
Abstract
Introduction
BP-related osteonecrosis of the jaws (BRONJ) is an adverse side effect of long-term BP therapy (BPT), which was first described in 2003. 3 –5
Low risk of BRONJ development has been reported in non-cancer patients (range: 0.01–0.04%) whereas high risk is associated with intravenous administration of nitrogen-containing bisphosphonates (nBPs) in cancer patients (range: 0.8–12%). 6,7
A clinical staging system for BRONJ was proposed in 2006 by Ruggiero et al. 8 in order to compare results of different approaches (Table 1). Such a staging system was modified in 2009. 9
Levels A and B should be maintained for at least 6 months after therapy.
Adapted from Vescovi, P., Merigo, E., Meleti, M., and Manfredi, M. (2006). Bisphosphonate-associated osteonecrosis (BON) of the jaws: a possible treatment? J. Oral Maxillofac. Surg. 64, 1460–1462.
Management of BRONJ is still controversial. No treatment has shown to have a proven efficacy and the interruption of BP administration does not seem to be beneficial 10 in terms of BRONJ incidence reduction.
A considerable improvement of symptoms has been documented after use of oral antimicrobial rinses, in combination with systemic (oral or intravenous) antibiotic therapy for all BRONJ stages. However, effects of antibiotic treatment are usually not persistent, and patients often require repetition of drug therapy for a long-term maintenance. 8
Some benefits after hyperbaric oxygen therapy (HBO) and ozone therapy have been described in patients with BRONJ. 11,12 Such positive results, however, have not been confirmed by other studies.
In early reports, surgical treatment was restricted to patients affected by stage III BRONJ. However, current guidelines suggest a conservative surgical approach (e.g., elimination of bone sequestra and necrotic bone debridement) also for stage II BRONJ. 9,13 –15
The effects of different laser wavelengths on the metabolism of bone, skin, and mucosa (both in vivo and in vitro) have been extensively documented. Several studies have shown the positive effect of LLLT in terms of improvement and fastening of the wound healing process. 16,17 Studies on LLLT tested a wide range of wavelengths ranging from 532 (green) to 2940 nm (infrared); with the majority of research reporting red-light visible and infrared light (1064 nm) sources. 18 Laser beam produces some changes in cellular metabolism, probably with a photochemical mechanism, 19 and with an intensity of the effects based on cell physiological status during the irradiation and on the wavelength used. 20
BPs produce suppression of the bone turnover with increase in bone micro-damage accumulation from 2 to 7%, 21 and are characterized by soft tissue toxicity caused by the influence on viability, migration, and apoptosis of the oral keratinocytes and fibroblasts, thus resulting in an inhibition of normal soft tissue healing around postextractive or local prosthetic trauma. 22,23 The LLLT capability to promote bone resorption and remodelling, 24,25 with a two-step mechanism linked to the subsequent activation of osteoblasts and osteoclasts, could give support for a possible usefulness of laser biostimulation in the treatment of BRONJ.
Vescovi et al. recently showed that intra- and postoperative laser biostimulation may be of some help in the promotion of mucosal/bone healing, particularly when LLLT is used for the treatment of early stages lesions. 17
Oral soft tissue healing process is improved by LLLT with the abbreviation of the exudative phase and the stimulation of reparative processes, and also by the transformation of fibroblasts in myofibroblasts, 26 the increase of blood flow by means angiogenesis and capillarity growth, 27 as well of growth factor release (TGF-PDGF-bFGF-IL6-IL8-IL1α), 28 –30 the faster formation, and increased deposition of collagen type I and III. 31 –33
An active role of bacterial infections (e.g., Actinomyces) in the pathogenesis BRONJ has been hypothesized by different authors. Microbial antibacterial activity of LLLT has been shown in vitro and in animal model studies, with different wavelengths. 34,35
On the basis of these previous considerations, LLLT appears to be a promising solution for the management of a condition of avascular and infected osteonecrosis such as BRONJ. 36 –38
Nd:YAG laser biostimulation could be useful for the treatment of BRONJ with or without surgical treatment, increasing speeding up of the healing process. 39 –42
The Er:YAG laser has great potential for hard tissue treatment, providing clean and precise cuts with minimal injury to the adjacent hard and soft tissues, while producing an ablated surface favourable for cell attachment with a bactericidal and biostimulatory effect. Some studies have documented the usefulness of this wavelength to efficiently ablate bone in patients affected by BRONJ. 43 –45
Patients and Methods
One hundred and twenty-eight patients (33 males, 95 females; 52 with MM, 53 BM, and 23 OP) affected by BRONJ were evaluated at the Unit of Oral Pathology and Medicine and Laser-Assisted Surgery of the University of Parma, Italy, between January 2004 and July 2009. At the time of BRONJ diagnosis, mean duration of BPT was 28 months (ranging between 1 and 96 months). Twenty-six patients (20.3%) were smokers, 9 (7.03%) had diabetes, and 89 (70.1%) had received long-term corticosteroid treatments. These additional risks factors were uniformly distributed into four groups of treatment.
