
Abstract
Introduction
Light-induced thermal effects on tissue are important for diagnostics, therapy, and surgery. 12 –14 For thermal phototherapy and surgery, higher light power densities are used. The issues of controllable temperature rise and thermal or thermomechanical damage (coagulation, vaporization, vacuolization, pyrolysis, and ablation) of the tissue are paramount in these high-energy procedures. 15,16 Several models have been developed to describe the photo-induced thermal distribution for different geometries and approximations. 17,18
Some emerging techniques have been developed on the basis of photo-induced thermal effect in tissues. 19 –21 Recent advances in the development of noble metal nanostructures, with unique photophysical properties accounting for surface plasmon resonance, have allowed for the use of nanoparticles as highly-enhanced photo-absorbing agents. Based on this principle, a new photothermal therapy has been developed, plasmonic photothermal therapy (PPTT). 22
In some cases, such as PDT, in addition to the photochemical reaction, it is possible to locally increase the temperature of the tissue up to the hyperthermic range, >40 °C. The heating of the tissue could affect the desired therapeutic result. Therefore, it is very important to consider this phenomenon in order to improve understanding of the mechanism of action of PDT.
The studies related to the heating of the tissues by optical irradiation have been performed in vivo 23 and ex vivo. 24 –27 Some research of this phenomenon has been performed in phantoms. 28 –31 These studies involved experimental approaches 32,33 as well as model-based studies. 34 –36 Also, some attempts have been made to noninvasively reconstruct the thermal distribution, thermal properties of tissues, or the thermal damage during thermal methods for the diagnosis, planning, and monitoring of thermal treatments. 37 –40
Based on the foregoing, the study of photo-induced temperature rise in tissues is important for a better comprehension of the therapeutic and diagnostic effects of the various modern techniques based on the fundamentals of optical and thermal mechanisms of laser–tissue interactions. The present research uses a simple one-dimensional model and an experimental setup to determine the thermal penetration depth in some excised human tissues. The ultimate goal of this kind of study would be the characterization of in vivo tissues during the light–tissue interaction. However, the characterization of freshly excised tissues can be of interest in developing models for occasions in which blood perfusion is absent or diminished, whether naturally or artificially. This type of tissue-characterization research enables the further development of multicomponent models to describe photothermal effects on tissues.
Methods
Optical—thermal distribution model; effective thermal penetration depth
In this section, we propose an optical–thermal model to describe the temperature increase in tissues in absence of blood perfusion, as in the case of ex vivo samples. Several models have been previously proposed to describe the light–tissue interaction, depending upon the wavelength and energy of the incident radiation. For a wide-beam irradiation of semi-infinite samples, considering that light is scattered into an almost isotropic distribution near the irradiated surface, the one-dimensional diffusion model may be used;
2
the solution for the fluence rate being:
where φ is the fluence rate, which represents the incident flux of radiant energy over a small sphere divided by its cross-section; φ0 is the fluence rate at the irradiated surface, or the power density of the incident light beam; x is the distance from the irradiated surface; δ is the optical penetration depth; L is the radiance; 41 and Ω is the solid angle. The characterization of the optical penetration depth for several tissues has been previously reported using this approximation. 42 The optical penetration depth δ is the inverse of the total attenuation coefficient μT and it depends upon the optical absorption β and scattering coefficients μs , as well as on the anisotropy factor g according to the diffusion approximation:
where the reduced scattering coefficient is
For strongly dispersive media irradiated with a broad light beam, the fluence rate at the surface φ0
can be written as:
where Γd is the diffuse reflection coefficient (Γd=0.2 – 0.5), 43 and I0 is the power density of the incident beam.
The thermal response of the light-irradiated tissue depends upon its optical and thermal properties. After choosing the light propagation model for the tissue, the subsequent propagation and distribution of photo-induced heat can be described by the traditional bioheat equation:
44
where θ represents the temperature increase caused by photo-radiation over the body temperature, ρ is the mass density of the tissue, c is the tissue-specific heat, k is the thermal conductivity, β is the optical absorption coefficient, and χ is the thermal diffusivity (χ=k/ρc). The energy loss is determined by the tissue perfusion rate Q. The heat source term on the right side of Equation 4 was considered dependant upon the absorption of the optical radiation (βφ). It is dimensionally correct to introduce the thermal penetration depth δT
(δT
2
=k/ρcQ=χ/Q).
