
Abstract
Introduction
Another possibly effective approach to treatment of xerostomia is offered through the application of the low-level laser therapy (LLLT). Generally, LLLT uses light energy in the form of photons to produce cellular responses in the cell. 7 Light photons are absorbed by cytochromes and porphyrins in the mitochondria of the cell. 8,9 Three things are proposed to occur: (a) a temporary release of nitric oxide from its binding site on cytochrome-c oxidase, which results in an increase in cell respiration and transcription 10,11 ; (b) stimulation of ATP (adenosine triphosphate) synthesis by activation of the electron transport chain 12,13 ; and (c) transient stimulation of reactive oxygen species, which play a significant role in cell activation. 14 These are thought to activate numerous intracellular pathways; regulate nucleic acid synthesis and protein synthesis; modulate levels of cytokines, growth factors, and inflammatory mediators; and stimulate proliferation and differentiation of different cell types. Previous studies on experimental animal models demonstrate the diverse effects of LLLT on salivary glands. It was shown that LLLT stimulates mitotic activity in the epithelial tissue of murine salivary glands, 15,16 increases the salivary flow rate, 17 changes enzymatic activity levels in saliva by decreasing peroxidase and catalase activity, 17 –19 and alters salivary protein concentration. 20,21 Most of the previously published studies refer to investigations into the effect of low-power lasers on structural and cytochemical alterations in animal salivary glands, while only a small number of clinical cases have been reported.
Given the increasing population of elderly persons, it is expected that xerostomia will be present in a large number of patients in the coming years and therefore treatment options need to be evaluated. So far, limitations in application of LLLT are the availability of laser devices, found almost exclusively at hospital facilities or clinics, and lack of consensus about the most effective laser and treatment parameters for best results. Since only a scarce number of in vivo clinical trials have been conducted to evaluate the effect of LLLT on salivary glands, the purpose of our study was to investigate the effect of LLLT on salivary flow rates in patients with xerostomia (dry mouth).
Materials and Methods
In this study the pulsed semiconductor Ga-As laser (Tecno Gaz) operating at 904 nm was used to treat 34 patients with xerostomia (age range, 43–74 y; mean age, 56 y) referred to our Department of Oral Medicine. An additional 16 patients, matched in age (age range, 48–70 y; mean age, 54 y), served as a control group and were treated with 15 mL of a 2% citric acid solution applied as a mouth rinse for 30 sec. The inclusion criteria for all patients were medical histories free of radiotherapy, Sjögren's syndrome and xerostomic drugs (antiretroviral medications, antihistamines, anticholinergics, antihypertensives, decongestants, narcotic analgesics, tricyclic antidepressants). 22 Sjögren's syndrome was excluded by the applied diagnostic criteria. 23 The study was performed according to the principles of the Helsinki declaration 24 and all subjects gave their informed consent in written form.
The selection of laser wavelength generally depends on targeted application and is governed by the fact that the optical characteristics of tissues vary considerably and are characterized by scattering and absorption coefficients that in turn depend on wavelength. 25,26 For example, the principal skin tissue chromophores (hemoglobin and melanin) have high absorption bands at wavelengths shorter than 600 nm. For this reason the visible or UV light does not penetrate to the tissue below the skin. On the other hand, water begins to absorb significantly at wavelengths greater than 1150 nm. Therefore, there is a so-called “optical window” in tissue covering the red and near-infrared wavelengths, in which the effective tissue penetration of light is maximized. In that context, Ga-As lasers operating at 904 nm provide the “effective penetration depth,” defined as the depth of penetration into a tissue at which the laser light intensity is so low that no biological effect of the light can be detected. 27 For example, the effective penetration depth for 7 mW HeNe laser (632 nm) is about 8–10 mm, while that for the corresponding Ga-As laser is 20–30 mm, thus providing deeper penetration into the tissue. 28,29 Aside from these considerations, further investigations of spectral dependence of response to laser therapy are outside the scope of the present study.