Eighty-five out of 128 patients (66.4%) had mandibular involvement, 30 out of 128 (23.43%) had BRONJ in the maxilla, and 13 out of 128 (10.15%) had the involvement of both the jawbones. All of these patients were subclassified according to the staging system proposed by the AAOMS 9 in the following groups: stage I (17/128), stage II (92/128), and stage III (19/128) (Tables 1 and 2).
Healing improvement: BRONJ sites after medical or surgical treatments (with or without LLLT) that progressed to “clinical success” a) stage 0 or b) passed from higher stage to a lower one (for at least 6 months).
Initial stage: each BRONJ lesion was classified as stage I, II, III at the time of the first clinical evaluation, according to Ruggiero et al. classification. 8
The overall number of BRONJ sites was 151, and the number of treated sites was 101.
Inclusion criteria for treatment were the presence of exposed or unexposed symptomatic BRONJ. Patients satisfying inclusion criteria but presenting a very poor health condition, mandibular fracture, or diffused stage III BRONJ not treatable under local anaesthesia were not included in the present evaluation.
An ortopantomography (OPT) and a CT scan of the lesion were obtained in all cases.
In each case the first therapeutic approach was chosen on the basis of the most updated guidelines available at the time of treatment. Surgical approach was taken into account after three consecutive antibiotic cycles not leading to a stable improvement of BRONJ. Each surgical intervention was performed with the patient under local anaesthesia, and planned according to the extension of the lesion. In all surgical cases, mucoperiosteal flaps were elevated to visualize and remove the necrotic bone. Surgical instruments included conventional bone burs or Er:YAG laser. A complete closure of the surgical wound was performed through conventional sutures.
In addition to antibiotic or surgical treatment in two separate groups, we performed LLLT applications using Nd:YAG laser. 39 According to the ethical standards of the Academic Hospital of Parma, we obtained a specific informed consent for each patient.
In order to assess the efficacy of different treatments, sites were subclassified as follows (Table 3):
Healing improvement: BRONJ sites after medical or surgical treatments (with or without LLLT) that progressed to “clinical success” a) stage 0 or b) passed from higher stage to a lower one (for at least 6 months).
G1: BRONJ sites treated only with antibiotic therapy
G2:BRONJ sites treated with antibiotic therapy and LLLT
G3:BRONJ sites treated with antibiotic and surgical therapy
G4: BRONJ sites treated with antibiotics, surgical therapy, and LLLT
In G1, 12 sites were treated with medical therapy with antibiotics (oral amoxicillin 1g 2 times/day with oral metronidazole 250 mg 2 times/day) for 2 weeks. Mouthwashes with chlorhexidine (0.20%) and hydrogen peroxide (3%) were also prescribed 2–3 times a day, sometimes with antimycotic rinses. Clinical examination of the lesions was performed 2 weeks after therapy and 3 weeks after antibiotics suspension as well. Of these 12 sites, 0/12 was classified at the time of first clinical evaluation as stage I, 9/12 (66.6%) were classified as stage II, and 3/12 (33.33%) were classified as stage III (Table 2).
In G2, 27 sites received medical treatment (as described for G1) in association with cycles of LLLT. In particular, each lesion received LLLT applications once a week for 2 months. Each LLLT application was performed with Nd:YAG Laser (1064 nm, Fidelis Plus, Fotona, Slovenia) used at 1.25 W average power, 15 Hz frequency (Duty cycle: 0,15%) and 320 μm of fiber diameter. The laser light was used in a non-focused way, 2 mm from tissue, for 1 min (power density: 268.81 W/cm2, fluence:14.37 J/cm2) and repeated five times. Of these 27 lesions, 5/27 (18.5%) were classified at the time of first clinical evaluation as stage I, 21/27 (77.8%) were classified as stage II, and 1/27 (3.7%) were classified as stage III.
In G3, 17 sites were treated with surgical therapy in association with medical therapy. Antibiotic treatment was usually prescribed beginning 3 days prior to the operation and ending 10 days after it. Conservative (and, when possible, early) surgical treatments reserved for those lesions consisted of (1) sequestrectomy of necrotic bone, (2) superficial debridement/curettage, or (3) corticotomy/surgical removal of alveolar and/or cortical bone. Operations were performed using traditional surgical instruments: a cold blade scalpel to incise mucosal tissues and rotary cutting instruments to remove necrotic bone. 41
Of these treated 17 lesions, 3/17 (17.7%) were classified at the time of the first clinical evaluation as stage I, 13/17 (76.5%) were classified as stage II and 1/17 (5.9%) was classified as stage III.
