
Abstract
Introduction
SRP is technically difficult and limited in its ability to remove or eradicate pathogens from deep periodontal pockets; bacterial invasion of periodontal tissues makes the treatment even more difficult. 14 –16 Therefore, other protocols have been used successfully in the treatment of periodontitis, such as the combination of mechanical debridement with laser therapy, aiming to potentiate the effects of SRP. 5 –8
Laser gingival curettage or laser curettage is a recent application of diode lasers in periodontics. 12,17 –20 Gingival curettage is a surgical procedure designed to remove the soft-tissue lining of the periodontal pocket, leaving only the gingival connective tissue. It is a separate procedure that may be performed in conjunction with or subsequent to SRP. The goal of SRP is the complete removal of bacteria, biofilm, calculus, and diseased root surfaces, and to create a biologically acceptable root surface. 21 SRP and gingival curettage are often performed simultaneously, which makes it difficult to determine their separate effects. Laser curettage of the pocket epithelium may contribute to the conventional treatment by retarding the migration of junctional epithelium, 22,23 interrupting the process of intracellular bacterial proliferation, removing diseased tissue, 24 and quantitatively reducing the number of microorganisms in infected periodontal pockets, 25 which may accelerate the process of periodontal wound healing. 26 –28
The correct use of a diode laser requires training, a minimum understanding of laser operation and functioning of an optical fiber delivery system, and efficient and safe protocols. Few published studies were found that investigated the reduction of laser power output (PO) caused by the contact of a silica-glass optical fiber with gingival tissues, or during periodontal debridement. 12,29,30
It is clinically known that the optical fiber tip needs to be frequently cleaved during surgical procedures. However, how do we know when it is time for the fiber tip to be cleaved? What is its effect on the clinical and microbiological results of periodontal therapy? Much of the knowledge that clinicians have about laser equipment and on protocols for laser therapy are based on their own clinical experience. More studies are needed to evaluate in vivo techniques and present their clinical results. Therefore, the aim of the present study was to evaluate the PO loss variation during laser curettage of infected periodontal pockets.
Materials and Methods
Experimental model
This was a secondary analysis of a clinical trial conducted with 32 patients with chronic periodontitis: an infectious disease characterized by the inflammation of periodontal tissues and progressive loss of conjunctive insertion. 27
Twelve patients, who attended the Special Laboratory of Laser Dentistry (LELO) at the University of São Paulo School of Dentistry (FOUSP), were selected to participate in the present study. The selection was performed by a specialist in periodontics. All 12 participants received SRP combined with high-power laser irradiation.
Patient selection and study design
The present study was approved by the Research Ethics Committee of FOUSP, Brazil, under the process number 129/04, and was conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. Written informed consent was obtained from all patients who agreed to participate in the study and responded to a medical history questionnaire.
SRP and laser treatment were performed by two periodontists. Clinical parameters were assessed 1 week before the treatment by a trained examiner (other than the periodontists). Eligibility criteria included patients with chronic periodontitis, aged from 30 to 65 years, who had good general health without evidence of systemic disease, did not use oral irrigators and/or antiseptic solutions for oral hygiene on a regular basis; and had a minimum of four teeth (four sites) with probing depth of 5–7 mm in at least one side of the tooth.
SRP was performed with the patient under local anesthesia (2% lidocaine hydrochloride with 1:100,000 epinephrine), which lasted for about 1 h. At the end of the session, each patient received two tablets of ibuprofen 200 mg and was instructed to take the pain medication, if needed. Periodontal treatment was performed during the entire study period. When any other dental treatment was necessary, the patient was referred to a different specialist of the Dental Clinic of the University of São Paulo.
Study group: SRP combined with high-power laser irradiation
Twelve selected patients received SRP combined with high-power laser irradiation (810-nm diode laser, Biolase, Irvine, CA). All of the periodontal pocket walls were irradiated according to the following procedure: a silica-glass optical fiber 400 μm in diameter, in contact mode, was inserted into the periodontal pocket 1 mm less than the pocket depth, 31 parallel to the long axis of the tooth, with a slight inclination toward the epithelial wall of the pocket. Next, laser curettage was performed on the entire surface of the tooth and pocket wall by rapid perpendicular movements of the optical fiber in the mesio-distal (horizontal) direction, and zigzag movements in the apico-occlusal (vertical) direction (Fig. 1). A sequence of predetermined application sites was adopted for the irradiation of the periodontal pockets. In order to prevent a residual temperature rise in sites that had not being irradiated, laser irradiation was delivered to alternate sites in the following sequence: mesio-buccal, disto-buccal, mesio-palatal, and disto-palatal. This made it possible to irradiate the entire surface of the tooth and pocket epithelium without touching the root cementum (Fig. 2).