45
Accordingly, Equation 4 can be rewritten as:
If the irradiation time is comparable to the thermal relaxation time of the tissue, a steady-state situation can be assumed in order to solve the bioheat equation (5). For this situation, the second term on the left side of Equation 5 becomes zero. Because our measurements were performed on ex vivo tissue samples, the perfusion rate Q is also zero. Therefore, Equation 3 can be rewritten as:
Considering solution 1 for the one-dimensional case, Equation 6 turns into:
The solution to Equation 7, using the fluence rate at the surface (φ
0) in Equation 3, becomes:
The solution given by Equation 8 suggests that the temperature increase follows the same exponential decay as the fluence rate (Eq. 1), characterized by the optical penetration depth δ. It has to be noted that, as discussed below, this model does not satisfy our experimental results. Also, according to the definition of the thermal penetration depth used in Equation 5, for the ex vivo case (Q=0), the parameter δ T should be infinite, which would be nonsensical.
An important mechanism by which heat is transferred to the surrounding tissue, especially when the perfusion rate is at or near zero, is the conductivity caused by heat flux (q). It is represented by Fourier's law, which for the one-dimensional case can be expressed as:
For the steady-state case under the semi-infinite slab approximation, the heat flux will depend upon the difference between the temperature of the irradiated surface {T(0)} and the temperature at infinity {T(∞)}. If the temperature increase at point x is approximated by θ(x)=T(x)−T(∞), and T(∞) is assumed to be constant, then the equation
where parameter δeff fulfils the requirements of dimensional analysis and represents the effects of heat flux and energy loss caused by convective and radiative effects.
The one-dimensional solution, considering the diffusion approximation of light distribution (Eq. 1) and boundary condition (Eq. 3), will be:
From the value of the tissue's optical penetration depth δ for the incident wavelength and the measured increase in temperature at different depths x, it is possible to determine the value of the effective thermal penetration depth δeff