The laser beam was applied bilaterally in noncontact mode to each salivary gland area, extraorally to the parotid and submandibular glands and intraorally to the sublingual gland (each patient received a total of six exposures, each lasting 120 sec, within 10 consecutive days of treatment). The distance between the probe and the irradiated area was kept constant at 0.5 cm throughout the treatment period. The mean energy density was 29.48 J/cm2 per exposure. The relevant technical data for the laser are given in Table 1.
FWHM, full width at half maximum.
For both groups the quantity of whole resting and stimulated saliva (Q-sal, mL/min) was measured for each patient before the laser treatment (LT) and 5 min after treatment and in controls before the citric acid stimulation and 5 min after the stimulation. Patients were asked to expectorate all saliva into graduated test tubes for a 10-min period. The amount of saliva was determined by the scale on the graduated tubes. Statistical methods, including correlation analysis and t-testing of the hypothesis were used for comparison and interpretation of the difference in salivary flow rates between the two groups.
Results
The salivary flow rates obtained from the laser group before and after LT throughout the 10-d treatment period are shown in Fig. 1, along with the corresponding differences between the flow rates measured before and after each exposure. The mean difference in the quantity of salivation (dQ-sal, mL/min) for the LT group, increased linearly from the initial 0.05 mL/min on the first day up to 0.13 mL/min on the last day of treatment. The results obtained from the control group treated with citric acid stimulation demonstrate a completely different patient reaction (Fig. 2). The difference (dQ-sal) in results obtained before and after the stimulation showed an increase during the first half of the treatment period, with a decrease close to the initial value toward the end of observation. The improvement in salivary flow rates for the laser group compared to the control group shows a statistically significant difference (p < 0.01).
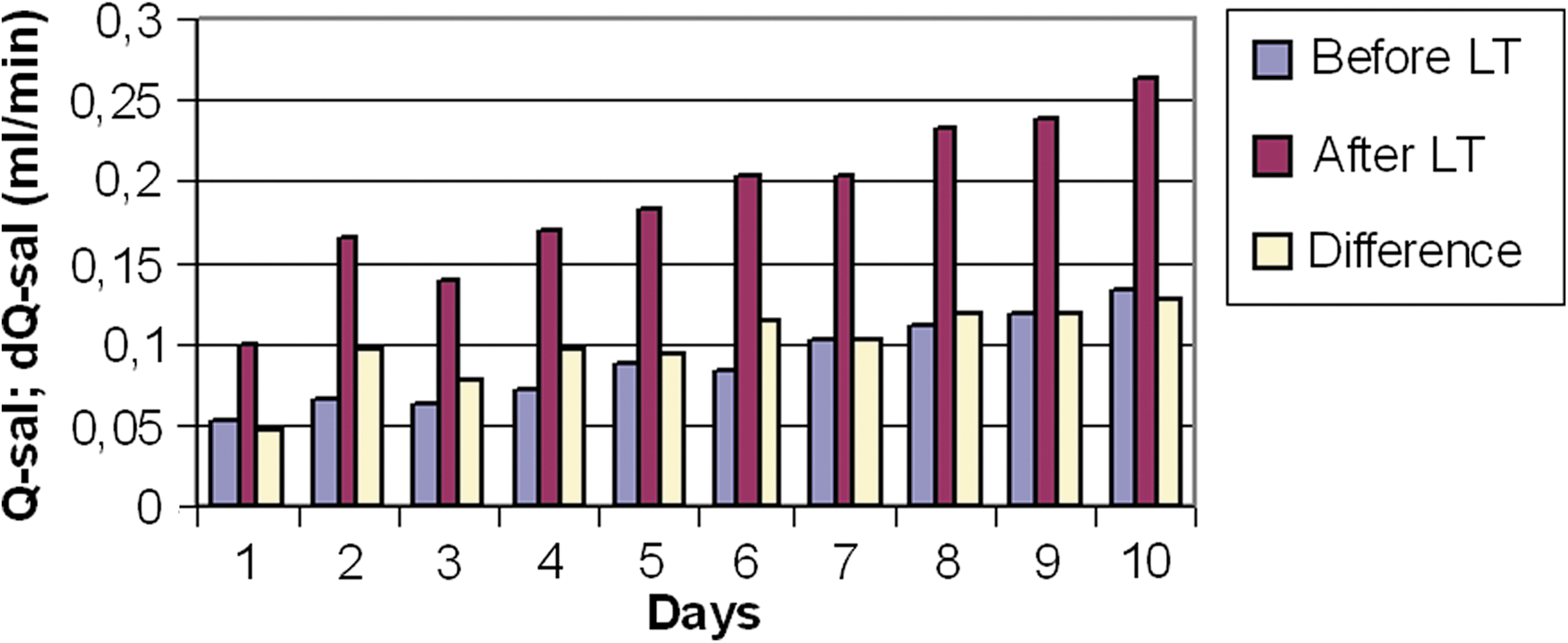
Salivary flow rates measured in the laser group during observation period.
