
Abstract
Introduction
Erbium:yttrium-aluminum-garnet (Er:YAG – 2940-nm wavelength) and neodymium:yttrium-aluminum-garnet (Nd:YAG – 1064-nm wavelength) lasers have demonstrated applicability in endodontics. 1,2 An alternative high-energy laser is the 980-nm diode laser, with low purchase and maintenance costs as well as greater versatility, because of its compact size. 3
The 980-nm diode laser transmits energy through thin flexible fibers, compatible with the dimensions and curved shapes of root canals. 3 –10 Diode laser wavelengths have good penetration potential, high absorption peaks in melanin and hemoglobin, and low interaction with water and hydroxyapatite. 5,6
The penetration capability of diode lasers (810–980 nm) is 10,000 times greater than that of Er:YAG, 11 and may reduce the number of microorganisms up to 500 μm in depth within the dentinal tubules. 3,6 Gutknecht et al. 3 reported a reduction of the microbial content in hard-to-reach areas, such as the dentinal tubules, after diode laser irradiation.
Morphological alterations in dentin irradiated with diode laser can be observed by scanning electron microscope, 5,8,10 and depend mainly on the parameters of the lasers such as output power, frequency, and application mode. This is because these parameters are directly related to the increase in temperature in the dental tissues. 7 Intracanal irradiation with 980-nm laser diode favors adhesion of epoxy resin based sealer, 12 and reduces apical leakage. 5
However, the results of these studies are not sufficient to confirm the effects of 980-nm diode laser on dentin. There are also few reports of the consequences of diode laser irradiation emitted at 980 nm on the mechanical properties of dentin. The purpose of this study was to evaluate the effect of irradiation with a 980-nm diode laser at 1.5 and 3.0 W on the microhardness of root dentin at depths of 30, 90, 150, and 300 μm, by varying the irrigant solution used during the biomechanical preparation.
Materials and Methods
This study was submitted and approved by the Ethics Committee of University of Ribeirão Preto, São Paulo, Brazil.
Human superior canines stored in 0.1% thymol solution at 4°C were washed in running water for 24 h to eliminate thymol residues. Teeth were examined under a 20×magnifier (Leica Microsystems, Wetzlar, Germany) to discard those with structural defects such as fissures and defective grooves. Seventy-two single-canal, human canines with complete root formation, no internal resorptions or calcifications, and no accentuated root curvatures were selected. The crowns were transversally sectioned at the cementoenamel junction, using a double-faced diamond disk (KG Sorensen, Barueri, SP, Brazil) at low speed (Kavo, Joinvile, SC, Brazil), standardizing the root length at 18 mm. The root canals were explored using a #15 K file, and the working length was determined to be 1 mm shorter than the standardized root length (17 mm).
The roots were randomly distributed among three groups according to the irrigant solution used during biomechanical preparation: distilled and deionized water (control); 1% NaOCl (pH 9.0); and, 1% NaOCl + 17% EDTA (pH 7.3).
Biomechanical preparation was performed using the K3 rotary system (SybronEndo, Orange, CA), powered by an electric motor (Endo Plus, Driller, São Paulo, SP, Brazil) at 350 rpm. The apical area was enlarged up to #50.02 file size. During this process, the root canals were irrigated with 2 mL of the irrigant solution selected for each group. The total time required to complete the biomechanical preparation was 20 min. In group treated with NaOCl + EDTA, 2 mL of EDTA solution was used as final irrigant for 5 min. All groups received a final flush with 10 mL of distilled water and were then dried with absorbent paper points (Dentsply Ind. e Com. Ltda., Petrópolis, RJ, Brazil).