In G4 (Figs. 1 –7), 45 sites were treated with medical and surgical therapy in association with LLLT (Nd:YAG laser) applications. Surgical operations were performed as described for G3, in association with laser Nd:YAG biostimulation (1.25 W power, 15 Hz frequency, fiber of 320 μm). The laser light was used as described for G2. The first application of LLLT was performed during the surgical intervention. The operated site was then treated every week with LLLT applications (same protocol described for G2) for 2 months. Of these treated 45 lesions, 9/45 (20%) were classified at the time of the first clinical evaluation as stage I, 35/45 (77.8%) were classified as stage II, and 1/45 (2.2%) were classified as stage III.
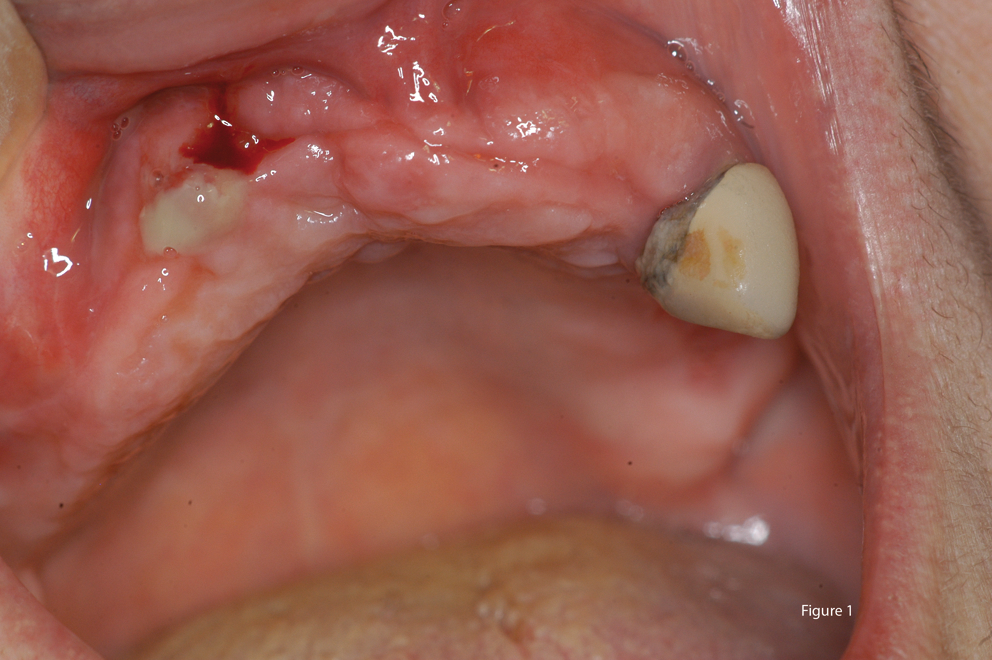
Clinical image of stage III maxillary BRONJ for the patient, a 65-year-old female treated with aledronate for osteoporosis for 48 months.
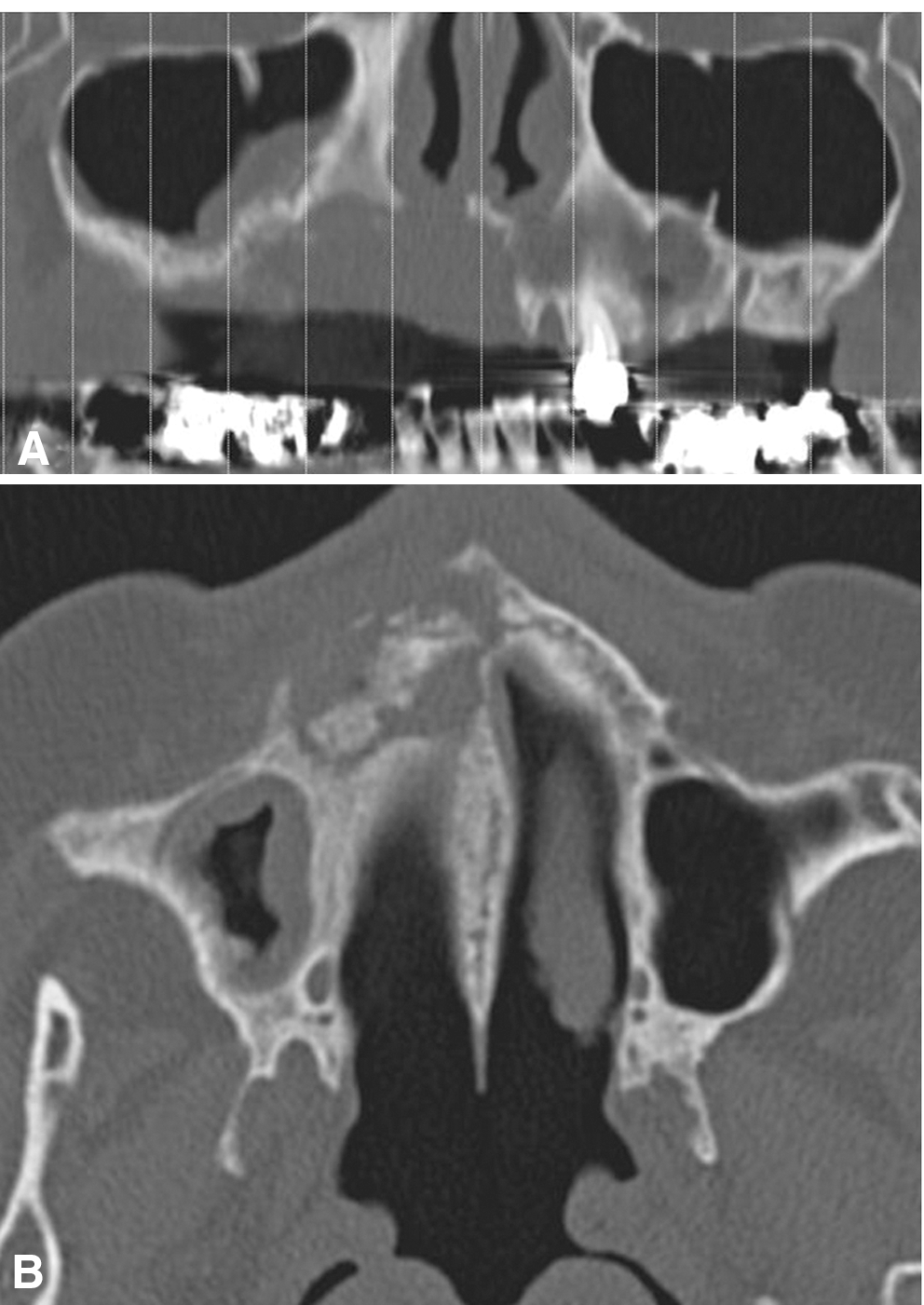
Radiographical images of stage III maxillary BRONJ of patient in Figure 1, showing signs of infection and sinusitis.
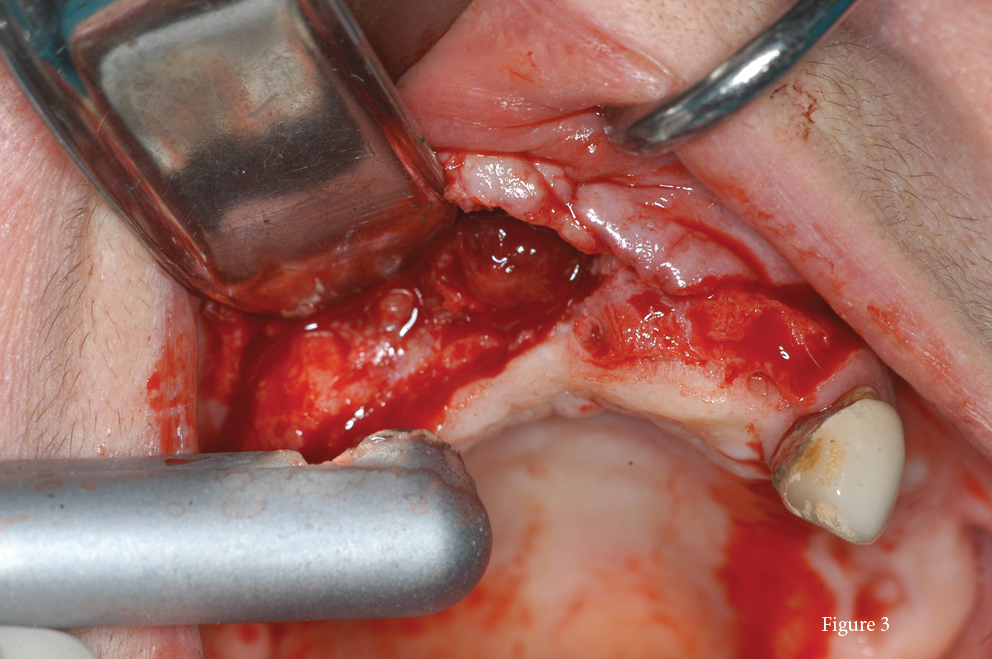
Surgical Er:YAG laser-assisted treatment of patient.
