
Abstract
Introduction
Current treatment of amblyopia involves optimal correction of refractory anomalies followed by occlusion of the leading eye or penalization. 3 -5 Generally, vision can be improved in children only up to the age of 9 years. If therapy starts later, full visual acuity and binocularity can be achieved only in rare cases. In adult patients, treatment of amblyopia can only aim at improving the quality of life, for example, by eliminating any work-related disadvantages. Various therapeutic approaches have been tested in adult patients but without long-term success.
Here, we present first evidence that low-level laser therapy (LLLT) may improve visual acuity in adolescent and adult patients with ametropic or strabismic amblyopia.
Materials and Methods
Study design and patients
This single-blinded, placebo-controlled, interventional, noninvasive study was conducted in accordance with the Helsinki Declaration. Written informed consent was obtained from all patients before enrollment. Data were collected during a 7-year period (maximal follow-up of 13 years) and retrospectively evaluated.
Patients ≥12 years of age with ametropic or strabismic amblyopia were included if they presented with a distant visual acuity of ≤20/30 Snellen after optimal correction. Patients were excluded if they had other concomitant eye or other systemic diseases that could impair vision.
Laser treatment
A continuous wave (cw)-type semi-conductor laser diode (780 nm) mounted with collimating optics (round laser spot area at 1 cm distance: 3 mm2) in a handheld casing, was used for LLLT. The laser was driven by an apparatus that provided low-frequency switching of the laser beam (292 Hz, 1:1 duty cycle) and automatic control of 7.5 mW average output power (Bimed, Munich, Germany). The average laser output was measured before each treatment using an external laser power output meter (Laser components GmbH, Groebenzell, Germany). The effective minimal laser power of 7.5 mW had been determined previously. 6
Laser irradiation was applied to the macula by guiding the beam of the laser diode at 1 cm distance above the eyeball while the eye was maintained in adduction. If necessary, eyelids were manually fixed. Each treatment took 30 sec with a dose of 0.22 J/cm2. Three to four (mean 3.5) treatments were performed during 2 weeks (mean total dose of 0.77 J/cm2).
Twenty patients (20 eyes) were randomly selected to receive mock treatment (control group); the laser beam was directed above the nose without contacting the eye. An acoustical signal after every 10 sec was perceived as treatment by the patients.
Ophthalmological examinations
A biomicroscopical and ophthalmoscopical examination was conducted at study inclusion (baseline), before each treatment, and at the end of the study. These examinations were performed under comparable conditions with respect to time of examination and examiner. Best corrected distant visual acuity was assessed by projection of Snellen optotypes (American Optical, U.S.A.) at a 20-foot distance after optimal correction of refraction. Only unknown optotypes were presented to prevent patients from learning them. In a subgroup of 12 patients (12 eyes) we recorded an M-VEP (according to methodological guidelines available at
To assess treatment safety and tolerability, we examined patients' eyes before and after each treatment session, and asked patients about their general well-being by non-leading questions.
Data analysis
Data on visual acuity were transformed into logarithmic minimal angle resolution (log MAR). Data were analyzed retrospectively categorizing the results as no change, improvement, or worsening. A t test for paired samples was used to examine the statistical significance of changes after completion of LLLT compared to baseline.
Results
Demographic and baseline characteristics
We included 178 patients (75 women, 103 men) with a mean age of 46.8 years (range: 13–72 years) in the study. Thirteen out of these 178 patients were adolescents, that is, 13–18 years old (6 women, 8 men). Two-hundred thirty-one eyes with amblyopia (118 right and 113 left eyes) were treated and evaluated. Amblyopia was caused by ametropia in 110/231 eyes and by strabismus in 121/231 eyes. In 53 patients amblyopia affected both eyes. The control group included 20 patients (14 women, 6 men) with a mean age of 38.6 years (range: 18–64 years) and 20 eyes with amblyopia caused by ametropia (n=10) and strabismus (n=10).
Visual acuity
LLLT improved best corrected distant visual acuity in 100/110 eyes with ametropic amblyopia (91%; p<0.001). Visual acuity increased by 1, 2, 3, 4, 5, 6, and 7 rows in 6%, 28%, 23%, 14%, 13%, 4%, and 3% of the eyes, respectively. In 10 eyes (9%) visual acuity remained unchanged (Table 1).
