
Abstract
Introduction
In humans, the liver can overcome a direct traumatic injury caused by car accident, blast injury, etc., or during surgical procedures that are performed in order to remove cancerous tissue. In such situations, the kinetics of liver regeneration following the trauma are highly significant to the patient due to the vital importance of the liver. Bone-marrow-derived mesenchymal stem cells (MSCs) are known to support hematopoiesis naturally by secreting a number of trophic molecules and growth factors. 3 The potential role of stem cells in liver regeneration has been recently reviewed, 4 and studies have shown that systemic administration of MSC-derived molecules significantly improved short-term survival in a rat model of fulminant hepatic failure. 5 The same molecules showed in vitro a direct inhibitory effect on hepatocyte death and a stimulatory effect on their proliferation. 6
The biostimulatory effects of low-level laser therapy (LLLT) on cells and organs have been extensively studied and reviewed. 7 –9 The beneficial effect of LLLT following ischemic or mechanical injury to organs like the skeletal muscle, heart, and brain has also been reported. 9 –11 However, the effect of LLLT on the process of liver regeneration has not been extensively studied. Gershbein et al. 12 found that at 10 d post hepatectomy, there was no effect of Argon and Nd:Yag lasers on liver regeneration compared with control non-laser-treated hepatectomized livers. de Castro et al. 13 have shown that application of LLLT following 70% hepatectomy to rats caused a dramatic increase in respiratory mitochondrial activity in the injured liver as early as 24 h post hepatectomy. The aim of the present study was to determine whether LLLT can enhance cell proliferation and blood-vessel formation during the critical early phase (up to 48 h) post acute hepatectomy.
Materials and Methods
Experimental procedure
Twelve 2-mo-old Charles River male rats, average weight 250 g, were used for this experiment. The rats underwent anesthesia with Avertin (1 mL of 2:1W/W Tribromoethanol-amine in Tert-Amyl-Alcohol diluted 1:40 in saline) 1 ml/100 g bw. The abdomen was exposed and ca. 70% of the liver was excised. The operation was performed under semi-sterile conditions with surgical instruments that were autoclaved prior to use. The excised tissue was weighed in order to assess that 30% remained. The abdominal incision was sutured, and rats were fed and supplied with water.
Laser irradiation
Rats were randomly assigned to control or laser-irradiated groups upon completion of the surgical procedure. A diode (GaAlAs) laser, wavelength 810 nm, with a tunable power output of maximum of 400 mW was used (Lasotronic Inc., Zug, Switzerland). The laser device was equipped with a metal-backed glass fiber optic (1.5-mm diameter). The beam diameter of the laser was 2 cm, and the measured power of irradiation on the liver was 5 mW/cm2. An infrared viewer (Lasotronic Inc.) and infrared-sensitive detecting card (Newport Inc., Irvine, CA) were used to determine the infrared irradiation area. A Nova laser meter equipped with special detecting probe (Ophir Optronics, Ltd., Jerusalem, Israel) was used to measure the power (in mW) of the laser irradiation applied to the liver. The laser was applied 3 h post surgery by placing the distal tip of the fiber optic on the shaved skin above the injured area, and the laser was set to deliver a power output that would yield a power density of 5 mW/cm2 on the liver. The duration of irradiation was 60 s, delivering a total energy of 0.6 J/cm2. At this power density (5 mW/cm2) of the laser, there was no elevation of temperature in the abdomen, as recorded from a thermocouple placed under the irradiated area. Control non-irradiated rats underwent the same procedure, but the laser was not turned on.
