
Abstract
Introduction
The causes of tendon overuse involve both extrinsic and intrinsic factors. 5 Repetitive mechanical loading at submaximal level is the single most frequently reported extrinsic factor, and this explains why this condition is so prevalent among the athletic population. In addition to loading, intrinsic factors such as age, gender, weight, and anatomical or biomechanical variations 6 –9 have also been regarded as contributing factors to tendon overuse. However, these factors were regarded as secondary, because they seldom result in tendon pathologies by themselves. Their presence, however, together with repetitive mechanical loading, would increase the vulnerability of the tendons to degeneration.
The exact mechanism of how these factors combine to produce the initial tissue damage in tendons is not known. However, tendons are sensitive to loading and they will respond to change in loading and adapt to the new mechanical environment in a subtle manner. 10 Repetitive loading, with or without the presence of intrinsic risk factors, may produce the initial pathological changes in either the extracellular matrix or the cellular components of the tendon. These changes will be manifested as tendinosis in the clinical setting.
The management of tendinopathy usually involves conservative treatment with physical therapy, and the rehabilitation process often requires a long duration of 3–6 months for complete recovery, 11 Once this condition develops, the intensity of training for the athlete will need to be reduced, and the response to treatment of the degenerating tendons is often very slow, thus having a significant negative impact on the performance of the athlete.
Clinically, the management of tendinopathy with either a therapeutic laser or exercise have both been reported to result in positive outcomes in pain reduction and functional improvement in patients with this condition in either lateral elbow extensors or Achilles tendons. 12 –14 However, those studies were focused on the clinical and functional outcomes. There has not been a report on the basic science, such as the biomechanical strength of degenerating tendons managed with physiotherapeutic treatments.
Oliveira et al. 15 studied the morphology of traumatically injured calcaneous tendon treated with a therapeutic laser in rats. They found that 8 days after injury, the laser-treated tendons had comparable organization patterns of collagen fibers to those of the normal controls. The authors concluded that low-intensity laser therapy was effective in improving collagen fiber organization of repairing calcaneous tendon after traumatic partial lesion. This finding is in agreement with an earlier report that laser therapy could improve the ultrastructural collagen alignment and size of repairing ligament after cutting injury. 16 However, the effect of laser on tissue strength of degenerating tendons has not been reported.
In order to examine the tissue biomechanical responses of degenerated Achilles tendon to treatment, this study was conducted to examine the effects of a therapeutic laser and a passive stretching exercise program on the basic science of biomechanical properties of Achilles tendons with induced tendon overuse, in a rat model.
Methods
Twenty-five 3-month-old female Sprague-Dawley rats were used in this study. The Animal Ethics Review Committee of The Hong Kong Polytechnic University approved this study. The animals were randomly assigned into five groups as in Table 1.
Tendon overuse protocol
The animals in Groups 1 to 4 were subjected to an exercise program for inducing Achilles tendon overuse. The exercise program of this study followed a recently developed protocol by Ng 17 that involved an enforced bipedal downhill running on a rat treadmill (Duen Production BCPT-98, Hang Zhou, Zhejiang, China) at 20 m/min with a 20 degree decline slope modified from the eccentric loading model of Soslowsky 18 . In order to increase the loading on the hindlimbs, a bipedal running model was induced by suspending the trunk of the rats with a harness so that the forelimbs were lifted off and the rats had to sustain their body weight with their hindlimbs and run in a bipedal pattern. The rats exercised for 1 h per day, 7 days per week for 8 weeks.
Therapeutic laser treatment
Animals in the laser group (Group 1) received a transcutaneous therapeutic laser over the Achilles tendon of both legs. The treatment parameter was referenced to Ng and Fung. 19 The therapeutic laser was applied with a probe (Omega Laser System Ltd., West Sussex, Great Britain) that produced a gallium aluminum arsenide (GaAlAs) laser beam with a wavelength of 660 nm, an average output power of 8.8 mW, and pulsed at 10 kHz. The treatment was given transcutaneously over the Achilles tendon of both legs. The rat was restrained in a plastic cage with the treated leg exposed and stabilized by the researcher. The laser probe was held at 90 degrees over the mid-point of Achilles tendon and in direct contact with the skin throughout the treatment session. The average power output of the laser probe was calibrated with a power meter prior to the study to ensure consistency of the output. The duration of the laser treatment was applied for 50 sec; therefore, the total amount of energy delivered to the tissue was 0.44 J per treatment. Because the size of the laser probe hole was 0.13 cm2, the energy density was 3.4 J/cm2.
