
Abstract
Introduction
Muscle repair is a complex process involving different phases, including inflammation, cell proliferation, and the synthesis of elements that constitute the extracellular matrix (ECM), such as collagen, and elastic and reticular fibers. 5 However, this healing process is often inefficient and results in the formation of scar tissue, which can contribute to the likelihood that muscle injury will recur. 4
The ECM and the molecules of the basal lamina are now known to be critical for skeletal muscle stability, regeneration, and muscle cell–matrix adhesion. 6 Collagen is an abundant component of the ECM and is important to muscle function, especially with regard to the lateral transmission of force, which is important in decreasing injury induced by contraction. 7 –9 Collagen synthesis is stimulated as soon as the interstitial lesion begins and is extended through to the final healing phases, as the remodeling of the tissue occurs. 5 Therefore, changes in the composition of the ECM could lead to changes in the ability of muscles to transmit force and to limit contraction-mediated muscle damage. 10
Several collagen types are found in skeletal muscle connective tissue, but collagen IV is the main component of basement membranes and forms a microfibrillar network in close association with the basement membrane around muscle cells, which interacts with other ECM components. Collagen IV is thought to play a critical role in the cell arrangement in tissue (e.g., by ensuring mechanical stability in skeletal muscle fibers). 6,9,11
Low-level laser therapy (LLLT) was introduced in the 1970s and 1980s, and since then, considerable scientific research has been undertaken to evaluate its potentially beneficial effects, including the use of cell cultures, animal models, and clinical studies. 1,12 This resource is an important form of therapy that has been used to treat muscle pain, but the biologic mechanisms behind the beneficial results achieved in clinical trials remain unclear. LLLT has been found to accelerate wound healing as well as to reduce pain and inflammatory response, thereby exhibiting several beneficial effects on inflammation and healing. 13,14 In muscle and tendon injuries, LLLT has been shown to reduce the duration of acute inflammation and accelerate tissue repair. 1
A number of studies have demonstrated the potential of LLLT in facilitating the muscle-healing process. 3,13,14 Other studies have demonstrated the enhancing effects of LLLT on fibroblastic activity and collagen production, but no consensus was reached about the findings. Pugliese et al. 5 verified that the Ga-Al-As laser induced a biomodulation of the collagen and elastic fibers, evidenced through an increase in the deposit of these fibrillar elements in the animals given laser therapy, and the 4-J/cm2 energy density provided more-significant results than the 8-J/cm2 one. In addition, Yasuhiro et al. 15 showed that LLLT with a wavelength of 632.8 nm induced an increase in procollagen synthesis in human fibroblast culture. Therefore, these findings suggest that this therapeutic modality can interact in an efficient manner with the various extracellular matrix elements. A close association has been demonstrated between increased collagen synthesis and the regenerative processes that occur in human skeletal muscle after exercise-induced muscle damage. 16 However, little is known regarding its effects on ECM remodeling (especially that of collagen IV) after cryolesion. No consensus exists in the literature regarding the best laser-irradiation parameters or the type of laser used for accelerating muscle repair. 17 In addition, little is known regarding the effects of the regenerative processes on ECM remodeling (especially that of collagen IV) by using a cryolesion muscle-regeneration model. Thus, the aim of the present study was to determine the effect of GaAlAs LLLT on collagen IV remodeling of the tibialis anterior (TA) muscle in rats after cryolesion.
Methods
The experimental protocols used in this study were in compliance with the principles of laboratory animal care formulated by the Brazilian College of Animal Experimentation (COBEA) and received approval from the Ethics Committee of the Universidade Nove de Julho São Paulo-SP, Brazil (protocol number: 13/2007).
Adult male Wistar rats (n = 45), weighing 234 ± 37.99 g at the beginning of the procedure, were maintained under controlled conditions of room temperature (22°C), relative humidity (40%), and 12-h night/day cycle, and were fed before and during the experimental period with solid rations and water ad libitum.
The animals were randomly divided into three groups: control (n = 5) without injury; nontreated cryolesioned group (n = 20), and LLLT-cryolesioned group (n = 20). The control group was killed 1day after the beginning of the experiment. The cryolesioned groups, with or without LLLT, were analyzed at 1, 7, 14, and 21 days after the injury procedure.
Surgical procedures were performed based on those described by Miyabara et al. 18 with the administration of 1 mL/kg of 1% ketamine HCL (Dopalen; Vetbrands, Sao Paulo, Brazil) and 2% xylazine (Anasedan; Vetbrands, Sao Paulo, Brazil). The TA muscle was surgically exposed and submitted to the cryolesion procedure, which consisted of the application of a round metal probe (3 mm in diameter) that had been cooled with liquid nitrogen to the surface of the exposed TA and maintaining it in this position for 10 sec. After the frozen muscle had thawed, the procedure was repeated on the same area for additional 10 sec.