The groups were subdivided into three subgroups (n=8) according to the laser parameter setting: A, no irradiation (control); B, 1.5 W/100 Hz; and C, 3.0 W/100 Hz. The laser unit used was the 980-nm diode laser (SIROLaser 2.2; Sirona Dental, Bensheim, Germany), with a 200-μm fiberoptic tip. The specimens were positioned in an adjustable acrylic device to hold them in a vertical position, and the root canals were filled with distilled and deionized water. The fiberoptic tip was introduced up to the apical region; the laser was activated and gently withdrawn from the root canal to the coronary region in using helicoidal movements, and was reintroduced into the apex for a total laser irradiation cycle of 20 sec. This irradiation cycle was performed only once in each root canal. The laser parameters were confirmed through the calibration system of the laser device, after the irradiation of each subgroup. Two millimeters of the fiberoptic tip were cut off after the irradiation of each subgroup to avoid energy loss.
The specimens were individually placed on a precision cutting machine (Isomet1000; Buehler, Lake Forest, IL), with a water-cooled diamond saw (South Bay Technology, San Clement, CA). They were sectioned perpendicularly to the long axis, resulting in eight slices of 2.5 mm thickness. The coronal surface of the root sections, corresponding to the middle third, were polished using silicon carbide papers (Norton, Lorena, SP, Brazil) of decreasing abrasiveness (from #400 to #1200 grit) and finished with aluminum oxide paste. Specimens were fixed with wax into a circular acrylic base.