Passive stretching exercise
Animals in Group 2 received passive stretching to their Achilles tendons on both legs within 10 min after every exercise session. The researcher applied the passive stretching by keeping the knees of the rats in extension and the ankles in maximum dorsiflexion. The stretching force was maintained for 10 sec and repeated for 20 times on each leg. This stretching program was chosen according to the normal clinical protocol of stretching for tendons.
Animals in the combined treatment group (Group 3) received both therapeutic laser and passive stretching with the protocol similar to those of Group 1 and Group 2. The order of treatment for Group 3 was passive stretching first, then the laser. The animals in Group 4 served as the running controls without any treatment, and those in Group 5 served as the normal controls. The treatments were applied daily throughout the study; therefore, a total of 56 treatment sessions were given to the animals.
Biomechanical testing
All animals were killed on the first day of week 9. Both lower limbs were removed at the hip joint, stored in a plastic bag and kept in a freezer of −70°C for later biomechanical testing. At 6 h before testing, the leg specimens were retrieved from the freezer and allowed to thaw inside the plastic bag. Each specimen was carefully dissected by removing all the soft tissues at the ankle joint, leaving only the intramuscular tendinous fibers, Achilles tendon, and calcaneus intact. The intramuscular tendinous fibers were then secured between two plastic strips with quick-setting superglue (Aron Alpha, Toagosei Co. Ltd, Columbus, OH). Care was taken to prevent the glue from running down the tendon, and the specimens were kept moist with normal saline during the whole testing procedure.
The glued plastic strips and calcaneus were mounted on the cross-heads of a material testing machine (MTS Synergie 200, MTS System Corporation, Ivry sur Seine Cedex, France). An extensiometer (MTS model 634.12F-24, MTS System Corporation, Eden Prairie, MN) was attached to the margin of the cross-heads for measuring the local strain of the tendon. The room temperature was controlled at 25°C during the tests.
The specimen was pre-conditioned with 10 oscillation cycles of 2.5% strain at a 10 mm per min to minimize the effect of deep freezing on the tissue. 20 After pre-conditioning, the specimen was stretched to 2.5% strain and maintained for 5 min. The loads were recorded at 5 Hz throughout the test, and the percentage change in load represented the load-relaxation property.
Afterwards, the tendon was subjected to ultimate tensile failure testing at a strain rate of 500 mm per min with a data sampling rate of 50 Hz. 21 The maximum load before failure represents the ultimate tensile strength (UTS) and the gradient of the linear portion of the load-deformation curve represents the structural stiffness.
Statistical analyses
One-way analysis of variance (ANOVA) was used to analyze the load-relaxation, UTS, and structural stiffness, with group as the factor. Post-hoc least squared difference (LSD) test was used to further analyze the ANOVA results that were significant. The significance level for all statistical tests was set at 0.05.
Results
The ANOVA results revealed a significant difference in stiffness (p=0.01), whereas UTS difference was marginally insignificant (p=0.07) and load-relaxation difference was not significant among the five groups. Post-hoc LSD comparisons revealed that the mean stiffness of all the four groups was significantly lower than that of the “no exercise” control group (p=0.01) (Fig. 1). In view of the low p value of the UTS, post-hoc LSD comparisons were performed and the results revealed that neither Group 1 or 3 was different from Group 5, whereas Groups 1 and 5 were higher than Groups 2 and 4 (p=0.01) (Fig. 2).