The cryoinjured area was macroscopically identified as a firm, white, disk-shaped region. In all cryolesion groups, only the left TA muscle was injured, and the right side served as the control. The wounds were closed with polyamide sutures, and the animals were kept for several hours on a warm plate (37°C) until they recovered from the effects of the anesthetic, to prevent hypothermia.
Laser irradiation
The laser device used in this study was the GaAlAs diode laser (MMOptics Ltd., São Carlos, SP, Brazil) with a beam spot of 0.04 cm2, an output power of 20 mW, wavelength of 660 nm, energy density of 5 J/cm2, and a power density of 500 mW/cm2, applied for 10 sec. The laser beam was placed in contact with the skin surface corresponding to the cryolesion area, and the irradiation was applied at eight points delimited in the cryolesion area (Fig. 1). Therefore, the energy was 0.2 J per point, totaling 1.6 J per treatment. The LaserCheck power meter (Coherent, Santa Clara, CA) determined the output of the equipment. The experiments were set up to standardize the procedures. Laser irradiation was performed on the TA muscle by using the AsAlGa laser on the injured region. This treatment was initiated 24 h after the lesion and performed 3 times per week, with a 24-h interval between sessions, totaling three sessions for the muscles analyzed at 7 days, six sessions for the muscles analyzed at 14 days, and 10 sessions for the muscles analyzed at 21 days.

TA laser-irradiation procedure. Circles represent areas around the injured region that received point laser treatment.
Animal killing was performed with an overdose of ketamine and xylazine. The left and right TA muscles were removed, weighed, and immediately frozen in liquid nitrogen–cooled isopentane and stored in liquid nitrogen. The 10-μm cross-sections were obtained from the frozen muscles with a cryostat (Leica CM3050, Nussloch, Germany), mounted on slides, and then stained with hematoxylin–eosin to visualize the general morphology of the muscle by using a microscope (Axioplan 2 Zeiss, Oberkochen, Germany).
Immunohistochemical analysis
Frozen sections were mounted on slides, air dried, and fixed in 20% acetone for 20 min. Slides were incubated for 15 min in 50% methanol solution, washed in distilled water, followed by 10 min in PBS buffer, and then incubated for 10 min in 2% bovine serum albumin (BSA)/PBS solution to block nonspecific binding. Sections were incubated for 1 h at 4°C with collagen IV antibody (Dako, Carpinteria, CA; anti-mouse, catalog MO785) with a 1/100 dilution in 0.1% BSA/PBS.
After incubation with the primary antibody, the sections were thoroughly washed with PBS buffer for 10 min and exposed to the secondary antibodies (1:100) (LSAB plus System HRP; Dako, Carpinteria, CA) for 30 min and, after further washing, incubated with streptavidin–biotin complex for 30 min. The sections were then incubated with diaminobenzidine tetra-hydrochloride (DAB; Novocastra, Newcastle, UK) and counterstained with Mayer's hematoxylin. Negative controls consisted of replacing the primary antibody with nonimmune serum.
Results
Morphologic aspects
Unlesioned control muscles exhibited normal muscle morphology with the presence of polygonal fibers containing peripheral nuclei and no signs of lesions. The findings of the nontreated and LLLT cryolesioned groups revealed similar morphologic aspects throughout the skeletal muscle repair process (Fig. 2). One day after injury, the skeletal muscle exhibited neutrophil infiltration with edema and necrotic fibers (Fig. 2a and b). At 7 days, the tissue exhibited a reduction in the inflammatory infiltrate and the appearance of immature skeletal muscle cells (Fig. 2c and d). At 14 days, a decrease in inflammatory infiltrate was noted, and fibers exhibited an increase in diameter, but the majority of fibers had a centrally located nucleus (Fig. 2e and f). At 21 days, most cells had a mature appearance (Fig. 2g and h).

Morphologic findings of nontreated and LLLT groups. At 1 day after injury, skeletal muscles that received treatment (
Immunohistochemical analysis
In control groups, collagen IV appeared as a tenuous line enveloping muscle fibers (i.e., endomysium), with a stronger signal evident in the perimysium (Fig. 3a and b). The nontreated and LLLT groups exhibited more-intense collagen IV immunostaining than did the contralateral controls in all experimental periods.