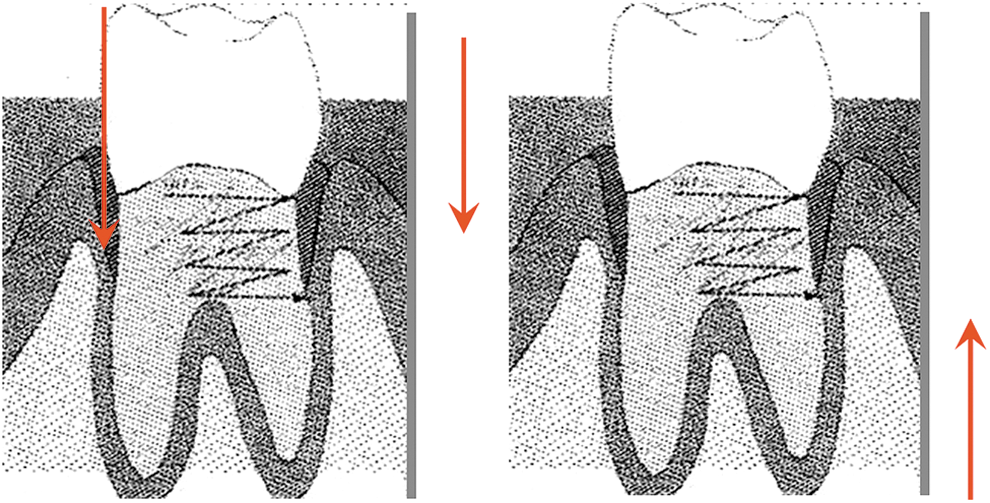
Diagram showing the movement of the fiber tip parallel to the long axis of the tooth, over the entire root surface, during laser irradiation (right). Rapid perpendicular movements (horizontal) (left). Movements in the apico-occlusal direction (vertical).

Laser curettage of diseased pocket epithelium. Photographs illustrating the application of high-power laser irradiation to infected periodontal pockets.
Four laser applications were performed per tooth (four periodontal pockets per tooth, around the entire root circumference). In the first irradiation, the laser was activated after the fiber had reached the calibrated depth. The duration of each application ranged from 10 (anterior teeth) to 15 sec (posterior teeth) per application site, depending upon the tooth anatomy, for a total of 40–60 sec per tooth. 10 Therefore, lower incisors, for example, received less laser irradiation (shorter irradiation time) than molars because of their reduced diameter. Immediately after the irradiation of each tooth was completed (every four applications), the fiber tip was freshly cleaved in an attempt to maintain the PO level at the tip of the optical fiber close to the laser power displayed on the control panel. Laser energy intensity ranged from 0.724 to 1.2 kW/cm2 (laser power, 1.7 W CW). Laser PO was measured with a power meter (Molectron, Coherent Inc., Santa Clara, CA) to standardize the energy applied to the application sites (Fig. 3). Before each measurement, the fiber tip was cleaned for debris with gauze moistened with saline solution. The mouth was rinsed with saline solution after laser curettage was completed.
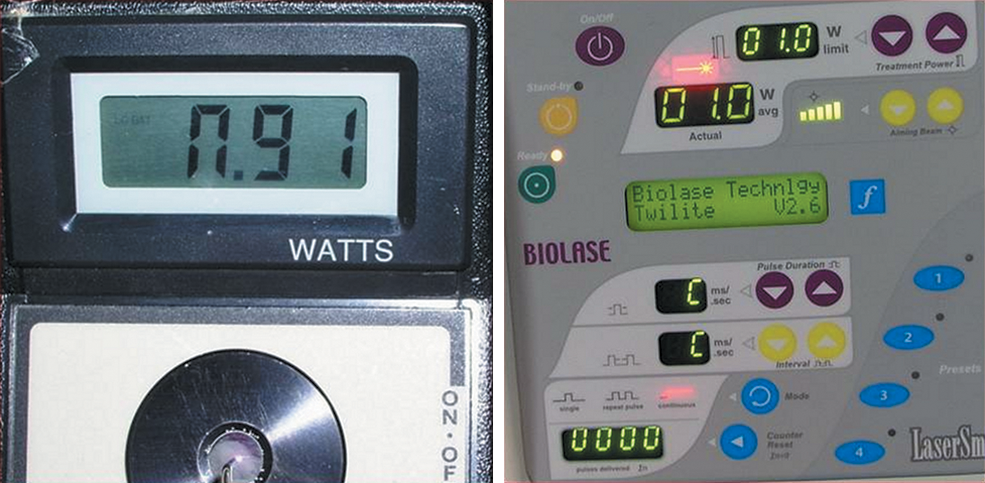
Power meter showing the PO measured at the optical fiber tip (left). Diode-laser control panel (right) displaying the laser power, which is higher than the PO measured by the power meter at the optical fiber tip.