for the irradiated excised tissue. Thermal conductivity k for human tissues is ∼0.5 W/mK.
46,47
In Equation 11, θ(x) is a transcendental function with respect to δeff
. Its solution can be found graphically, by plotting two functions (F
1 and F
2) conveniently defined as functions of δeff
.
The intersection point of these two functions corresponds to the value of the thermal penetration depth (δeff ) for experimental point T(x). As an example, Fig. 1 shows a plot of functions F 1 and F 2 for blood (δ=0.20±0.01 mm) at a depth of x=8.5 mm. In each sample, the values of δeff determined at each depth are used to produce an average value for δeff .
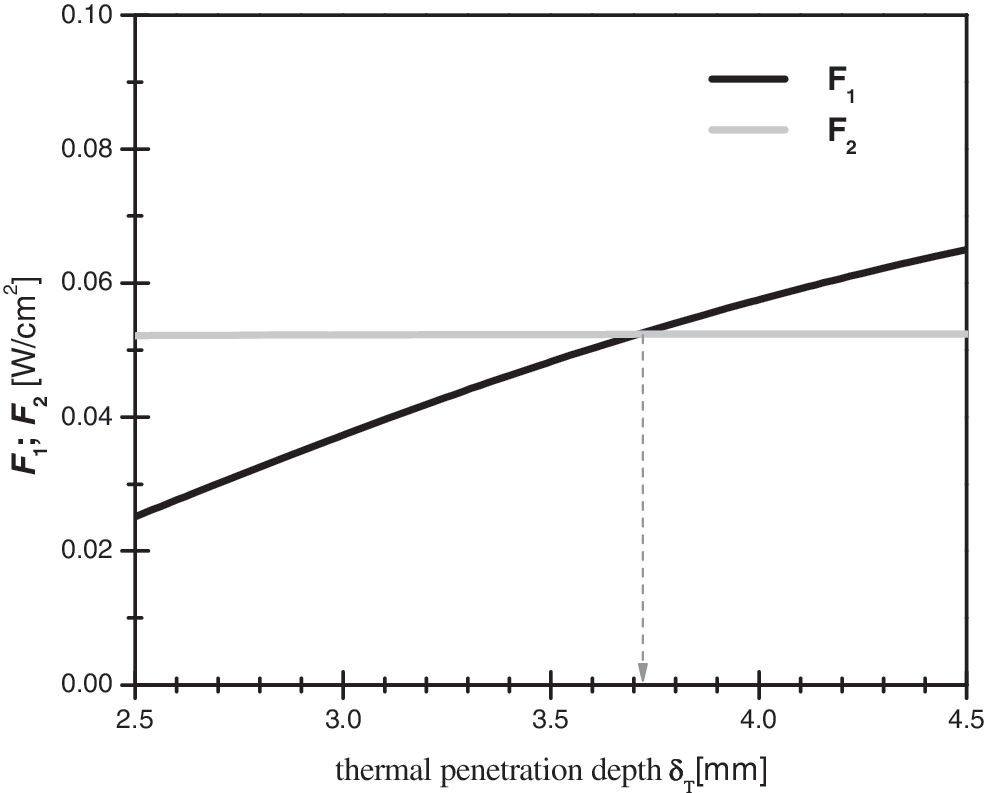
Plot of functions F1 and F2 used to determine the value of effective thermal penetration depth.
In Equation 10, convection, radiation, vaporization, and metabolic heat effects are not accounted for because of their negligible effect in many practical cases. The source term
Experimental setup
The experimental setup for measuring the photo-induced temperature increase as a function of depth is shown in Fig. 2. A 250 W xenon lamp was used as the light source. A simple optical system was designed to obtain a nearly parallel beam and a homogeneous illuminated spot 4 cm in diameter on the sample surface. The optical radiation was filtered to achieve a spectral band centered at 630 nm with a bandwidth of 70 nm. The power density of the red spot on the sample was determined to be 200 mW/cm2. The irradiation system was designed to properly match the wavelength (630 nm) that is widely used forPDT, using δ-aminolevulinic acid (δ-ALA), Photophrin® (Axcan Pharma, Birmingham, AL), and similar photosensitizers. On the other hand, this source is capable of delivering a sufficiently high irradiance to observe a temperature increase >40°C in the samples. The optical properties of the tissue samples were taken for the wavelength corresponding to the peak of the obtained optical band.
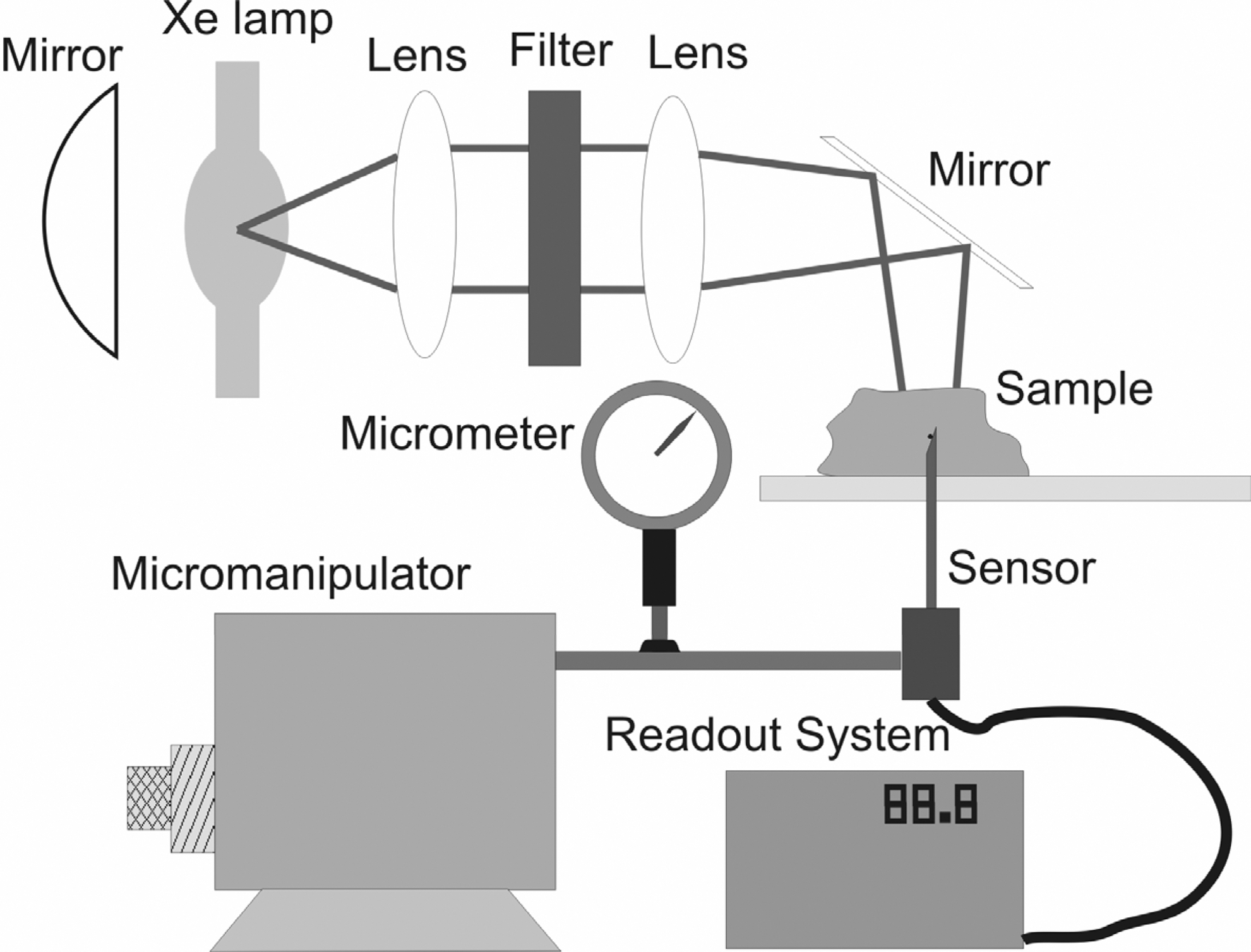