Knoop microhardness (KHN) values were obtained using a Shimadzu HMV2 hardness tester (Newage Testing Instruments Inc., Southampom, PA), with a static load of 25 g for 10 sec in dentin, at depths of 30, 90, 150, and 300 μm from the canal lumen. At each dentin depth, the microhardness test was performed in triplicate, and the means were submitted to ANOVA and Tukey–Kramer post-hoc tests at a 0.05 significance level. Details of the methodology are shown in Fig. 1.
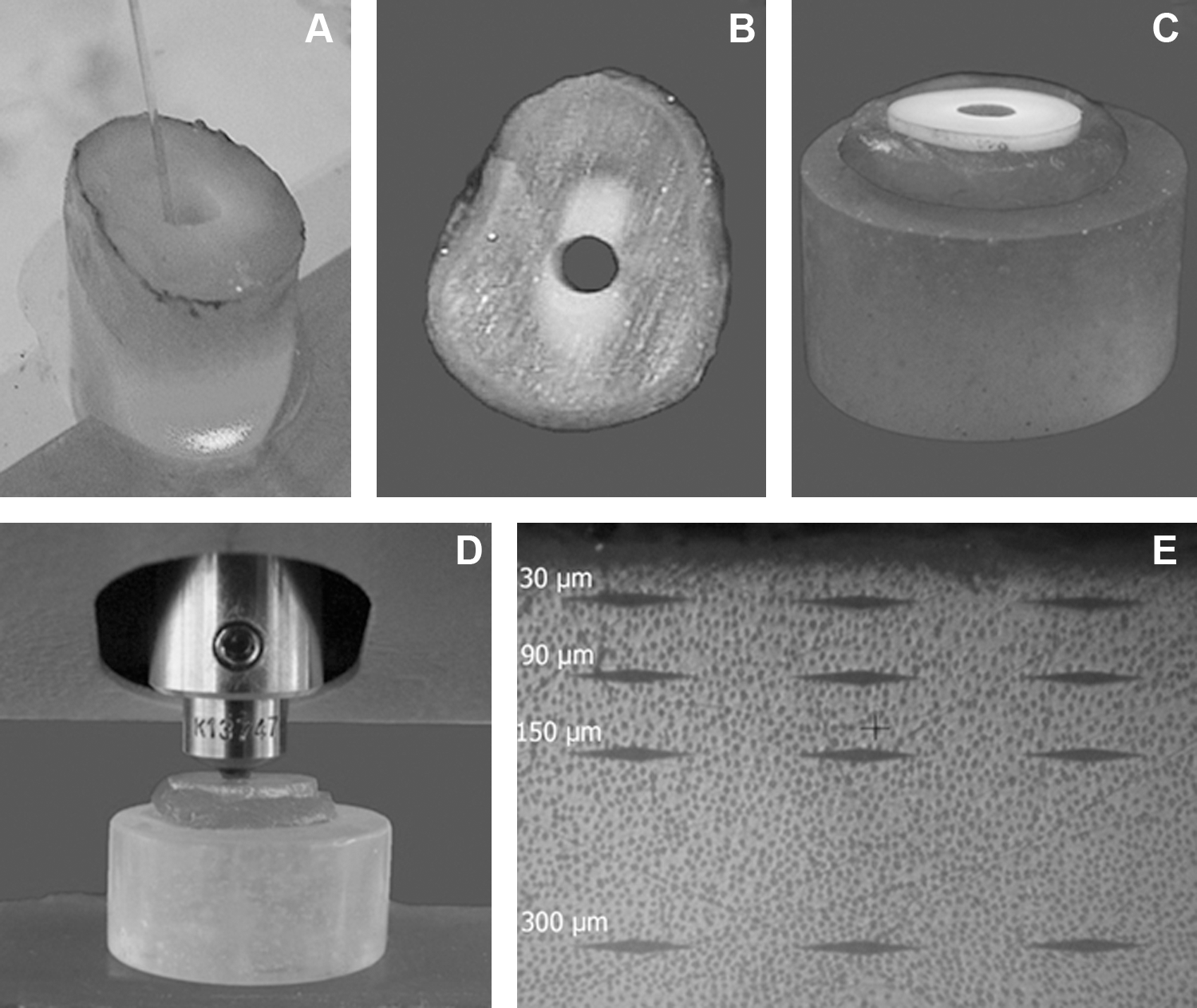
(
Results
The microhardness (KHN) values obtained from the dentin, at depths of 30, 90, 150, and 300 μm after treatment with different irrigant solutions and laser parameters are shown in Fig. 2.
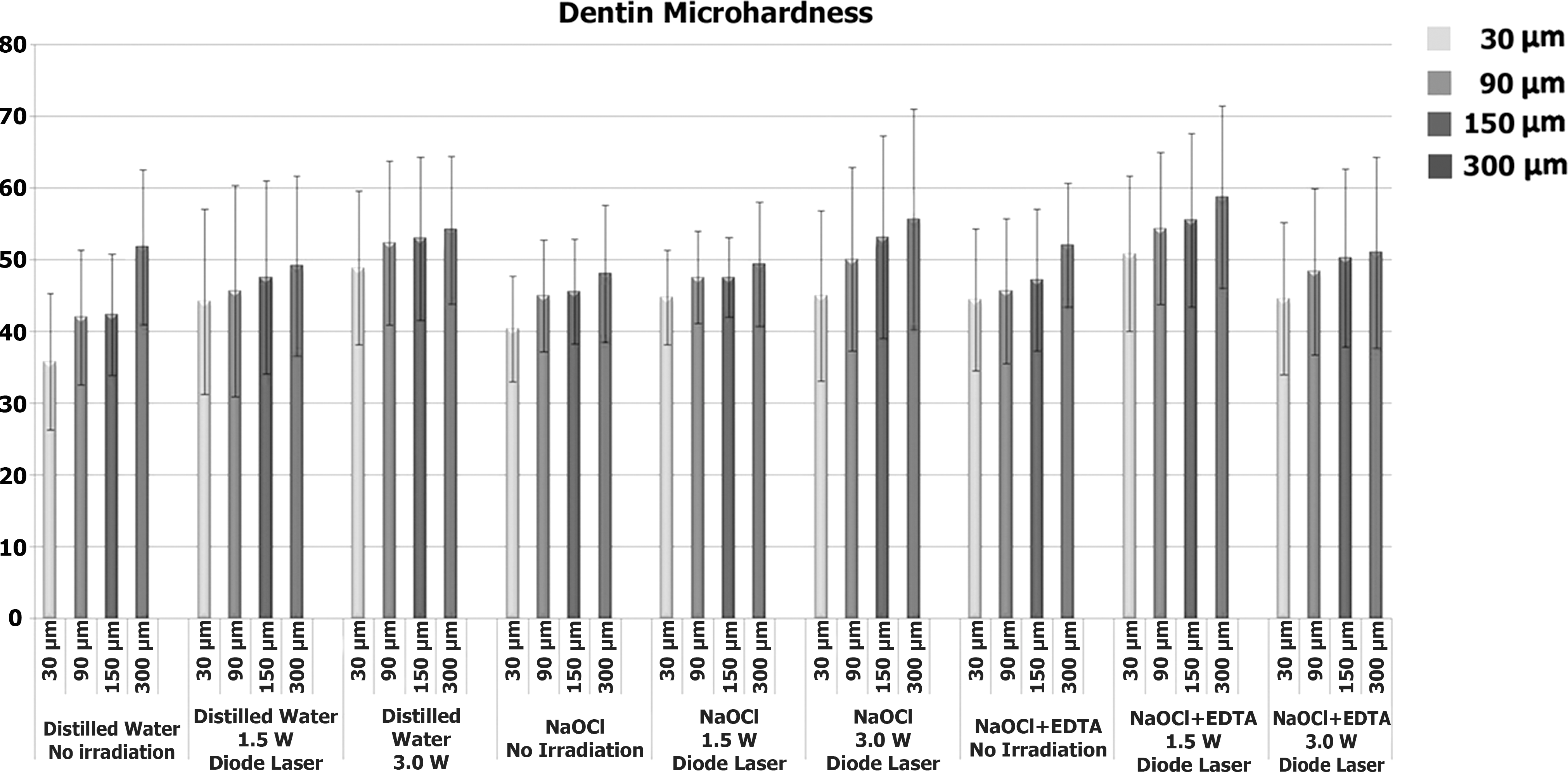
Microhardness (KHN) obtained from the dentin at different depths, after treatment with irrigant solutions and diode laser.
ANOVA showed significant statistical differences for the factors laser parameter, dentin depth, and interaction between irrigant solution and dentin depth (p<0.05). No differences were found among the irrigant solutions (p>0.05).
The Tukey–Kramer test ascertained that the groups irradiated with 1.5 and 3.0 W/100 Hz were statistically similar (p>0.05), and that they were different (p<0.05) from the non-irradiated group (p<0.05) (Table 1). The highest microhardness values were obtained at depths of 150 and 300 μm, which were statistically similar (p>0.05); and, they were different (p<0.05) from the values obtained at the depth of 30 μm. Intermediate values (p>0.05) were observed at the depth of 90 μm (Table 2).
Same letters indicate statistical similarity (p<0.05). Tukey critical value: 3.66.
Same letters indicate statistical similarity (p<0.05). Tukey critical value: 4.69.
Considering the interaction between irrigant solution and dentin depth, the highest microhardness values were obtained with NaOCl associated with EDTA at 300 μm. These were statistically different (p<0.05) from the groups irrigated with NaOCl or distilled water at 30 μm (p>0.05). The other groups showed intermediated values (p>0.05) (Table 3).
Same symbols indicate statistical similarity (p<0.05). Tukey critical value: 10.35.
Discussion
Laser systems located in the range of 810–980 nm wavelengths, near the infrared region, have been intensive studied in recent years because of the enhanced effectiveness of laser light deep within the infected root canal walls, as compared to chemical solutions; and, this fact justifies the incorporation of this technology into the endodontic arsenal. 3,13 The consequences of the interaction between laser light and dental tissues are not well documented, and can vary according to the selected parameters. The intrinsic properties of the dentin can also be affected by laser irradiation. This study evaluated the effects of the 980-nm diode laser on dentin microhardness, after using different irrigant solutions, by applying a non-destructive mechanical test.