BrdU labeling and immunohistochemistry
For determination of newly formed blood vessels, 5-Bromo-2′deoxyuridine (BrdU, Sigma Co., St. Louis, MD) was injected intraperitoneally into the liver in order to label proliferating cells. At 3 h post operation, the rats were injected with 10 mg/100 g bw BrdU. The BrdU injection was repeated the following day at 5 h prior to sacrifice. The rats were sacrificed by an overdose of Avertin at 2 d post hepatectomy. The entire liver was excised and placed in neutral buffered formalin (NBF) for fixation. After customary procedures of embedding and sectioning, the slides were subjected to immunohistochemical assays for BrdU (Zymed Laboratories Inc. San Francisco, CA) for estimation of proliferation, and c-kit (Santa Cruz Biotechnology, Santa Cruz, CA) as the marker of MSCs, according to the manufacturer's instructions. Histological sections from each liver were randomly selected for analysis of new blood-vessel formation, using BrdU staining kit according to the manufacturer's instructions (Zymed Laboratory Inc. Streptavidin-Biotin system). The sections were viewed at a direct 400 × magnification using a Zeiss microscope equipped with a video screen. Three observers, who were blinded to control or laser-treated rats, analyzed the blood vessels in the entire area of the liver sections. The total number of newly formed blood vessels (less than 50 μm in diameter) and total number of blood vessels were counted in each area. Newly formed blood vessels were defined as those that had one or more BrdU labeled endothelial cells nuclei. The number of blood vessels was expressed relative to the analyzed area. BrdU labeled cells were also counted as a parameter for newly formed proliferating hepatic cells.
Statistics
The Sigma statistical software (Sigma, St. Louis, MO) was used for statistical analysis. Tests were performed first for normality distribution followed by parametric (ANOVA) or non-parametric test. Statistical significance was defined when p values were <0.05.
Results
Figs. 1 and 2 demonstrate that the density of proliferating (BrdU immunopositive) cells in the regenerating area of the laser-treated liver was significantly (p < 0.01) higher (2.6-fold) than in the control non-laser-treated livers. Similarly, the density of newly formed blood vessels was also significantly (p < 0.01) elevated (3.3-fold) in the laser-treated livers relative to the non-laser-treated ones (Figs. 3 and 4). The density of the c-kit immunopositive cells was 2.3-fold higher (significantly, p < 0.01) in the livers that were subjected to laser application in comparison to the non-laser-treated rats (Fig. 5).
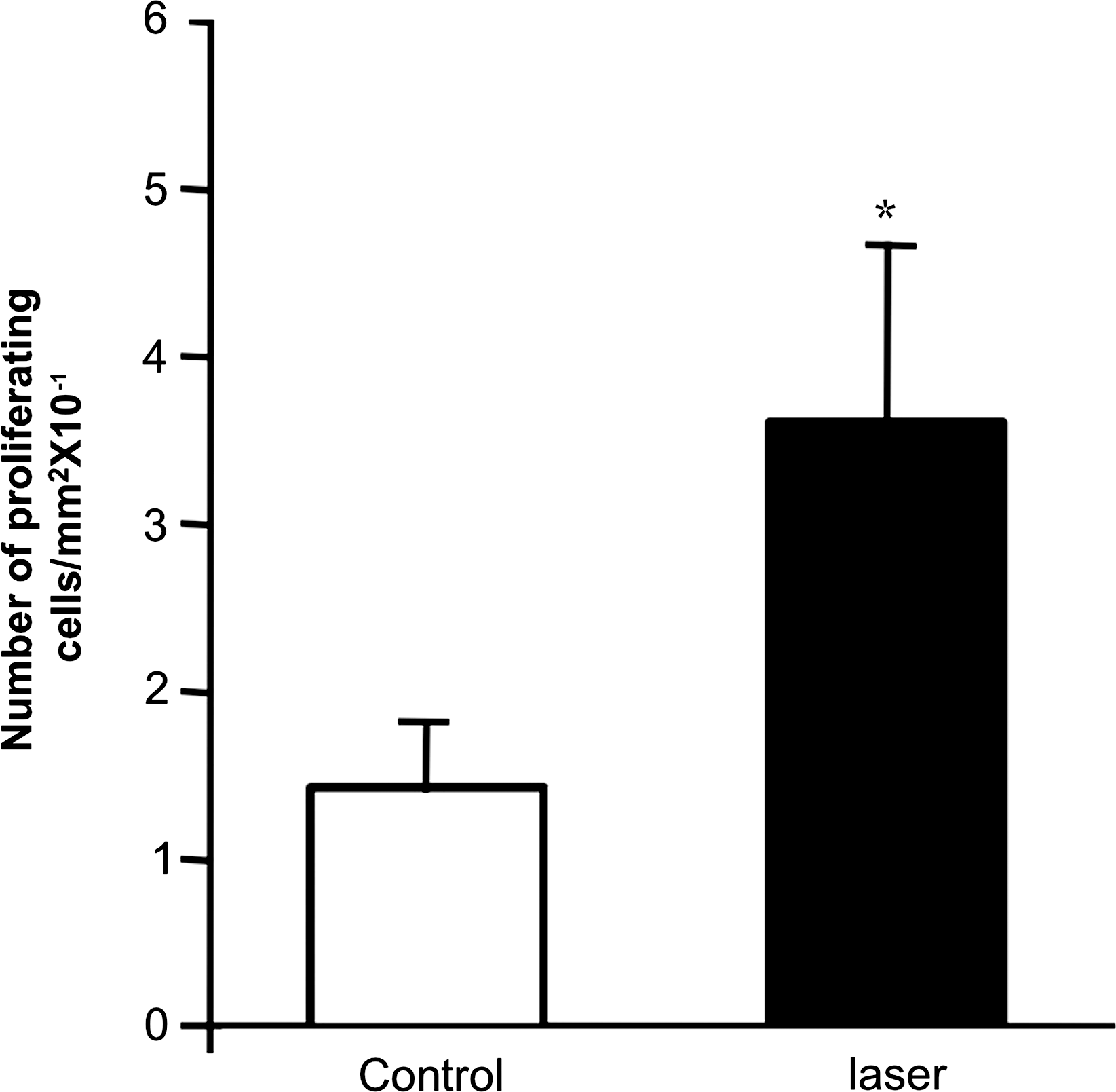
Density of BrdU immunopositive cells in control non-laser-treated (open column) and laser-treated (solid column) regenerated area in liver of rats 2 d post heapatectomy. Results are expressed as mean ± SEM of rats in each group.

Representative light micrographs of histological sections from the regenerated zone of BrdU immunopositive staining of control (a) and laser-treated (b) livers. Note a higher density of immunopositve nuclei in the laser-treated livers as compared to non-laser-treated ones. (Color image can be found at
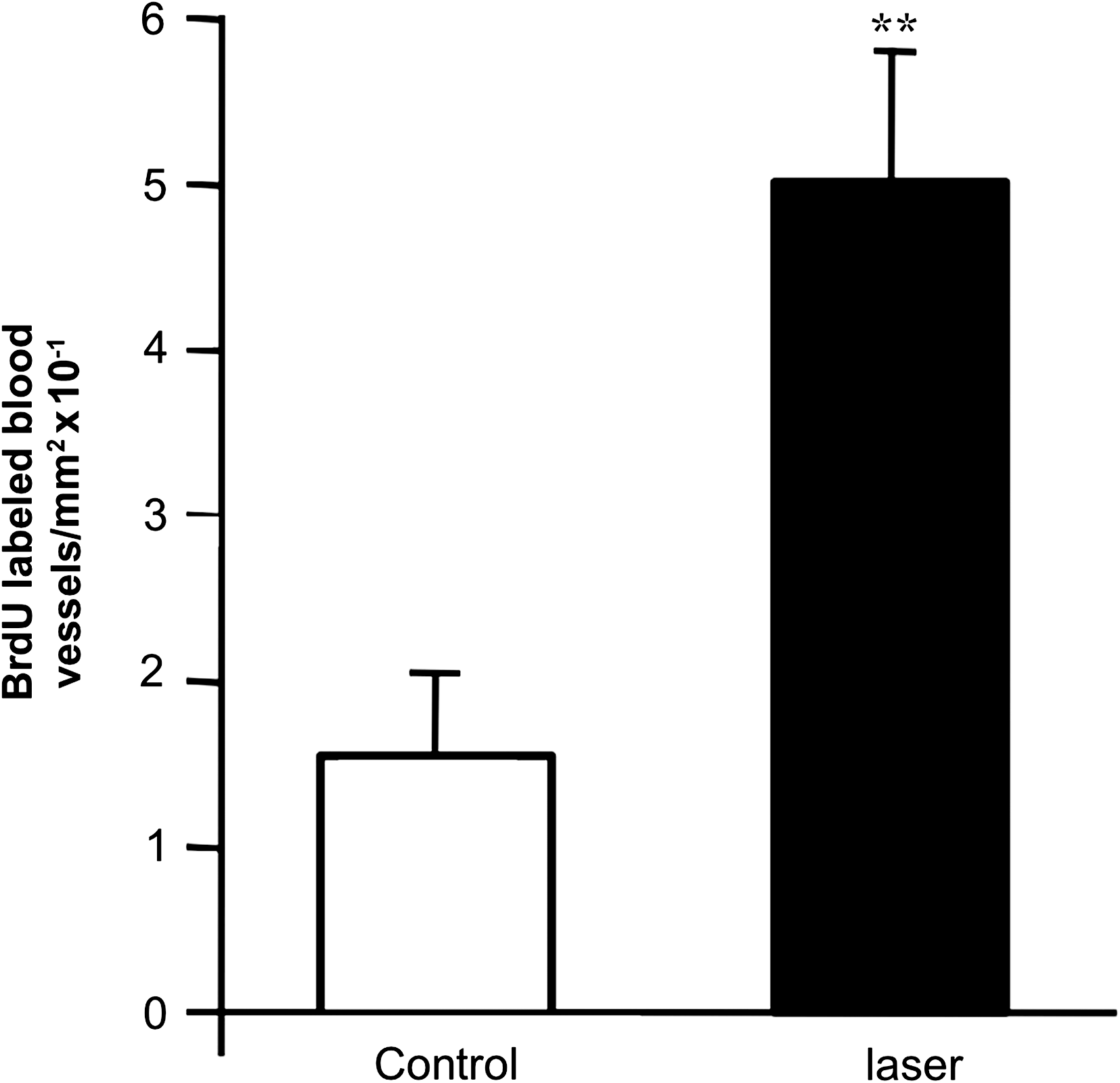
Density of newly formed blood vessels in control non-laser-treated (open column) as compared to laser-treated (solid column) regenerated area in liver of rats 2 d post hepatectomy. Results are expressed as mean ± SEM of rats in each group.