Measurement of power loss during laser curettage
Four PO measurements were performed per tooth (except for one tooth in which only measurements for the first and second laser applications were obtained) for a total of 110 measurements.
A good cleavage is necessary to maximize PO at the fiber tip. Cleavage quality was evaluated by aiming the fiber at a flat surface and observing the shape of the spot created by the visible aiming beam. A uniform circular spot indicated a good cleavage. PO was measured at the tip of the optical fiber, using a power meter, prior to each laser application. Before each measurement, the laser power was set to 1 W at the control panel to facilitate mathematical analysis. After each PO measurement, laser power was increased from 1.0 to 1.7 W CW for the next application, and the periodontal pocket was irradiated as described previously.
Control measurements
In order to evaluate the transmission loss of a silica-glass optical fiber, 28 laser irradiations were performed without the fiber tip making contact with the teeth or gingival tissue. Laser power was set at 1.0 W CW at the control panel. The fiber tip was cleaved before each irradiation. The laser was switched on and the PO at the fiber tip was measured with a power meter. Four measurements of PO were made per irradiation at 15-sec intervals for a total of 112 measurements.
Statistical analysis
Repeated-measures analysis of variance (ANOVA) was performed to evaluate differences in mean PO between applications/irradiations within and between groups, with post-hoc comparisons between irradiations being made using a t-test for paired samples with Bonferroni correction, and post-hoc comparisons between groups being made using a t-test for independent samples. The Kolmogorov–Smirnov test was used to test for normality of residuals. Because of lack of normality, the non-parametric Mann–Whitney U test was performed for comparisons between groups, and the Friedman test was used for comparisons between irradiations. Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 17.0 for Windows (SPSS Inc., Chicago, IL). All statistical tests were performed at a significance level of 0.05 (p<0.05).
Results
In the study group, a mean PO loss of 54% (which includes a fiber transmission loss of 9%) was found between the laser power set at the control panel and the PO measured at the fiber tip after the fourth laser application.
There were significant differences in PO among groups (p<0.001), according to the Mann-Whitney U test. The mean PO values for each laser application are shown in Fig. 4. Measurements of PO at the fiber tip in each group obtained at a laser power of 1 W are shown in Table 1. Percent power losses between laser applications in each group measured at the optical fiber tip, at a laser power of 1 W, are shown in Table 2. The differences in PO measured at the tip of the optical fiber between applications/irradiations in each group are depicted in Table 3.
