
Abstract
Introduction
In literature, several authors have reported that the most popular lasers used in neurosurgery (CO2 and Nd:YAG) induce histological effects both on brain and tumor tissues (histological alterations, thermal effect, and depth of action were studied). 8,10 –13 Yamagami et al. evaluated the effect of a Nd:YAG laser on different tumors (four meningiomas, one astrocytoma, and two mixed tumors). These authors found the following histological changes: one carbonized and vaporized layer, one vacuolated layer, one tiny necrotic layer, and one layer of tissue edema. 11 In 2010, Ryan et al. studied the action of a CO2 laser on swine brain tissue and compared it with bipolar cautery and with scalpel incisions without cautery. 9
The thulium laser has recently been introduced in surgical practice. 4 –6,14 –17 It was mainly used in urological surgery for vaporesection of the prostate and for bladder neck incisions. 14 –19 In neurosurgery, it was used mainly for third ventriculostomy. 20 Its wavelength is selectively absorbed by water, which is present everywhere in the human body; this feature allows it to vaporize and coagulate small vessels. 18 In an aqueous medium, the laser's effect is limited to tissues located <2 mm before the tip of the fiber; any tissue further than 2 mm from the tip is shielded by the water medium. The thulium laser is conveyed through a flexible optical fiber of <1 mm in diameter; it can be used in pulsed or continuous wave settings and with different power settings and exposure times. 21,22 The 2-μm thulium laser is an attractive option for use in micro- and endoscopic neurosurgeries.
The aim of this study was to evaluate the effects of a 2-μm thulium laser on meningiomas as compared with bipolar cautery and an ultrasonic aspirator.
Methods
Nine patients with a diagnosis of meningioma were enrolled in this study. The median age was 54 years, and there was a predominance of females (seven females vs. two males). Five patients had a histological diagnosis of meningothelial meningioma (World Health Organization [WHO] grade I). One patient had a diagnosis of fibrous meningioma (WHO grade I). Two patients had an atypical meningioma (WHO grade II), and one patient had a diagnosis of anaplastic meningioma (WHO grade III). All meningiomas were supratentorial and suitable for “en bloc” resection (Table 1).
All patients were treated with surgical resection. One tumor specimen, at least 3 cm in diameter, was obtained from each tissue sample. Immediately after surgical removal, the specimen was divided into four slices, each ∼7 mm thick. The slices were marked with stitches. An incision of 1.5 cm was made on each slice using these different settings: • Slice 1: linear incision with a 2-μm thulium laser (RevoLix® jr; Katlemburg-Lindau; Germany), 10 sec of exposition, continuous and no touch modality: ○ Power, 12 W; 100 J administered • Slice 2: linear incision with a 2-μm thulium laser (RevoLix® jr), 30 sec of exposition, continuous and no touch modality: ○ Power, 6 W; 206 J administered • Slice 3: linear incision with bipolar forceps (AESCULAP GN 300 BipoJet®, Melsungen; Germany) set at 20% power. • Slice 4: linear incision with ultrasonic aspirator (Sonopet Striker Model UST-2001®, MI) set at 50% power.
The incisions were then marked with ink. Samples were fixed with 10% formalin, embedded in paraffin, and then stained with hematoxylin and eosin. They were then observed by a pathologist and two neurosurgeons.
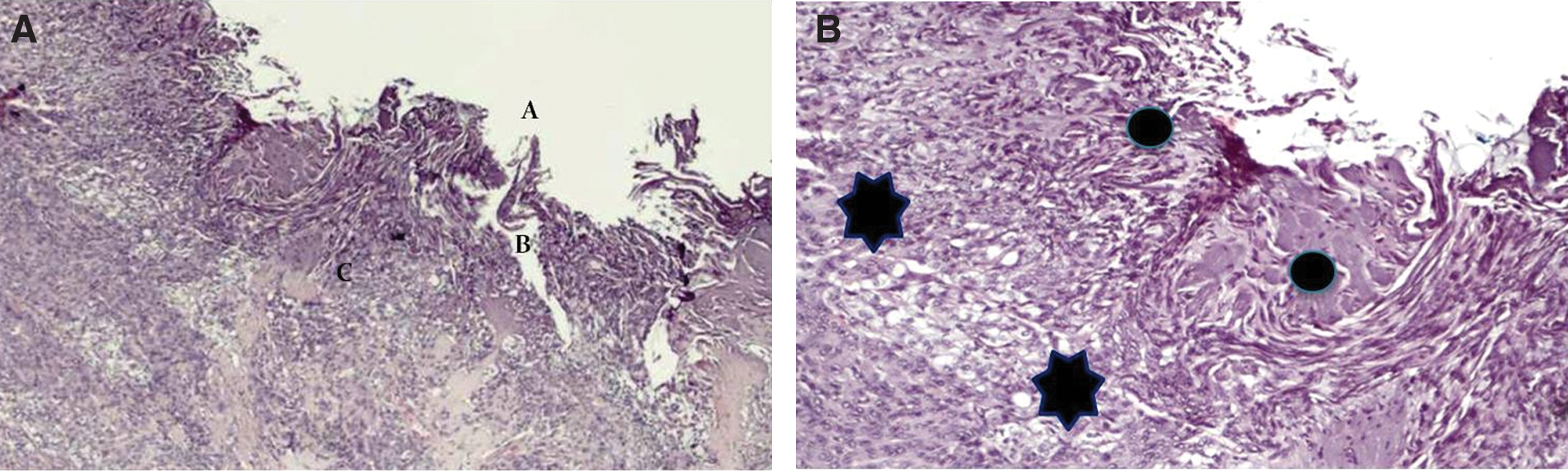
Light microscopy of laser incisions revealed three zones: area A, a central crater; area B, a vaporized zone showing a honeycomb structure; and area C, a shrunken zone showing nuclear pyknosis and hyperchromatic nuclei (Fig. 1).