Iodopovidone solution cleaning of the surgical site.
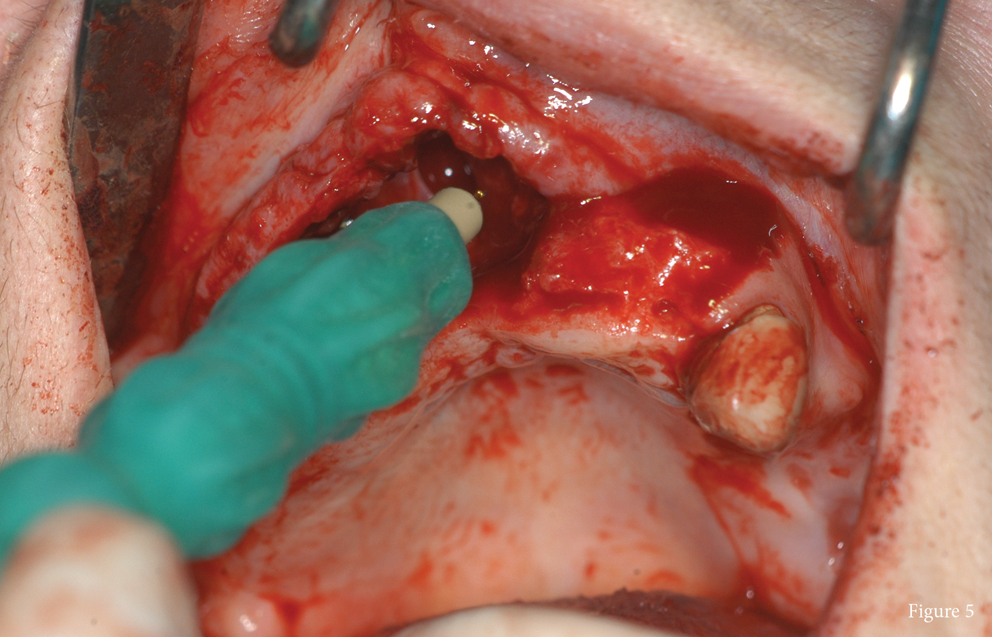
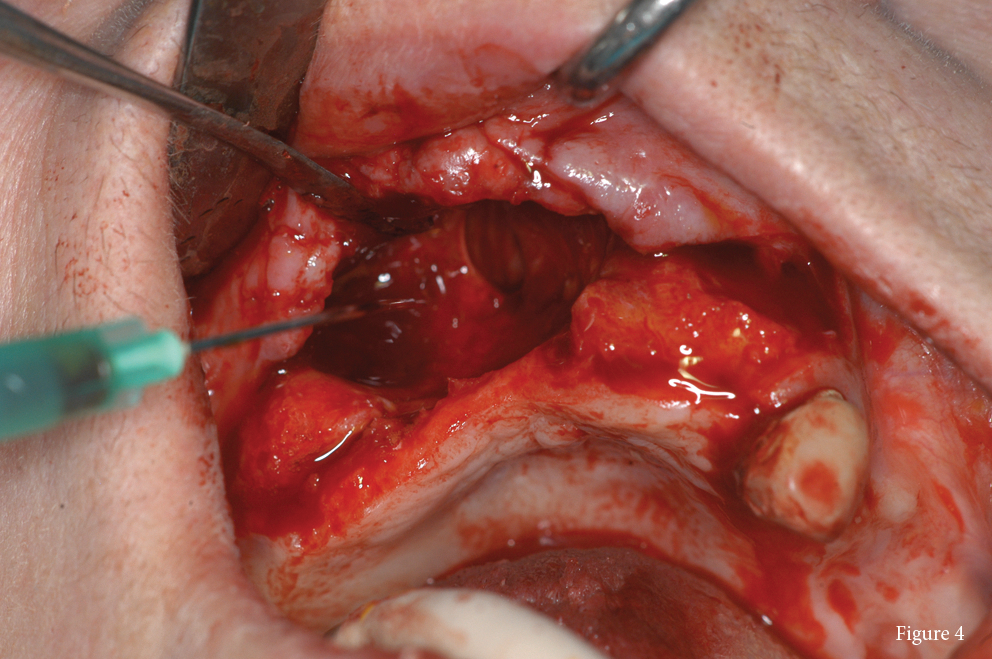
Intraoperative Nd:YAG laser biostimulation of the surgical site.