Experimental setup for measuring the photo-induced temperature increase for different depths.
To comply with the semi-infinite slab condition required by the one-dimensional diffusion model (Eq. 1), the sample must be thick enough. This means that the linear dimensions of the measured piece of excised tissue must be much larger than the expected optical penetration depth. The colon samples were measured with their naturally-adhered tissue in order to obtain a significantly thick sample. However, a two-layer model would give a more correct result for this type of tissue. Likewise, a similar semi-infinite slab condition was assured for the one-dimnesional approximation of the bioheat equation solution (Eq. 11). Therefore, the samples were considered thick enough to ensure that the temperature rise at their distal borders equalled zero.
A NiCr-NiAl thermocouple (type K) of 125 μm in diameter was used as the temperature sensor. Considering that the thermal conductivity values 49 for glass (k∼1 W/mK) are much closer to the typical value for human tissues (k∼0.5 W/mK), and about 15 times smaller than the thermal conductivity values for stainless steel (k∼15 W/mK), a glass pipe of similar size and geometry was used instead of a stainless steel hypodermic needle, in order to reduce the heat exchange across the length of the measuring probe. In this way, this source of error was minimized from our experiment. The temperature readouts were performed with a digital thermometer accurate to 0.1°C. A micromanipulator allowed for an accuracy of 0.01 mm in the displacement of the temperature sensor inside the samples. This displacement was controlled by a micrometer. The temperature measurements were performed after 7–8 min of irradiance, which complies with the steady-state approximation for the thermal distribution.
The blood, colon, breast, lipoma, axilla, lung, and liver tissue samples were taken during surgery and measured within 2 h thereof in order to diminish the effects of natural tissue degradation after excision. During the manipulation, the samples were kept under a moist cotton tissue to retard the drying process as much as possible.