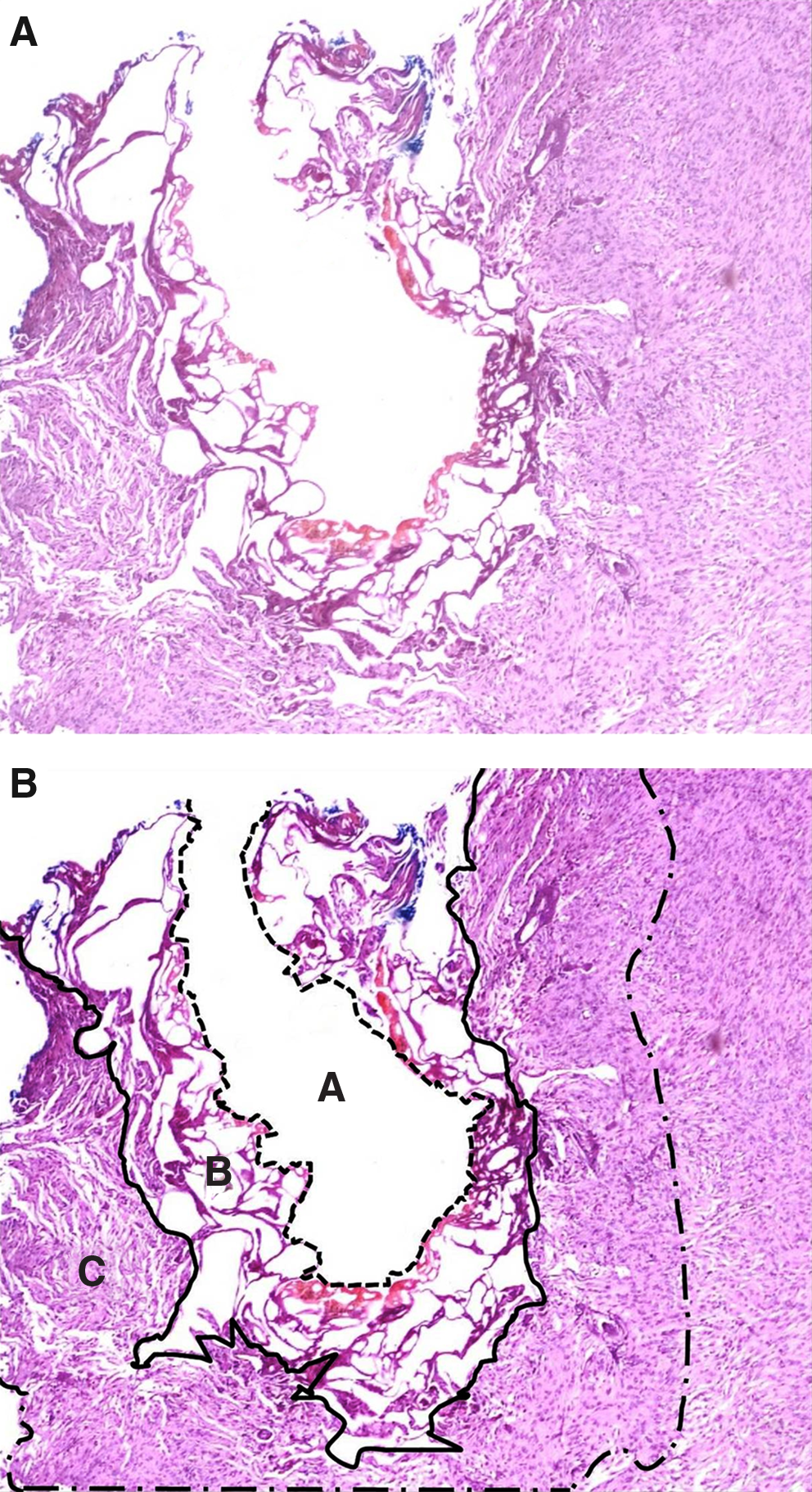
Photomicrographs of laser effects on tissue.