In the present study, the microhardness values of the groups irradiated with 1.5 and 3.0 W/100 Hz were different from those of the non-irradiated group. This can be attributed to the thermal effect caused by laser energy, which changes the dentin structure. 9,10,14,15 The action mechanism of the 980-nm diode laser is likely to be similar to that of the 1064-nm Nd:YAG laser, because both are located in the near-infrared region of the electromagnetic spectrum. 11 In these wavelength bands, some energy is absorbed by dentin mineral content, such as carbonate and phosphate, resulting in crystalline arrangement and melting. 10
Diode lasers could cause damage to the root surface, and some of its effects have not yet been completely determined, making it relevant to determine parameters in vitro before using it in clinical practice. The parameters of this study were selected based on the study of Alfredo et al. 7 These authors verified that the application of 980-nm diode laser in root canal, for 20 sec, at 1.5 and 3.0 W with 100 Hz did not result in temperature rises >10°C 16 , which makes it feasible to use safely in endodontic therapy.
In this study, no differences were found in microhardness when comparing the laser parameters (1.5 and 3.0 W/100 Hz), which means that the small increase in output power was not sufficient to provide significant changes in the dentin.
Regarding the different dentin depths, there was an increase in microhardness from the root canal lumen toward the outer root surface. This finding can be easily understood when evaluating the specimens that were not submitted to laser irradiation (control group). In this group, the dentin microhardness was lower in the area surrounding the pulp, probably because of the intertubular matrix of this area. 17,18 Furthermore, there is a positive correlation between microhardness and tubular density. This means that the diameter of the dentin tubules increases toward the pulp, whereas microhardness decreases in this direction. 19 Likewise, the laser-irradiated specimens showed an increase in dentin microhardness regardless of laser power, and higher values were observed in the deeper regions of the dentin (150 and 300 μm).
Laser systems located in the range of 810–980 nm wavelengths, near the infrared region of the electromagnetic spectrum (diode and Nd:YAG lasers), have low absorption coefficients in water and hydroxyapatite; and, both systems allow propagation, scattering, and diffusion of the laser energy through the dentin tubules. 3,6,12 On the other hand, Er:YAG lasers have lower penetration ability in dental tissue, because of their high absorption coefficients in water and hydroxyapatite; therefore, this laser interacts mainly with the superficial layers of the dentin and promotes changes in microhardness up to 60 μm. 15,20
The chemical solutions used during root canal preparation did not affect the microhardness of the dentin. Although some studies indicate that dentin microhardness tends to decrease after using NaOCl and EDTA, the results can vary according to the methodology. 21,22 Other aspects to be considered are the concentration, pH, and action time of the NaOCl, because these factors are related to the collagen-protein denaturation of dentin. 23,24 In this study, the NaOCl solution had a low concentration (1%) and was in contact with the dentin only during biomechanical preparation (20 min). The EDTA solution did not decrease the dentin microhardness at any depth. This is probably because it has superficial chelating action of calcium ions, mainly in the first minutes, and this action is limited by the accumulation of an organic substrate over the dentin. 25 Probably, if the EDTA solution had been used alternatingly with the NaOCl, the effects on dentin microhardness would have been intensified. 26 Marchesan et al. 8 demonstrated that dentin permeability after 980 nm diode laser irradiation was directly related to the solution used for final irrigation.
Considering the interaction of dentin depth and irrigant solution, higher values were found for dentin treated with NaOCl and water, both at 30 μm. The differences could be attributed to the morphological variations of dentin substrate within groups, and could affect the results. 9
According to the results of this study, and based on recent research done with the 980-nm diode laser, it is important to emphasize that this laser system has endodontic applicability. However, further studies should be conducted to establish optimal laser parameters for intracanal application, as well as the effect of laser energy on the mechanical properties of dental substrates. In addition, it is necessary to develop fibers that allow better transmission of laser energy onto the root canal walls, thus avoiding damage to the supporting periodontal tissues.
Conclusions
Considering the limitations of a laboratory study, it may be concluded that dentin microhardness increased after 980-nm diode laser irradiation in the deeper regions of the dentin (150 and 300 μm), regardless of the irrigant solution used during biomechanical preparation.
Footnotes
Author Disclosure Statement
No competing financial interests exist