture sites and influence healing through the release of mediators (e.g., interleukin-1β). 23,24
Conclusions
The wound-dressing procedure using Tegaderm HP and newer adhesives was simple, easy to perform, and had a very high rate of wound splinting (>80% for later studies) in diabetic mice. The model developed does not have the deficiencies identified in previously reported studies and testing of therapies to stimulate cutaneous wound healing (e.g., laser irradiation) can be performed in this model, which mimics human wound healing. This study using control diabetic and nondiabetic mice provided valuable reference data with which laser-irradiation studies can be compared.
Footnotes
Acknowledgments
The technical assistance of Ms M. Fisher and Ms D. Potter, Histology Unit, University of Otago, is gratefully acknowledged. We thank Professor P. Herbison, Department of Preventive and Social Medicine, University of Otago, for statistical advice. We are grateful to Dr. J. Schofield, Director of Animal Welfare, University of Otago, for advice on creating the wounds surgically and on the care of mice. We thank R. McPhee, Department of Anatomy and Structural Biology, University of Otago, for producing the illustrations.
Author Disclosure Statement
Competing financial interests do not exist.