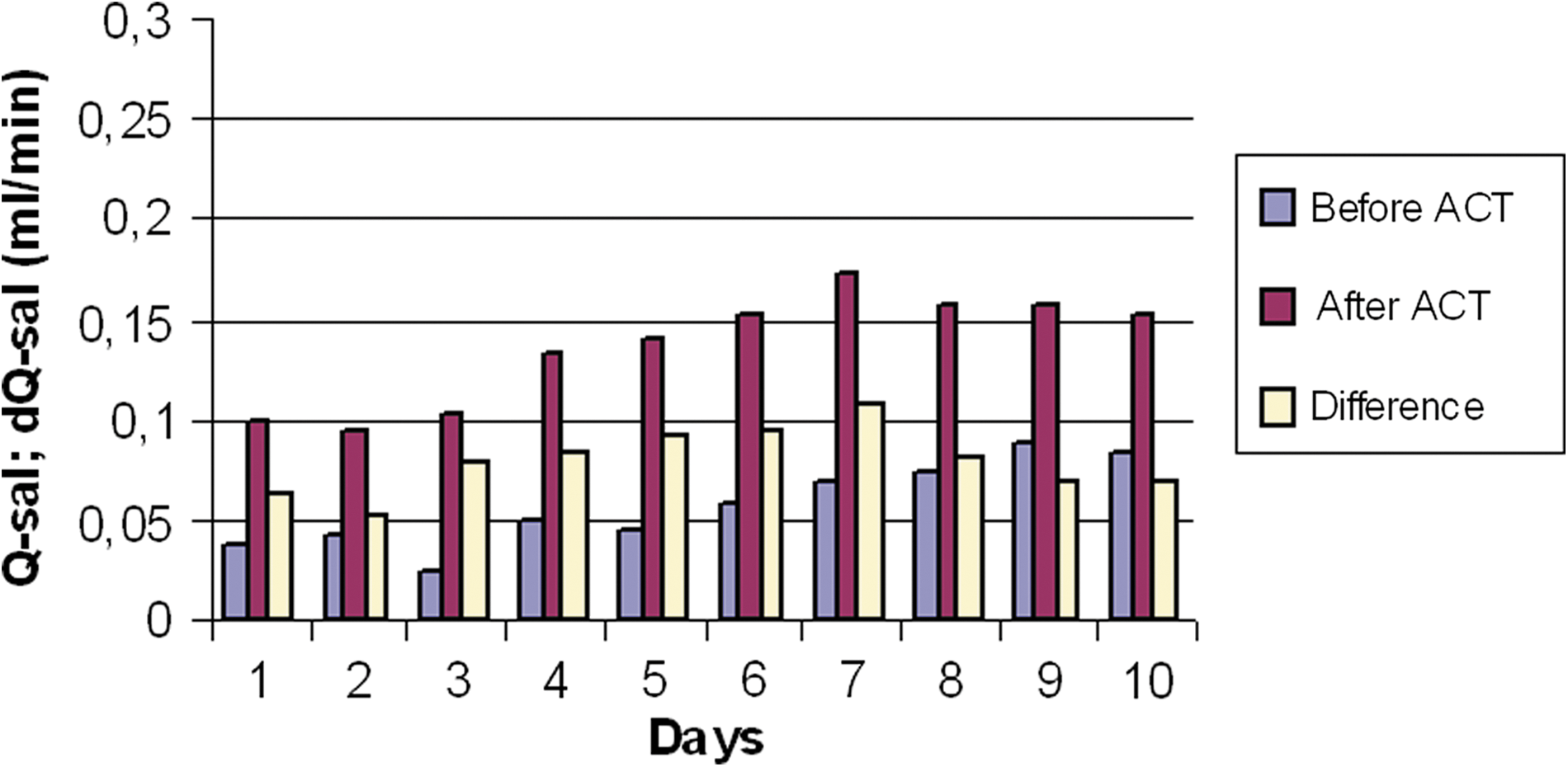
Salivary flow rates for the control group during observation period.