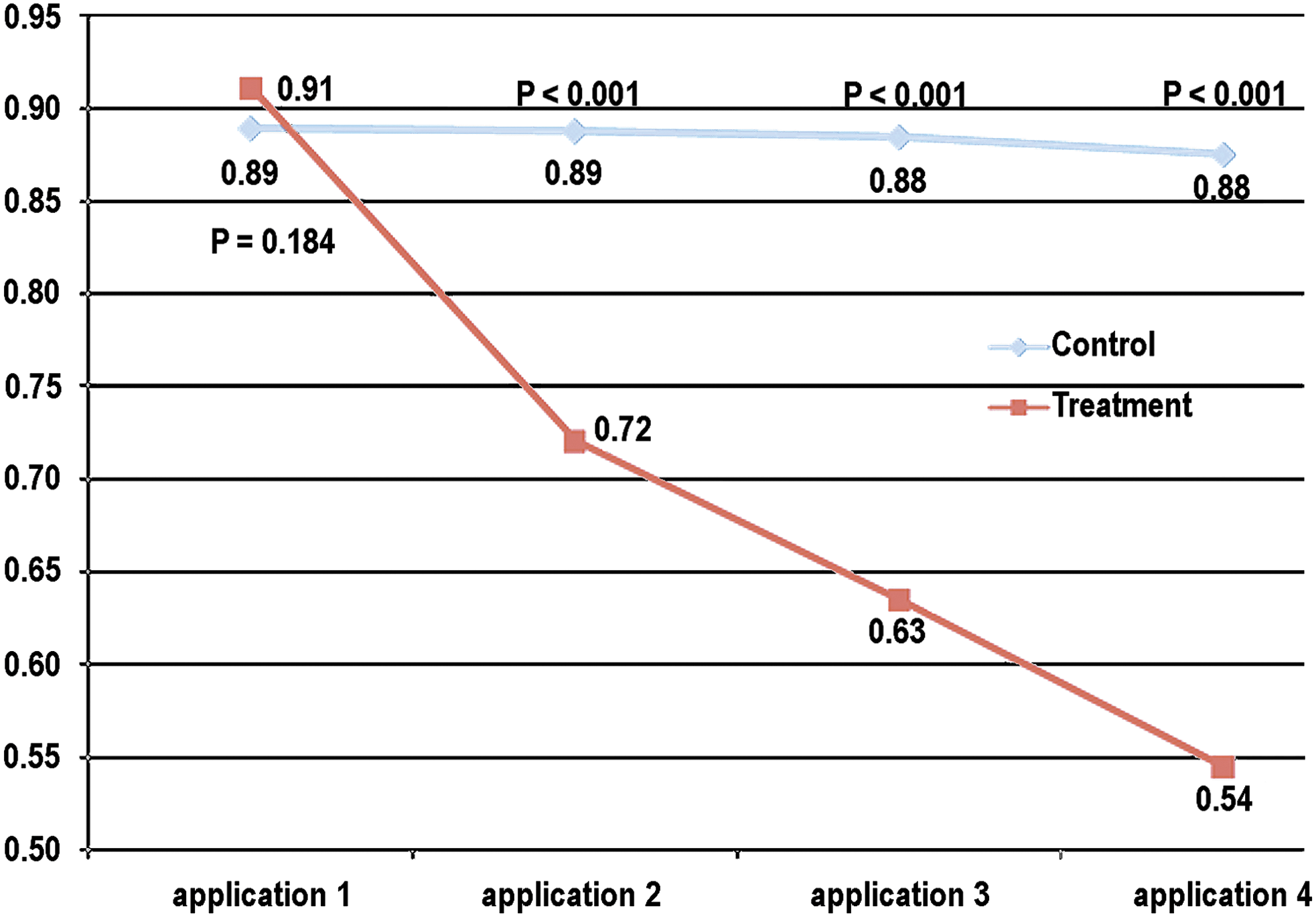
Comparison between groups of the mean PO at the optical fiber tip for each laser application at a laser power of 1 W.
Applic., application or irradiation.
Applic., applications or irradiations.
Applic., applications or irradiations; SD, standard deviation; SE, standard error.
In the study group, the relative power loss between applications significantly decreased at a constant rate from the first to the fourth application. Similarly, a relative power loss between irradiations was found in the control measurements, with significant differences between the third and fourth irradiations (p=0.016). However, the relative power loss between irradiations in the control measurements was much lower than that in the study group. PO values were normally distributed in the control measurements, according to the Kolmogorov–Smirnov test (first irradiation, p=0.921; second irradiation, p=0.920; third irradiation, p=0.730; fourth irradiation, p=0.939).
Discussion
For the safe use of lasers, operators need to know the control set value and actual PO during laser irradiation, as high PO can affect clinical safety and reduced PO is strongly associated with reduced clinical effectiveness.
To our knowledge, this is the first study showing the significant power loss that occurs during high-power diode laser gingival curettage. Kamma et al. 12 conducted a study using a 980-nm diode laser, operating at a laser power of 2 W CW for periodontal debridement and root surface decontamination. However, although the authors reported that the optical fiber was cleaved and PO was measured prior to and between successive treatments, their PO measurements were not published.
The present study revealed a marked and progressive loss of PO resulting from the contact of the tip to the optical fiber with gingival tissue. The cleaving of the fiber tip after few applications should be performed to minimize power loss. Power loss may decrease laser intensity to levels below those necessary to produce the desired microbial reduction.