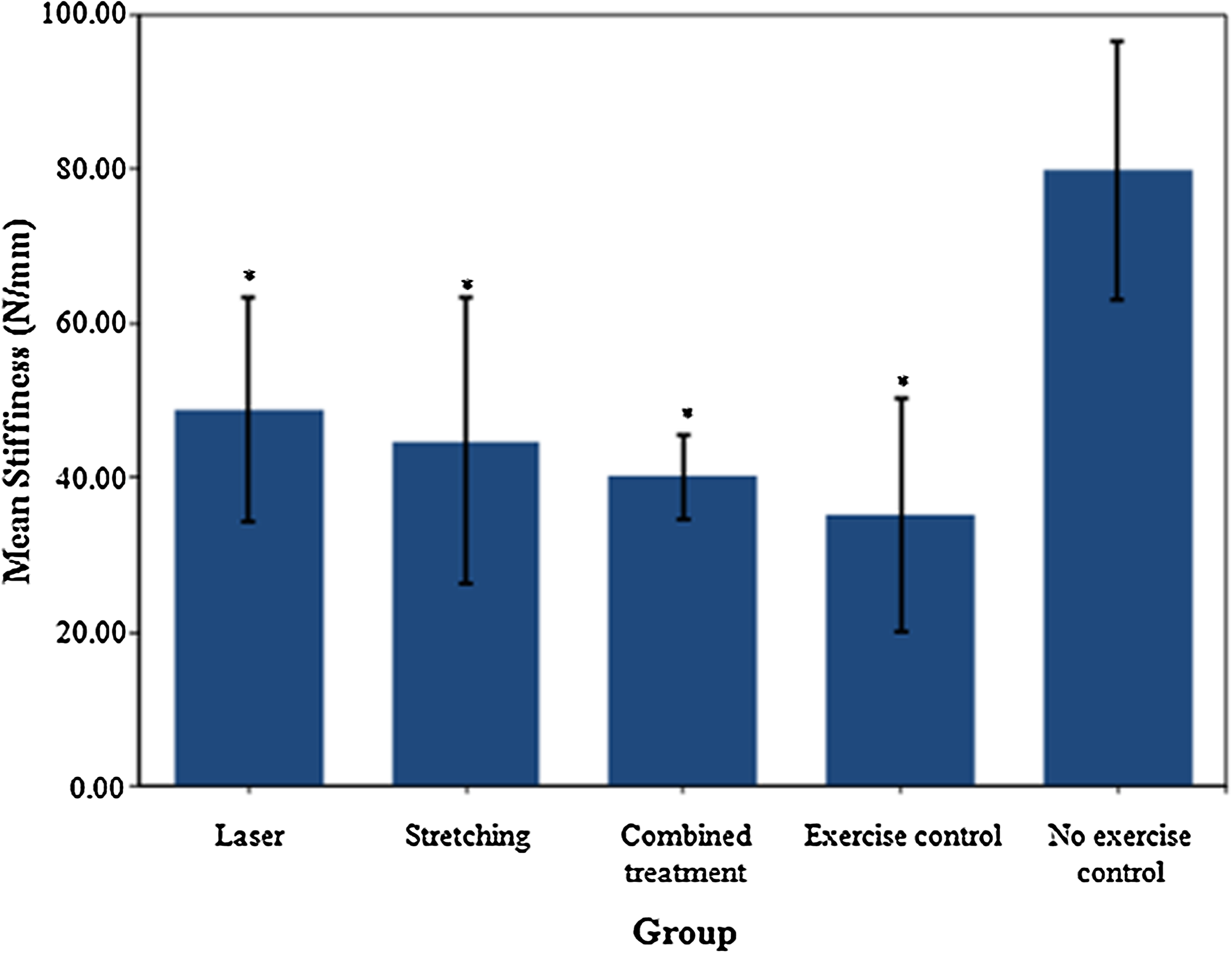
Means and standard deviations of the structural stiffness of the Achilles tendon for the groups. *Significant difference compared to the “no exercise” control group (p=0.01).