Results
Figure 3 shows that, for a hypothetical tissue, under the approximation proposed by Svaasand et al. (Eq. 5),
43
the hyperthermic state (>40 °C) is achieved at a relatively large depth (∼10 mm) when δ=2 mm, δT=7 mm, k=0.5 W/mK, Γ=0.5, and I
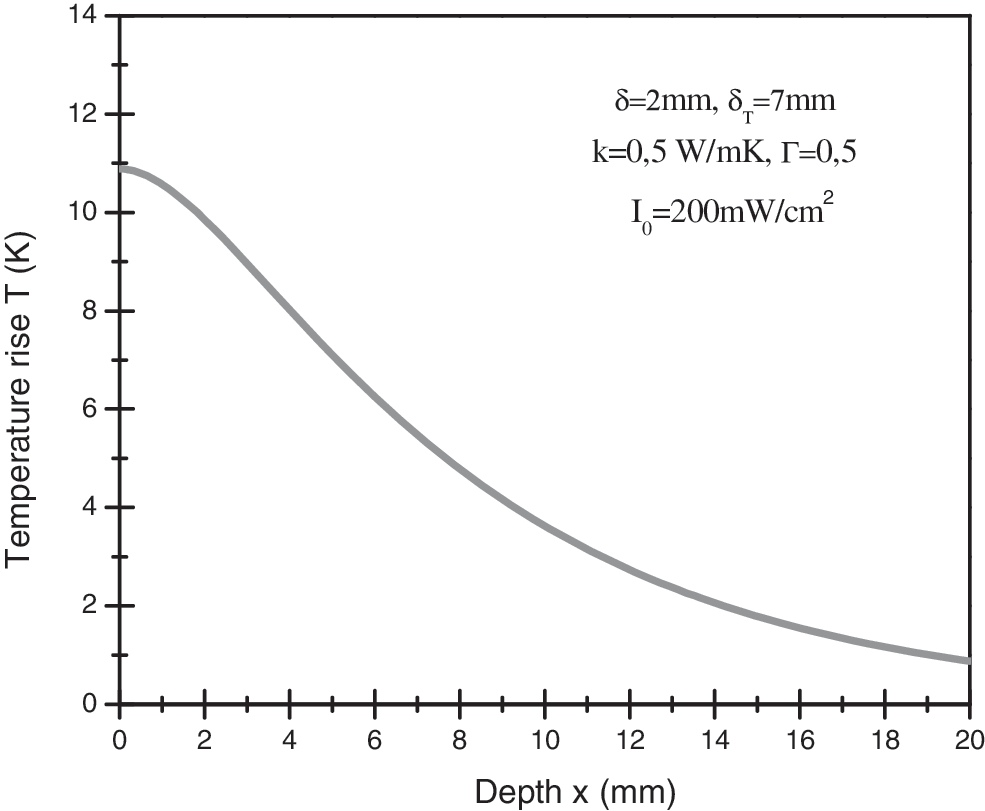
Solution to the bioheat diffusion equation for a hypothetical tissue.
Figure 4 shows the experimentally-measured temperature increase as a function of depth for a photo-irradiated sample of blood (dotted curve). The experimental data were processed using the functions (F 1 and F 2) described in Equation 12. Accordingly, the values for the effective thermal penetration depths were obtained graphically from the intersection point of F 1 with F 2 for each measured point, and then averaged. The effective thermal penetration depth for blood was determined to be δeff = (4.3±0.4) mm. The optical penetration depth for this sample, obtained using a previously described method, 42 was δ =(0.20±0.01) mm.