In Fig. 3 the difference (dQ-sal) before and after the stimulation for both the LT and control groups is depicted together with the corresponding data fits. During the considered observation period, the increase in the difference in salivary flow after LT was a linear function of the treatment time as represented by the corresponding linear fit of measured data exhibiting a relatively high regression coefficient (R 2 = 0.751). The change in the difference in salivary flow before and after LT observed in the control group showed no significant correlation with the treatment time (R 2 = 0.106).
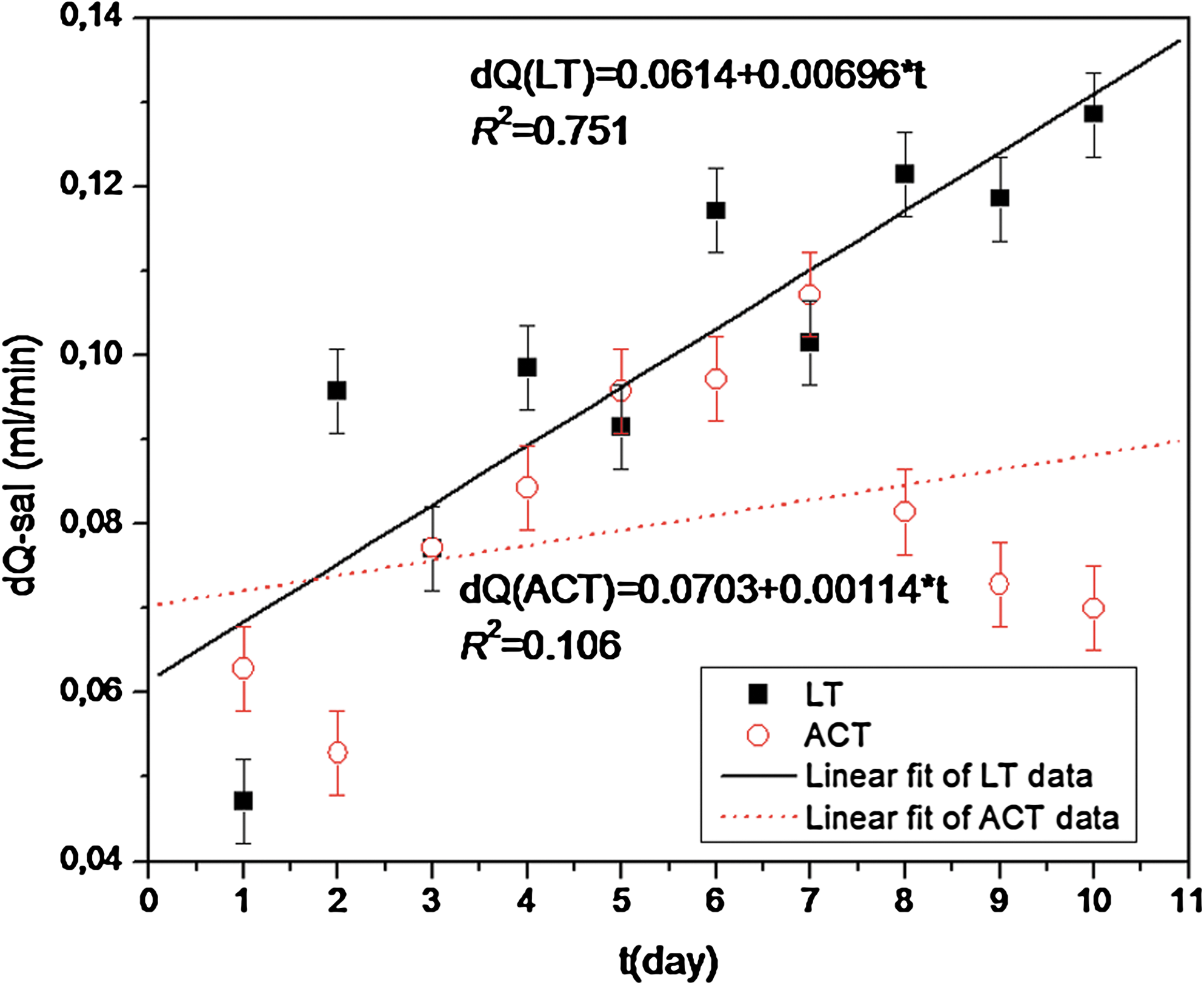
The difference in the quantum of salivation (dQ-sal, mL/min) recorded during the treatment of the laser group and the control group. The symbols represent measured data and lines represent corresponding linear fits.
Discussion
Our results show that the LT resulted in a continuous increase in salivary flow during treatment, while the results of the citric acid (ACT) treatment obtained from the control group exhibited a decline following an initial increase (Fig. 3).
The plot in Fig. 3 clearly shows that the response of the gland to the same amount of applied energy was not constant but increased linearly over time. The observed linear increase (R 2 = 0.751) in the average difference between the salivation flow before and after each LT during the therapy indicates that LT results not only in a temporarily stimulating effect on salivary glands but also has a regenerative effect, thus restoring the function of the salivary glands. One may expect that for prolonged treatment this trend would change and that the rate of increase in the difference in salivary flow would slow down and eventually reach a constant level, which would depend on the degree of the gland recovery.