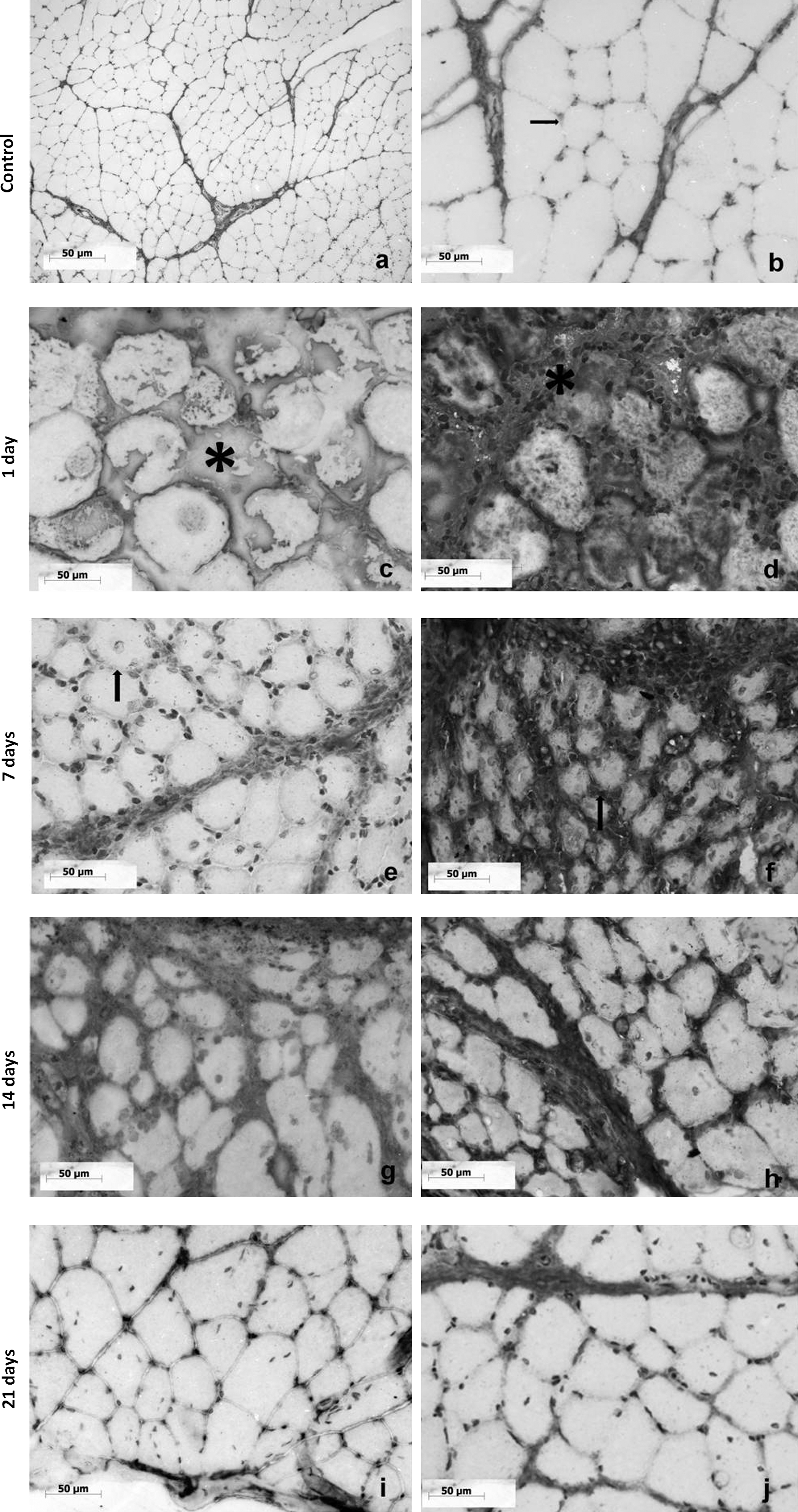
Immunohistochemical analysis of collagen IV in rat skeletal muscle. In the control group, collagen IV appeared as a tenuous line involving muscle fibers (endomysium; arrow) and more-abundant immunoassaying in the perimysium [
At 1 day after injury, collagen IV distribution was similar in nontreated and LLLT groups, with dispersed immunolabeling in the cellular space of the necrotic fibers (Fig. 3c and d). After 7 days, the LLLT-treated group demonstrated an increase in collagen IV immunolabeling and distribution when compared with the respective nontreated group (Fig. 3e and f). This change was most evident in the ECM of the endomysium. A stronger collagen IV immunolabeling with better-organized and compactly arranged collagen fibers was observed. At 14 days, an increase in collagen IV immunolabeling was seen in the endomysium in the nontreated group (Fig. 3g), which was similar to that of the LLLT group (Fig. 3h). At 21 days, both nontreated and LLLT groups exhibited similar collagen IV distribution to that observed in the control group (Fig. 3i and j).