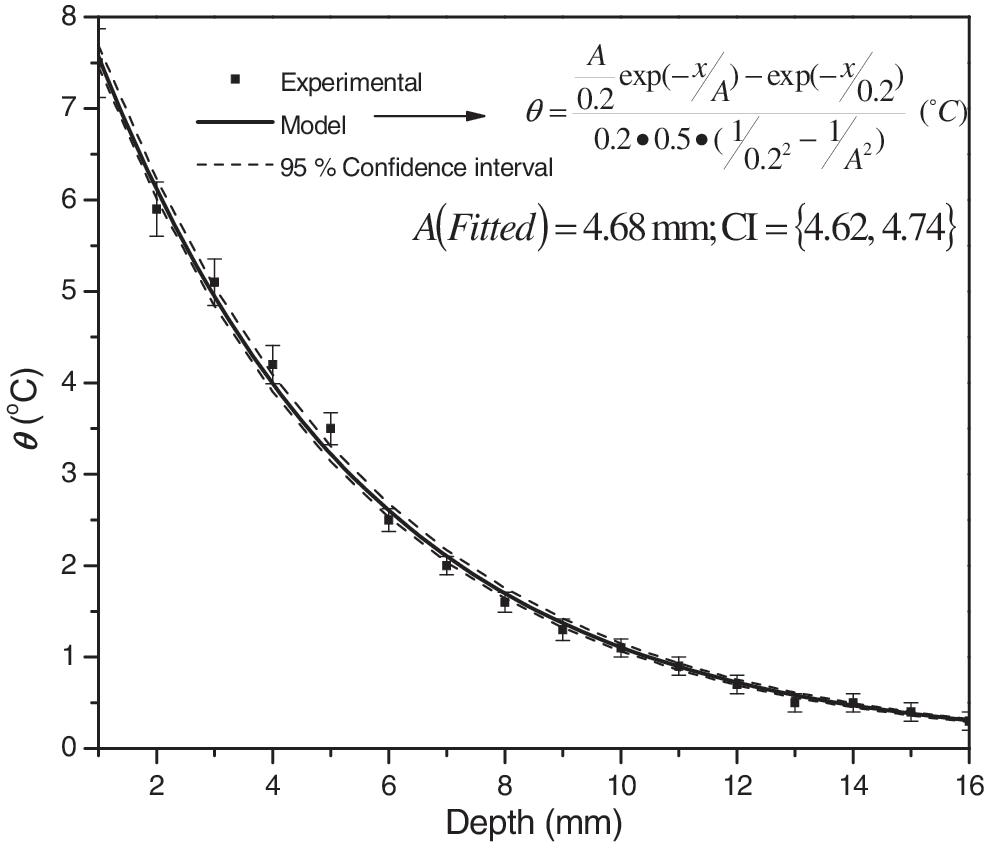
Experimentally measured temperature distribution in a photo-irradiated sample of blood (dotted curve). The solid line represents the best fit to the model solution, Equation 10.
The solid line in Fig. 4 represents the nonlinear regression best fit to the experimental data. The fitting process was based on Equation 11, with the effective thermal penetration depth as the fitting parameter. The fitting function is given in Fig. 4; A being the parameter to be evaluated during the fitting process. It can be seen that this parameter corresponds to the effective thermal penetration depth δeff .
The values of thermal conductivity (k=0,5 W/mK), reflectivity (Γ=0,5), and power density on the irradiated surface (I
The best fitted value of the effective thermal penetration depth δeff for blood was 4.68 mm, with a 95% confidence interval of 4.62 –4.74 mm. This result agrees with the calculated values of the effective thermal penetration depth (δeff ) in blood using the graphical method previously described.
Similar graphs were obtained for the colon, breast, lipoma, axilla, lung, and liver tissues under study. In all cases, a similar agreement was obtained between the calculated values of the effective thermal penetration depth using the graphical method with functions given by Equation 12, and the estimated parameter using the solution to the bioheat Equation 11 as the fitting function.
As an example, Table 1 shows the values of the effective thermal penetration depth determined from the temperature increase measured at different depths in a breast tissue sample. The mean value of the effective thermal penetration depth (δeff ) is given in the last row of the table.
δeff =(5.37±0.31) mm.
The mean value of the effective thermal penetration depth was also calculated and reported for all of the studied samples. Table 2 shows the values of δeff and δ for these samples. The values of the optical penetration depth δ were obtained to determine the effective thermal penetration depths, following the method presented elsewhere. 42 In all cases, the value of δeff is significantly larger than that of δ. The fourth column of Table 2 presents the values of the ratios of the effective thermal-to-optical penetration depths. This ratio is a measure of how distant a thermal response in the tissue could be expected from that of the layers absorbing the optical radiation. Comparing the results in Table 2, it can be seen that, for porous tissues such as liver and lung, the effective thermal penetration depth δeff is very close to that of the value in blood. It can be concluded that, for these tissues, the effective thermal penetration depth δeff is determined by the presence of blood.