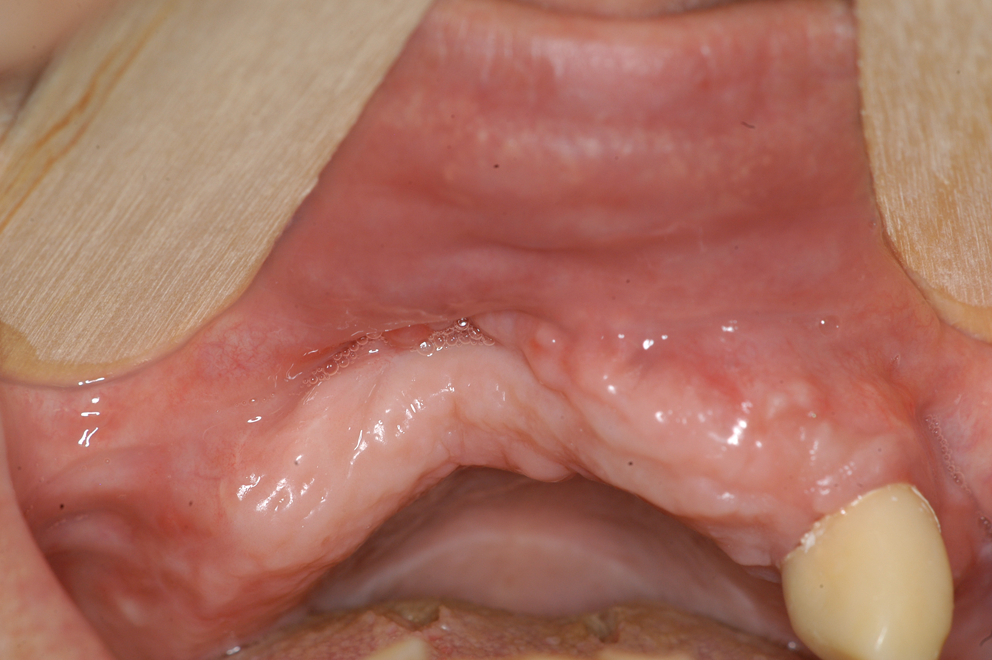
Complete healing of patient 6 months after surgery.
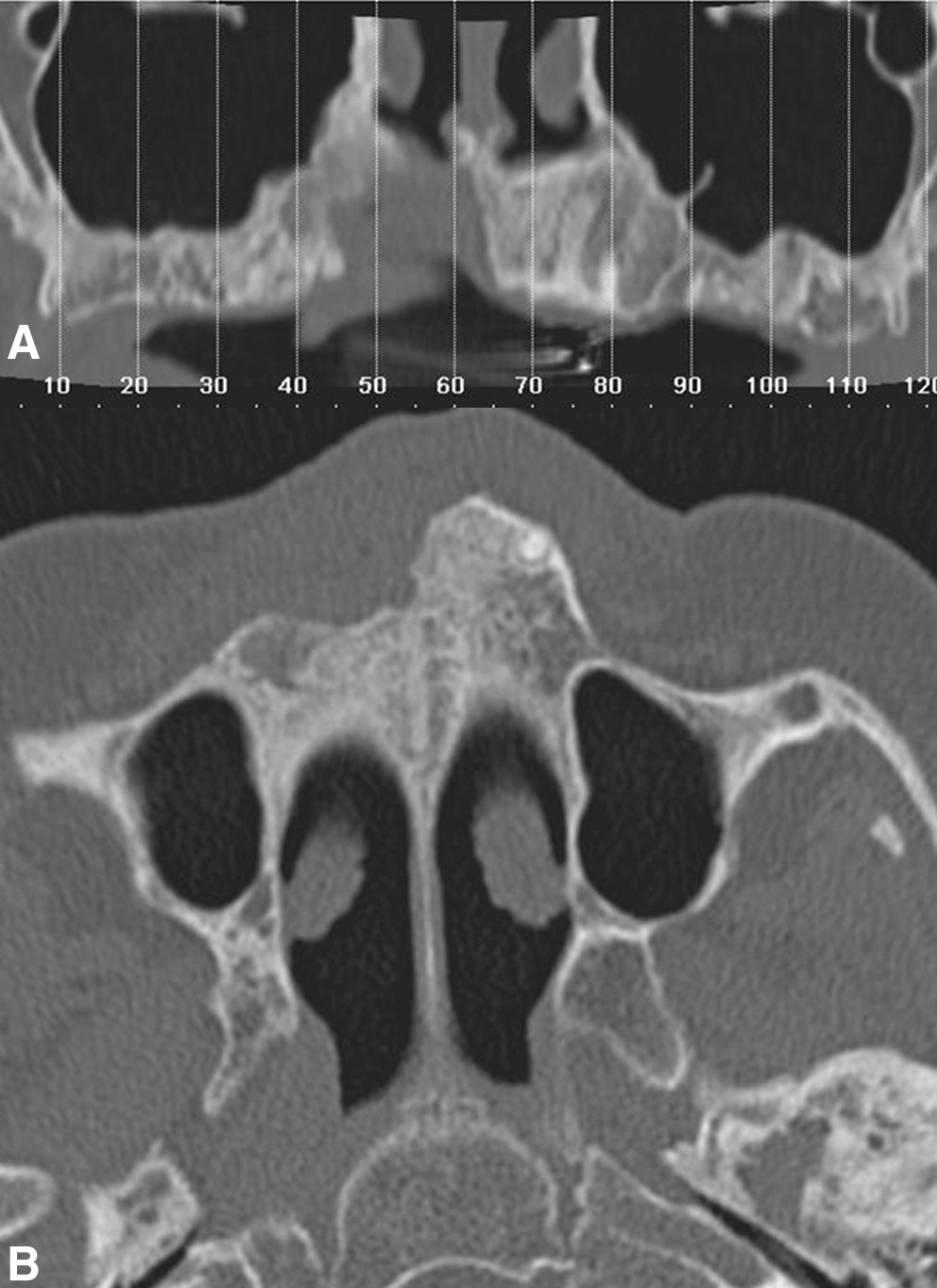
CT images showing the improvement and the healing of the maxillary sinus after BRONJ treatment.
Oral mucosa incisions were performed with cold blade scalpels or Nd:YAG/Er:YAG lasers. Surgical removal of necrotic and peripherical bone was achieved in most cases by rotary cutting instruments or, in a small number, by intervention with Er:YAG laser. Bone resection or vaporization of the necrotic areas was obtained with variable parameters, from 250 mJ 20 Hz Very Short Pulse (VSP) with a fluence of 50 J/cm2 up to 300 mJ, 30 Hz with a fluence of 60 J/cm2. During the surgical intervention we used an iodopovidone solution as irrigation; Er:YAG laser device has been used with a distilled water irrigation system.
Because of the risk of relapses of BRONJ, clinical result is the only possible evaluation; histopathological control is recommended only in case suspicious for metastatic lesion. A decrease in patient signs and symptoms is a reliable and objective parameter of clinical success. In order to define clinical parameters that could be used to evaluate the results obtained with the different therapeutic strategies reported previously, we have already introduced 46 what we call “clinical success”. This is identified as a treatment able to give a positive result (at least in terms of patient quality of life): (1) complete mucosal healing (classified as stage “0”) or (2) transition from a higher to a lower stage of BRONJ site according to Ruggiero's system (healing improvement). Both clinical results had to be maintained over at least 6 months. These two levels of clinical improvement were then used in this study to record the results obtained from the four treatment groups retrospectively evaluated (Table 3).