Discussion
The results of the present study demonstrate that LLLT promotes an increase in collagen IV immunolabeling in skeletal muscle in the first 7 days after acute trauma caused by cryoinjury, but does not modify the duration of the tissue-repair process. Even with LLLT, the injured muscle tissue needs ∼21 days to achieve the same state of organization as noninjured muscle.
Laser phototherapy is based on photochemical and photobiologic effects on cells and tissues. LLLT has been used mostly on pathologic tissues exhibiting some degree of alteration, such as healing or inflammatory processes. According to the literature, LLLT accelerates wound healing by increasing mitotic activity and promoting changes in collagen synthesis. However, the mechanisms of this effect have not yet been fully identified. 14,19
In the present study, the cryolesion model used was effective in inducing injury and subsequent regeneration in a well-delimited area of the TA muscle, as described previously by Miyabara et al. 18 However, no changes in cell morphology or the duration of muscle healing occurred with laser treatment over a 21-day period. LLLT is known to depend on a combination of parameters such as wavelength, power, energy, density, irradiated area, exposure time, and number of irradiations. 19 –21 Further studies are needed to determine the best laser-irradiation parameters for achieving improvement in skeletal muscle cell growth.
Conversely, the laser protocol used in the present study affected collagen IV labeling in the muscle cells, especially at 7 days after cryoinjury. The laser-treated group exhibited collagen IV distribution at 7 days after injury, similar to that achieved in the nontreated animals at 14 days. This type of collagen is the main component of the basal membrane and is responsible for the maturation, strength, and maintenance of mechanical stability in skeletal muscle fibers. It therefore plays an important role in muscle healing. 6,11 The tolerance of the basal cell membrane to stress in cases of injury is dependent on the integrity of this protein. Based on these aspects, the results of the present study indicate that laser therapy may help the mechanical stability of skeletal muscle in the first days after injury, but does not affect the duration of fiber maturation. Once again, collagen IV labeling of treated and nontreated muscles was different only at 7 days after injury. On days 14 and 21, the collagen immunolabeling was similar between groups.
The effects of LLLT on collagen and procollagen synthesis have been demonstrated in the literature. 19,21 However, controversy regarding the effect of laser irradiation on collagen metabolism remains. Some authors have suggested that laser light increases collagen synthesis, 22,23 whereas other authors report a decrease in collagen synthesis after irradiation. 21,24
A study was carried out by using standard transverse contusion injury inflicted to the left calf of rats, and the effects of immobilization and mobilization on the production of granulation tissue and scar formation were observed. Types IV and V collagen were detected in the endomysium around the regenerated and uninjured muscle fibers, and small regenerating muscle fibers were seen within the sear tissue in all groups. 25
Furthermore, a number of studies have demonstrated modifications in collagen proteins after different exercise protocols. Immunohistochemical changes in collagen III and IV have been found in the endomysium, and an increase has been observed at 5–20 days after exercise. An increase in collagen I and III RNAm has been reported in skeletal muscle after running. 26 An increase in collagen IV has been described in rat skeletal muscle after long-term exercise 27 as well as brief exercise. 8,28 –31 Furthermore, Mackey et al. 12 found an increase in type IV collagen-staining intensity in human muscle endomysium after a round of high-force eccentric muscle contractions, thereby suggesting extracellular matrix remodeling.
Medrado et al. 14 applied LLLT with different energy densities to rats with dorsal skin wounds and analyzed the lesions after 5, 7, and 14 days with histology, immunohistochemistry, and electron microscopy. The authors found that the extent of edema and the number of inflammatory cells were reduced in the treated animals at all evaluation times, and an increase in the proliferation of fibroblasts and myofibroblasts coincided with an augmentation of collagen and elastic fibers. Moreover, LLLT on other tissues was proven to play an important role in collagen remodeling. In the present study, an increase in collagen IV labeling and better distribution in the laser-treated group was noted, particularly on Day 7. A number of studies have found laser therapy to be capable of influencing the proliferation of fibroblasts, osteoblasts, and epithelial cells. This therapy may also modulate the muscle-regeneration process as well as collagen IV distribution and organization, which may provide benefits to muscle tissue during the repair process.
In summary, the results of the present study show that collagen content is modulated in regenerating skeletal muscle under LLLT, which might be associated with better tissue outcome, although the histologic analysis did not detect tissue improvement in the LLLT group. This is a preliminary study, and further studies must clarify how LLLT could induce changes in other ECM components, such as type I and type III collagen, fibronectin, and laminin. Additional experimental techniques are planned for analyzing collagen IV expression during this process.
Footnotes
Acknowledgments
We thank CNPq and UNINOVE for financial support.
Author Disclosure Statement
No competing financial interests exist.