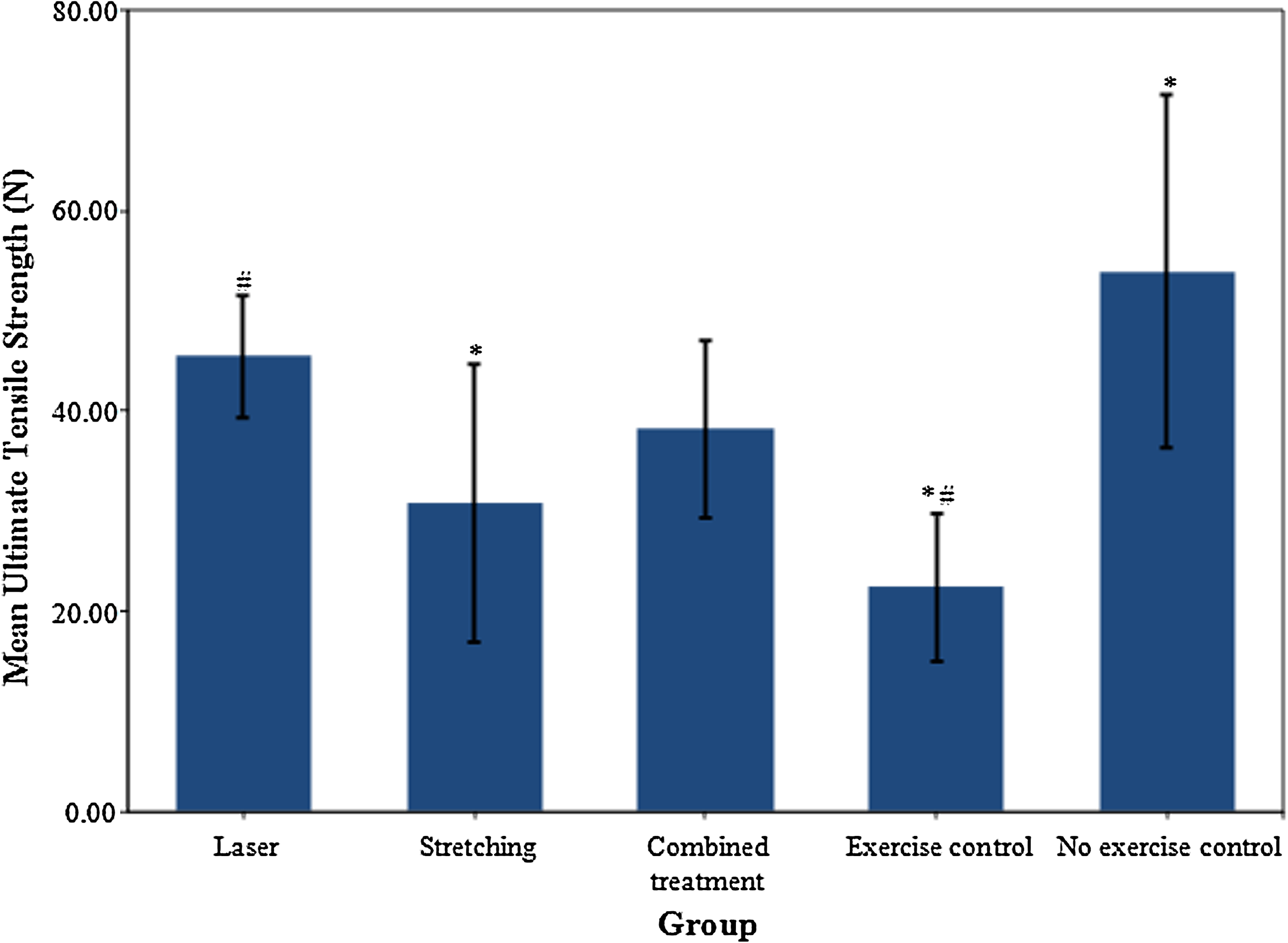
Means and standard deviations of the ultimate tensile strength of the Achilles tendons of the groups. # Strength for exercise control group was significantly lower than that of the laser group (p=0.01), *Strength for exercise control and passive stretching groups was lower than that of the “no exercise” control group (p=0.01).