Statistical analysis
Statistical analysis was performed using the Fisher test, and results were considered statistically significant for p<0.05.
Results
Improvement (in terms of transition from a higher to a lower stage for at least 6 months) was recorded in 3 out of the 12 (25%) BRONJ sites treated with medical therapy only (G1) with a transition to stage 0 for 2 sites (16.6%) and a mean follow-up of 7.5±2.06 months (range, 6–12). For 18 out of the 27 (66.6%) lesions treated in G2, an improvement was observed. Of note, 9 of these improved BRONJ sites (33.3%) had a permanent transition to stage 0 with a mean follow-up of 11.55±7.12 months (range, 6–26). For G3, 9 sites (52.9%) had a permanent transition to stage 0, with a mean follow-up of 9.47±5.34 months (range, 6–24) (Table 3). Finally, in G4, an improvement of 40/45 (88.8%) BRONJ lesions was recorded. Moreover, 33/45 (73.3%) had a permanent transition to stage 0, whereas the other 7/45 (15.5%) had a transition to lower stages, in comparison to that recorded at the time of first clinical evaluation. The mean follow-up in this group was 16.44±10.95 months (range 6–54) (Table 3).
A statistically significant result was recorded from the comparison of the BRONJ sites treated with antibiotic therapy alone (G1) when compared to those treated with local LLLT applications (G2) (p=0.0346). In addition, the BRONJ lesions treated with a surgical approach and LLLT applications (G4) were statistically characterized by healing improvement in comparison to those treated in the other groups (G1-G2-G3; p<0.05).