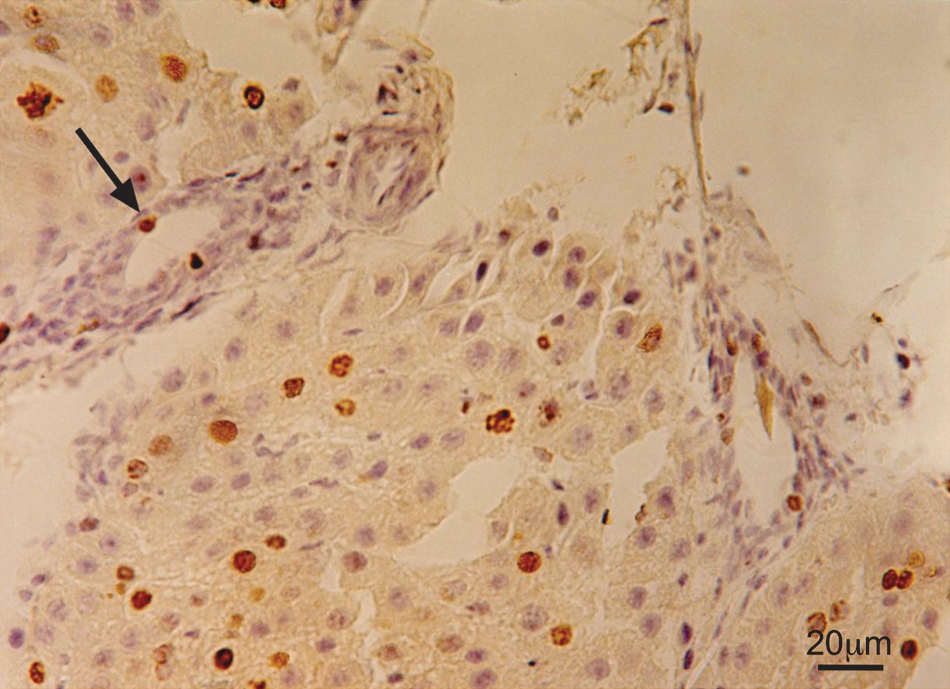
Representative light micrographs of BrdU immunopositive staining in endothelial cells of new blood vessels (arrow) in laser-treated hepatectomized rat livers. (Color image can be found at

Density of c-kit immunopositive cells in control non-laser-treated (open column) and laser-treated (solid column) rats 2 d post hepatectomy. Results are mean ± SEM of rats in each group.
Discussion
The results of the present study demonstrate that LLLT significantly affects the initial phase of regeneration post hepatectomy. This effect is associated with promoting the proliferation of newly formed hepatocytes enhancing formation of new blood vessels and a higher density of c-kit immunopositive cells in the regenerated region of the injured liver in the laser-treated livers versus control, as early as 2 d post hepatectomy. The enhanced cell proliferation and new blood-vessel formation in the partially hepatectomized laser-treated livers as early as 48 h post injury, most probably augmented to the process of liver regeneration. Enhancement of cell proliferation by LLLT has been previously reported for various types of cells, including cardiac stem cells and MSCs in vitro. 13 –16 Enhanced proliferation of cells following LLLT to the subventricular (regenerating) zone in the brain of stroked rats has also been reported. 11 Promotion of neoformation of blood vessels (angiogenesis) by LLLT was also demonstrated in the rat heart post myocardial infarction. 17 The enhanced formation of new blood vessels as early as up to 48 h post hepatectomy contributed to the enhanced regeneration of the liver, as found also for other regeneration process in injured/ischemic organs. It has been recently postulated that MSCs can contribute to the regeneration of organs not only by their differentiation to the type of the injured cells, but also by secreting various growth factors at the site of injury. 3 The enhanced cell proliferation and blood-vessel formation may thus be a result of enhanced secretion of growth factors from the cells that are c-kit immunopositive, whose density was found to be elevated in the laser-treated livers.
The present study may also have clinical relevance. The kinetics of liver regeneration, which has a spontaneous regenerative capacity, after partial hepatectomy (due to direct trauma such as car accident, sport injury, blast etc.) may be a crucial factor for the survival of trauma victims. The use of LLLT offers a new approach to patients' post hepatic trauma, facilitating a speedier recovery and possibly increasing the survival rate of victims following acute liver injury. LLLT can also be used to treat patients with liver cancer who undergo partial hepatectomy (post or during chemotherapy) as the kinetics of liver regeneration post surgery is limited as a result of the chemotherapy, which is aimed at inhibiting cell proliferation. Thus, in these patients, it is crucial to restore the liver function post such surgery.
Conclusion
The fact that the liver has a natural capacity to regenerate can serve as a basis for accelerated regeneration due to LLLT applied close to the event of hepatectomy. LLLT given 3 h post hepatectomy significantly enhanced the formation of blood vessels, hepatocyte proliferation, and mesenchymal stem-cell density in the newly formed liver tissue in comparison to control non-laser-treated rats as early as 2 d after hepatectomy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.