Discussion
There have not been similar studies that investigated the treatment effect of a therapeutic laser and passive stretching on degenerating Achilles tendon in an animal model. The reason could be the lack of a suitable model of Achilles tendon overuse in animals. Very recently, Ng 17 has successfully developed an Achilles tendinosis model in rats using an 8-week enforced bipedal downhill running exercise protocol. The present study, by adopting this exercise protocol, has resulted in a significant decrease in mechanical strength in all the exercise groups, which formed the experimental basis for this study.
A natural phenomenon associated with repetitive submaximal loading in tendons is that the repeated loading may lead to micro-damage of the tissue. 22 Given that tendons, similarly to other connective tissues, are capable of repairing themselves when injured, the occasional micro-damage has little consequence when the tissue is given the time to recuperate. However, when the rate of damage exceeds that of the natural repair process, the damages start to accumulate, and it is believed that this accumulation of micro-damages can trigger the array of pathological changes seen in tendinosis. 5
Our results revealed that a therapeutic laser treatment and a combined program of a therapeutic laser together with passive stretching had improved the tensile strength of the overused rat Achilles tendons. The group that received the passive stretching exercise also showed an improved strength profile as compared to the “no treatment” running group, although it did not reach statistical significance.
The therapeutic laser parameter and dosage were chosen with reference to a previous study, which reported positive treatment results for tendons that had sustained transection injury in rats. 19 However, we acknowledge that because there was no other laser parameter used in this study, it cannot be concluded how this parameter compares with other laser parameters for treating this condition.
The ultimate tensile strength of the laser group was found to be significantly higher than the running control group, but the passive stretching group or the combined treatment group did not show this result. In addition, the results revealed no difference in ultimate tensile strength between Groups 1 and 5, but Group 1 had lower stiffness than Group 5. From a mechanical point of view, the decrease in tendon stiffness would render the tendons less efficient in sustaining the load at a given elongation, and the load not taken up by the tendons would be borne by other structures, thus resulting in overloading or pathological changes. Therefore, the present finding suggested that a laser treatment program might slow down the weakening of the degenerating tendon, but it could not stop the pathological changes from developing. Furthermore, the passive stretching either alone or in combination with laser treatment was not found to be effective for treating Achilles tendon overuse.
According to the biological timing of soft tissue healing, the new collagen fibrils would scatter in the extracellular matrix and start to aggregate into organized bundles by day 21 in response to external loading. 23 The resultant mechanical behavior of the tissue is dependent upon the quantity, geometrical size, and orientation of the collagen fibrils within the extracellular matrix. 24 In view of the normal timing of soft tissue healing, the present study had covered the period of active collagen synthesis and early remodeling, which would be important for determining the functional strength of the repaired tissues.
The mechanisms of improved tissue strength with the low-level laser therapy (LLLT) and stretching could be multi-factorial, such as overgrowth of the repairing tissue, improvement of the ultrastructural morphology, or tissue biochemistry. It has been reported that the mechanical strength of soft tissue correlates with the hydroxypyridinium (HP) crosslink density. 25 However, whether LLLT would improve the biochemistry profile of degenerated tendon is questionable, as it has been reported that the HP crosslinks had not increased in the healing tendon of rabbits after laser therapy. 26
The small number of animals in this study with large variance has limited the statistical power of this study. Future study with larger sample is needed for drawing a more conclusive result. In the present study, we have only examined the tissue's structural properties, it is not known if the material properties of the tendon have also improved. With an oversized tendon, it would acquire strong mechanical strength but it may not be functionally desirable because of risk of tenosynovitis. 27 It would be logical to examine the ultrastructural morphology of both the treated and untreated tendon tissues in the next phase so as to examine if this mode of treatment would enhance collagen fibril size or alignment within the extracellular matrix.
Conclusions
We conclude that a therapeutic laser program of 0.44 J might be able to slow down the decrease in strength of degenerating Achilles tendon, but it could not stop the pathological changes from developing. Other irradiation parameters should be investigated for this condition. The application of passive stretching either alone or in combination with a therapeutic laser is not effective in treating tendon overuse.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.