In this study, the fiber tip was cleaved every four laser applications (after the entire circumference of the root of a tooth was irradiated) because of the high power loss detected during laser curettage. A mean fiber transmission loss of 9% was measured prior to the first application (before the fiber tip touched the gingival tissue). This is not in agreement with the findings of De Micheli et al., 32 who reported a fiber transmission loss of 20% during sham laser treatment (with the laser in non-contact mode), using a 400-μm silica-glass optical fiber. Our results revealed marked differences in the patterns of power loss between the two modes of irradiation (contact and non-contact modes). There was a significantly greater reduction in PO in the study group (contact mode) compared to the control measurements (non-contact mode). The mean PO at the second, third, and fourth applications were, respectively, 20.89%, 30.39%, and 40.26% smaller than the mean PO at the first application in the study group (contact mode), in contrast with 0.14%, 0.54%, and 1.58%, respectively, in the control measurements (non-contact mode).
Recent studies reported reduction in PO at quartz and sapphire contact tips after laser irradiation using a 2,936-nm Er:YAG laser in contact mode for tooth enamel ablation. 29,30 Eguro et al. 29 observed that the PO significantly decreased with time in both tips, and that the mean PO at the sapphire tip was higher than that at the quartz tip. Moreover, it is considered that the reduction in PO may be caused not only by the scattering and reflection of the laser beam at the irregular surface of the fiber tip, but also by tissue debris attached to the tips, which may result in further scattering or blocking of the laser beam. 29,30,33
Laser-tissue interaction
Studies examining the efficacy of the diode laser in periodontal debridement have been performed using different types of lasers, such as the 665-nm aluminum–germanium–arsenide (AlGeAs), 14 810-nm gallium–aluminum–arsenide (GaAlAs), 32,34 –36 655-nm GaAlAs, 37 and 980- nm diode lasers. 12,19 In most of these studies, there were minimal temperature increases over the 5°C accepted limit. In order to irradiate the periodontal pockets, the laser beam should be directed to the pocket epithelium, because, according to Radvar et al., 38 if the laser beam is positioned perpendicular to the coronal root surface it may cause damage to periodontal tissues. Damage was not observed with the laser beam parallel to this surface. Another factor to be considered is the energy absorbed by the surrounding tissue. According to Maiorana, 4 the adjacent tissues absorb little energy from the laser, because only ∼20% of the absorbed energy reaches depths >2 mm. This author also observed that it is necessary for the laser application to be performed with a continuous movement of the fiber tip, with or without water cooling, to prevent overexposure and overheating. In the present study, we chose to use brief and fast motions, but without water cooling in order not to reduce the thermal and antimicrobial effects of the laser. Kreisler et al. 39 reported that damage to the root cementum may occur depending upon the irradiation parameters, irradiation time, and angle of the laser beam with respect to the root surface, especially when the diode laser is used in continuous mode.
The protocol proposed in this study (810-nm diode laser operating at a laser power of 1.7 W, energy intensity range 0.724–1.2 kW/cm2, CW, irradiation time of 10–15 sec per site), was not found in the literature. However, these values were based on in vivo studies using diode laser irradiation to reduce the microbial population and for laser curettage of the pocket epithelium, attempting to prevent damage to the root surface and adjacent tissues. 5,6,40
Further studies are required to clarify the causes of PO loss at the optical fiber tip during laser irradiation of gingival tissues, and its effect on treatment outcome.
Conclusions
Our results revealed new and original information on the variation of PO at the tip of a silica-glass optical fiber after laser irradiation using an 810-nm diode laser for gingival curettage. There was a significant mean PO loss of 40.26% at the fiber tip between the first and fourth laser application. A mean power loss of 54% was found between the laser power displayed on the control panel and the PO at the fiber tip measured after the fourth application. A low- transmission loss of the optical fiber was observed in the control measurements (mean PO loss of 1.58% between the first and fourth irradiations).
Summary
Reduction in laser power output occurs because of the contact of the optical fiber with gingival tissues or during periodontal debridement. The purpose of this study was to evaluate power loss at the optical fiber tip during laser curettage of infected periodontal pockets. A significant power loss (mean, 40.26%) was observed after the periodontal debridement of a tooth, indicating that optical fiber tips need to be cleaved frequently during the procedure. It was also observed that application sites should be rotated during laser gingival curettage to minimize PO loss and prevent thermal damage.
Footnotes
Author Disclosure Statement
No competing financial interests exist.