Best corrected distant visual acuity was measured at a distance of 20 feet using American Optical Snellen optotypes. The change in visual acuity is presented in terms of logarithmic minimal angle resolution (log MAR).
In patients with strabismic amblyopia, visual acuity improved in 107/121 eyes by one or more rows (89%; p<0.001). Visual acuity increased by 1, 2, 3, 4, 5, 6, and 7 rows in 20%, 15%, 19%, 16%, 14%, 3%, and 2% of eyes, respectively. In 14 eyes (11%) visual acuity remained stable (Table 2). No changes in the visual acuity were observed in the control group.
Best corrected distant visual acuity was measured at a distance of 20 feet using American Optical optotypes (Snellen). The change in visual acuity is presented in terms of logarithmic minimal angle resolution (log MAR).
Generally, the increase in visual acuity after LLLT tended to be faster and more pronounced in adolescent patients (aged ≤18 years) in comparison to adult patients (aged >18 years) with ametropic or strabismic amblyopia (data not shown).
One patient with ametropic and esotropic amblyopia was followed for 13 years. The visual acuity of the better eye was maintained at the level obtained after the initial LLLT (from 20/30 to 20/20), over a period of 10 years. The visual acuity of the strabismic (esotropic) eye had returned to the initial visual acuity of 20/100 but reached again a maximum of 20/25 after repeated treatments (Fig. 1).
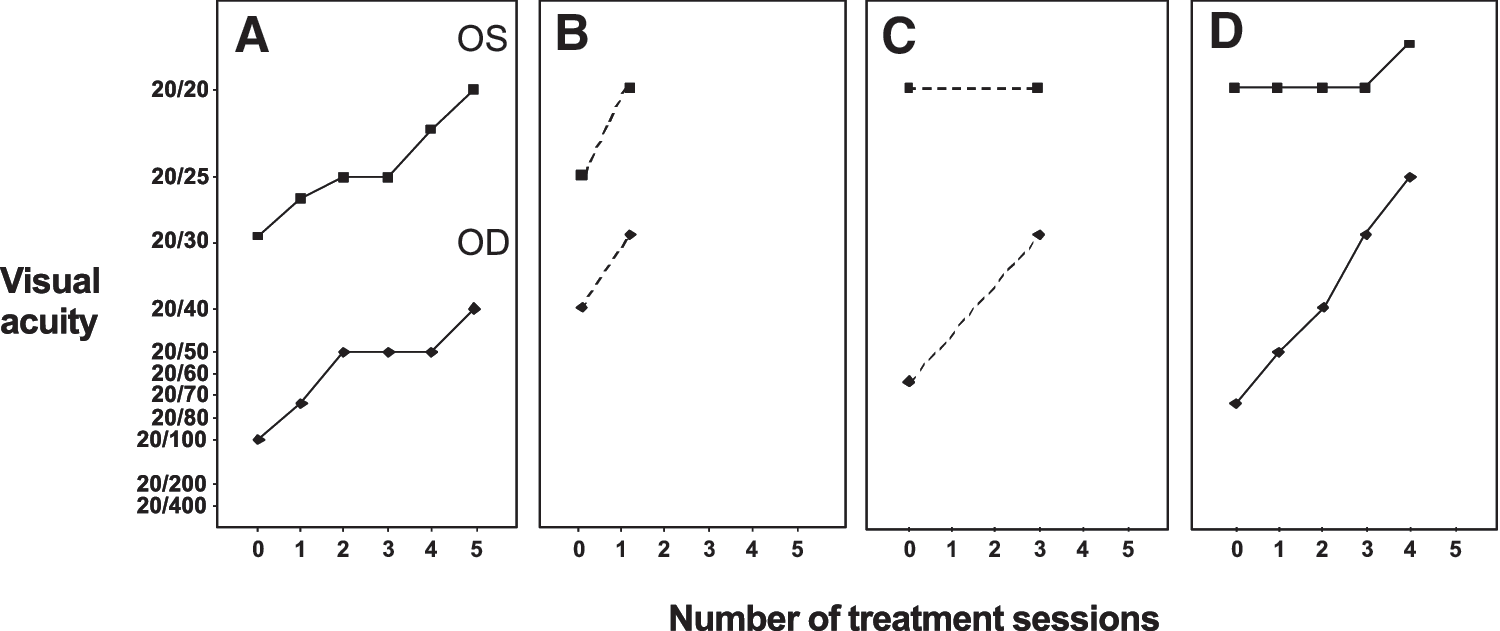
Long-term effects of low-level laser therapy in a patient with amblyopia. Measurements of best corrected distant visual acuity in a patient (aged 13 years at the beginning of therapy) with ametropic amblyopia (left eye, upper curve) and esotropic amblyopia (right eye, lower curve).