The data for the control group show that the ACT stimulation also resulted in an initial increase in dQ-sal at levels comparable to those from the laser group. However, later in the therapy this initial trend was reversed and dQ-sal fell to its initial level. There was no correlation with the duration of the therapy (R 2 = 0.106), indicating that there was no significant improvement of the salivation function (Fig. 3). Hence, the observed effect is only a short-term response to ACT stimulation.
Contrary to the results obtained in some previous studies on experimental models that indicated possible adverse effects of laser irradiation on glandular tissue, 30 the patients involved in this study did not report any side effects or discomfort, thus confirming the results of recent studies showing that LLLT provides a broad therapeutic potential 16,17,31 –33 without significant adverse effects.
Results similar to those presented here were also obtained by other authors, although in case reports, small groups of patients, or animal models. 17,31 –33 However, according to our knowledge and available data, no other studies involving research on patients with xerostomia selected by applying criteria similar to ours have been published so far. Thus, we cannot compare our results with those from other studies.
Conclusions
The results of this preliminary study indicate that LLLT of salivary glands in patients with xerostomia may represent a beneficial adjunct to salivary flow stimulation and may even induce regenerative effects in salivary glands.
Further investigation is necessary on larger groups of patients, including placebo groups, to establish whether the observed effects are short-term or prolonged improvements in salivary flow rate, and also to determine the relevance and influence of certain parameters such as exposure time, average energy levels, wavelength, and probe distance.
Footnotes
Acknowledgments
This research was conducted under grant no. 065-982464-2532 from the Ministry of Science, Education and Sport of the Republic of Croatia.
Author Disclosure Statement
No competing financial interests exist.