Discussion
The light–tissue interaction has been described with a simple model detailing the photo-induced temperature increase. The one-dimensional solution for the bioheat model of a hypothetical tissue, with typical optical and thermal parameters, suggests that a relatively large volume of the irradiated tissue reaches the hyperthermic state. This fact shows the necessity of considering the thermal effect during PDT or other sufficiently high-powered optical radiation treatments, particularly when the therapeutic results are discussed.
A good agreement was observed between the model solution and the experimentally-measured temperature increase at different depths in the studied samples. This model can be used to evaluate the potential increase in temperature for different depths when the surface of the tissue is irradiated with a broad light spot.
Comparing the values of effective thermal and optical penetration depths, the following can be concluded for all of the studied tissues. The volume, in which the effect of temperature increase caused by optical absorption takes place, is larger than the volume of tissue where the light is absorbed and the photochemical processes occur.
The effective thermal-to-optical penetration depth ratio (δeff /δ) is maximum in blood. This indicates that, although the optical penetration depth at 630 nm is small in blood compared to the rest of the tissues, the temperature rise with depth is similar in blood and the rest of the studied tissues. It can be concluded that in porous tissues, such as liver and lung, the presence of blood allows for a deeper heat penetration.
The experiments were performed using a 70-nm-width spectral band, centered at 630 nm. Strictly speaking, optical penetration depth is wavelength-dependent. Therefore, the effective thermal penetration depth is (in principle) wavelength-dependent. For wavelengths with more penetration into the tissue, it means in the near-infrared zone of the optical window, the absorption could occur in deeper layers of the tissue, increasing the effective thermal penetration depth. Complementary studies should be performed to study the possible consequences of this dependency. There is more than one set of values of β, μs, and g for every specific value of δ (see Eq. 2). The temperature increases as a result of the absorption of the incident energy of light; however, the scattering properties of the tissue will affect the distribution of the optical radiation within the tissue; therefore, they will determine how much optical energy could be absorbed at each point. Consequently, thermal distribution depends also upon the scattering properties of the tissue. In a specific tissue, the temperature at the irradiated surface or near the inserted fiber tip will be higher as the reduced scattering coefficient increases and therefore the effective thermal penetration depth decreases.
In the case of in vivo tissues, the thermal penetration depth δ T will depend upon the blood perfusion rate as mentioned previously (Eq. 4). The thermal penetration depth δ T increases for tissues with lower values of perfusion rate Q. 50,51
Another fact to account for during the photo-irradiation in vivo, is the dynamic change of optical parameters caused by coagulation, and for a higher irradiance, the protein denaturation and the charring of the tissue. 32,52
The dynamic behavior of optical properties of tissues, depending upon the temperature, have been widely reported,
53,54
mostly for temperatures >45°C, when huge changes in optical properties seem to start.
55
However, there are scarce reports on temperature effects on tissue optical properties <45°C. Laufer et al., in an ex vivo study on skin samples,
26
reported an increase of the reduced scattering coefficient
More research should be done to properly understand and describe the photothermal interaction in the temperature range <45°C when the photo-induced coagulation and protein denaturation have not yet begun.
Conclusions
In this study, the concept of the effective thermal penetration depth in tissues has been defined as a parameter not dependant upon the perfusion rate of blood, but on the wavelength of the incident optical radiation, and the optical and thermal characteristics of the tissue. This could be useful for developing models to describe the thermal effects with a separate analysis of the tissue itself and the blood that irrigates it.
The effects of the heating the tissues <45°C has not been sufficiently studied. A better understanding of the thermal effects in this temperature range will certainly enable the improvement of the results of light-based therapeutic methods with irradiances around a few hundredths of a mW/cm2.
Footnotes
Author Disclosure Statement
No competing financial interests exist.