M-VEP
The amplitudes of the M-VEP recorded in 12 patients (12 eyes), ranged from 558 to 6543 nV and from 1471 to 6794 nV before and after LLLT, respectively. The mean amplitude increased by 1207 nV from 2412 nV at baseline to 3619 nV after LLLT (+50%; p<0.001). M-VEP latencies ranged from 116 to 195 msec (Table 3). A representative example of the change in M-VEP is shown in Fig. 2.

Multifocal visual evoked potential (M-VEP) before and after low-level laser therapy (LLLT) in a patient with strabismic amblyopia. LLLT (6 treatments) of the left eye (lower curve) in a 65-year old patient with strabismic amblyopia increased best corrected distant visual acuity from 20/70 to 20/30 and M-VEP amplitude by 1094 nV. No changes were noted for the untreated right eye (upper curve).
Safety and tolerability
Overall, LLLT was safe and well tolerated. There were neither local nor systemic adverse effects. No case of diplopia occurred. Ophthalmoscopic examinations revealed no visible morphological changes of the macula after LLLT.
Discussion
Amblyopia is a frequent cause of impaired vision, which can be successfully treated only in children. So far, there is no therapeutic option for adolescents or adults who have missed this critical time interval. We present here first evidence that LLLT may improve visual acuity even in these patients.
A statistically significant improvement in best corrected distant visual acuity was observed after LLLT in 90% of the eyes with amblyopia in adults. In some eyes, visual acuity even reached 20/20. The magnitude of the improvement appeared to correlate with baseline visual acuity. Patients with strabismic amblyopia who did not respond to LLLT (11%) had severe amblyopia with poor visual acuity (≤20/200) and eccentric fixation.
Additional treatments helped to regain the once initially achieved improvement in visual acuity in patients who experienced a recurrent loss of vision. We therefore suggest regular controls and, if necessary, repeated LLLT (at first every 3 months, then every year) to stabilize the initial improvement of visual acuity.
M-VEP revealed a statistically significant increase of the amplitude. This increase did not correlate with the functional improvements. This may be explained by the fact that the amplitude is subject to various influences, and is therefore less reliable than the latency. The shortening of the latency was slight and not statistically significant.
The exact mechanisms of the effects of LLLT are not elucidated. 7 Experimental studies found that laser light stimulated metabolic activities and cellular protein synthesis by increasing the synthesis of adenosine-3-phosphate. 8 Eyes with amblyopia may also benefit, similarly to eyes with age-related macular degeneration (AMD), 6 from the direct stimulation by laser light causing a hyperpolarisation. Such stimuli were shown to promote interneuronal communication and function, probably by synaptogenesis and formation of “spins”. 9
Conclusions
LLLT may improve best corrected distant visual acuity and amplitude of the M-VEP in adolescent and adult patients with ametropic and/or strabismic amblyopia. The rapid improvement of visual acuity is associated with fewer treatments and control examinations and is therefore very economic. LLLT is not destructive or painful, and can easily be applied in combination with other therapies, or even as prophylaxis to avoid the development of amblyopia. The short duration of LLLT and lack of occlusion or additional drug treatments is expected to positively affect patient compliance.
This explorative study was undertaken to gain first experiences in this new field. Future trials are required to compare and establish the optimal treatment modalities using randomized, controlled, and double-blinded study designs and an appropriate number of study subjects.
Footnotes
Author Disclosure Statement
No competing financial interests exist.