In order to analyze the results obtained with a medical (G1 + G2) versus a surgical approach (G3 + G4), we compared the results obtained in terms of complete healing and clinical improvement. Higher levels of both complete healing (level A: p=0.0003) and clinical improvement (level B: p=0.0003) (Table 4). Furthermore, a similar comparison was performed with the results obtained with non-laser-assisted (G1+G3) versus laser-assisted (G2+G4) therapy. Although no statistical differences were recorded in these two groups in terms of complete healing, a higher level of clinical improvement (level B) was recorded using a laser-assisted approach (p=0.0003) (Table 4).
Healing: Complete mucosal healing without signs of infection or pain for at least 6 months (level A).
Improvement: Passage from a higher to a lower stage of the disease (level B).
None of the results obtained appeared to be influenced by the site of the lesions (mandible or maxilla involvement) (p=0.28) or underlying pathology such as MM, BM, or OP (p=0.088). However, fewer BRONJ sites classified as stage III underwent clinical improvement (p=0.0007) (Table 5).
Healing improvement: BRONJ sites after medical or surgical treatments (with or without LLLT) that progressed to both level A and/or level B.
Considering all the BRONJ sites for which an improvement was recorded compared to those treated but without clinical success, no significant influence between discontinuation of BP therapy and healing improvement was recorded (p=0.4656), nor was there any influence in terms of different underlying diseases (p=0.08726) (Table 5).
Finally, no statistically significant correlation was identified between smoking habits, type of treatment, and lesion improvement (p=0.9027).
Discussion
The analysis of the data reported in the present study showed that medical therapy alone induced only a slight improvement in symptoms and signs of BRONJ (3/12; 25%; Table 3). Antibiotic treatment can usually limit the signs and symptoms of acute inflammation caused by infection for a short period (usually 3–4 weeks) with a subsequent relapse. On the contrary, the surgical approach is associated with a significant improvement of the clinical aspect in the present study (Level A, p=0.0002–Level B p=0.014).
The best results in terms of number of BRONJ sites with clinical healing and duration of effects of therapy were obtained with the combination of antibiotic therapy, conservative surgery (including the use of Er:YAG), and LLLT. In addition, only a slight difference could be noted between the results obtained with surgery alone (52.9%) and those obtained with antibiotics and LLLT applications (33.3% level A, 66.6% level B). This observation suggests that the application of LLLT can be useful, especially for medically compromised patients who cannot be treated surgically. As recently reported, 46,47 LLLT gives an helpful advantage in terms of stimulation of bone cell proliferation and differentiation and vascularization.
Variables such as BPT discontinuation, maxillary or mandibular localization of lesions, and patient pathology were not related to treatment outcome in the present study.
It is important to note that no cases staged as III had a clinical improvement after any treatment. This result confirms that early stages of BRONJ (with minimal bone exposure) can benefit from both medical and conservative surgical strategies.
In our experience, better results were obtained with the surgical approach than the medical therapy, and this observation could be linked with other published ones. 44 Minimally invasive surgery, performed with the patient under local anaesthesia (at a day hospital) in the early stages of the disease may effect a complete mucosal healing.
In a recent review, Migliorati and colleagues reported percentages of complete healing variable from 17.3 to 17.6% for medical therapy or surgical debridement to 46.3% for free flap or surgical resection procedures, 47 with mucosal healing in 56.2% and bone healing in 5.9% of patients. In the present study, the group treated with a laser-assisted surgical approach (G4) achieved complete mucosal healing in 73.3% of cases.
Conclusions
The BRONJ staging system first proposed in 2007 8 and recently updated in 2009, 9 is currently being used in different studies as the reference system for the classification and treatment of this disease (Table 1).
However, different studies have reported that late surgical management of BRONJ can induce a progression of the disease from the initial to later stages. 9,10,15,39,48 –52 In addition, as already reported, we should not forget that patients with this condition (often affected by neoplasias) undergo chemotherapy, are debilitated by their malignancy, and are therefore not able to bear the side effects of prolonged (and sometimes permanent) therapeutic antibiotic schedules. 15,39,49 LLLT induces an improvement of oral soft and hard tissue healing process.
In light of these considerations, we analyzed the surgical and nonsurgical treatment and Nd:YAG laser applications of 101 BRONJ sites. Clinical results were evaluated by two levels of success: complete mucosal healing (level A) and improvement of signs and symptoms (level B) for a follow-up from 6 to 54 months (average 16 months). 39
Minimally invasive surgery, performed with the patient under local anaesthesia (at a day day hospital), may effect a complete mucosal healing by reducing the microbial superinfection of soft tissues. In addition, LLLT applications may stimulate the regeneration and angiogenesis of soft tissues, increasing the speeding up of the healing process.
In conclusion, from our experience, it is possible to observe that an early conservative surgical approach, associated with LLLT, could be considered a reliable treatment in comparison to medical therapy alone.
Footnotes
Author Disclosure Statement
No competing financial interests exist.