The depth of the incision was measured at the deepest point of the tissue effect (area A+B+C). Cytological alterations of tumor cells were also reviewed (Figs. 2B, 3B, and 4B).
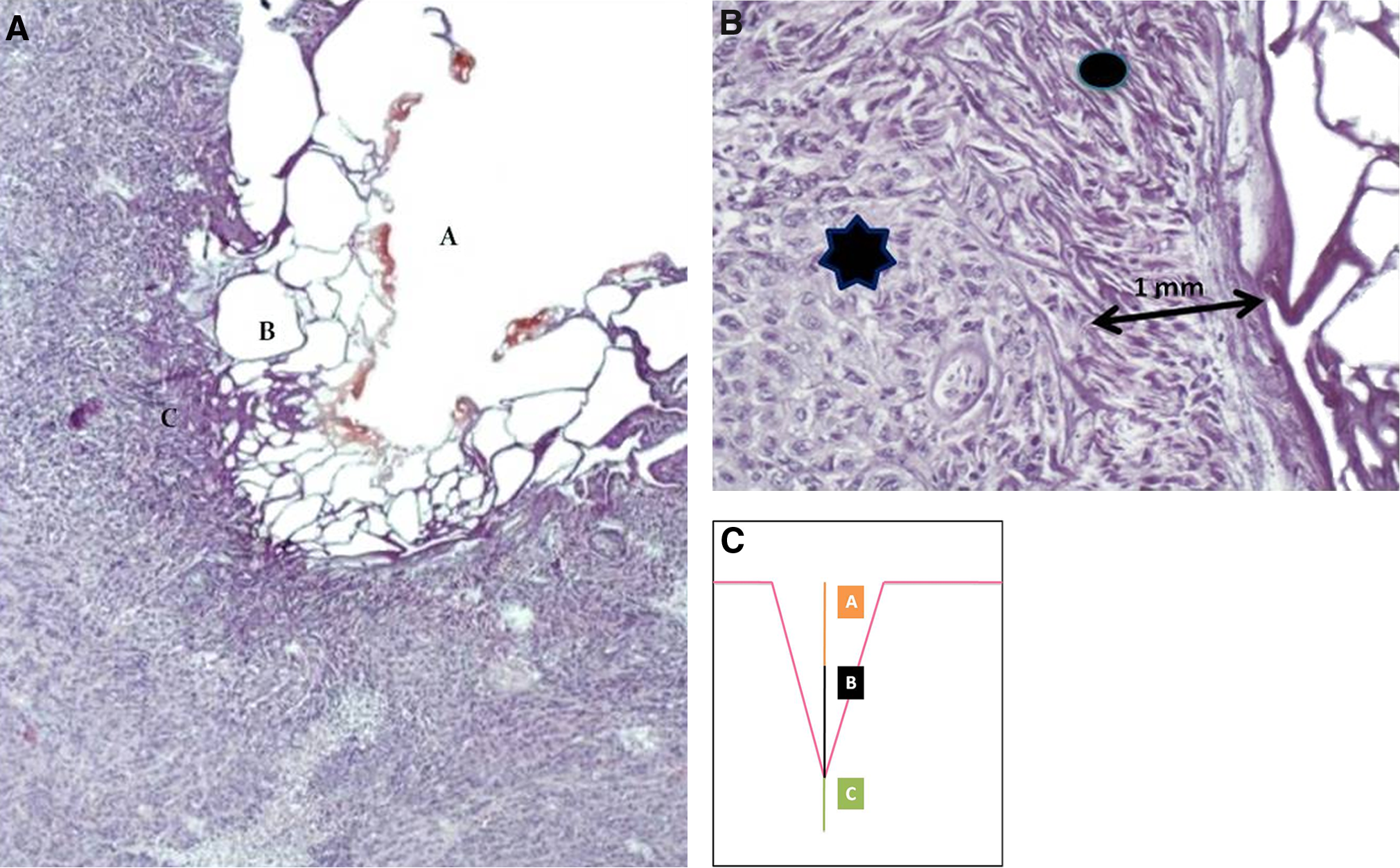
Photomicrographs of tissue changes after 2 μ thullium laser action. Meningioma was irradiated for 10 sec with the following settings: continuous wave, no touch modality, 12 W.
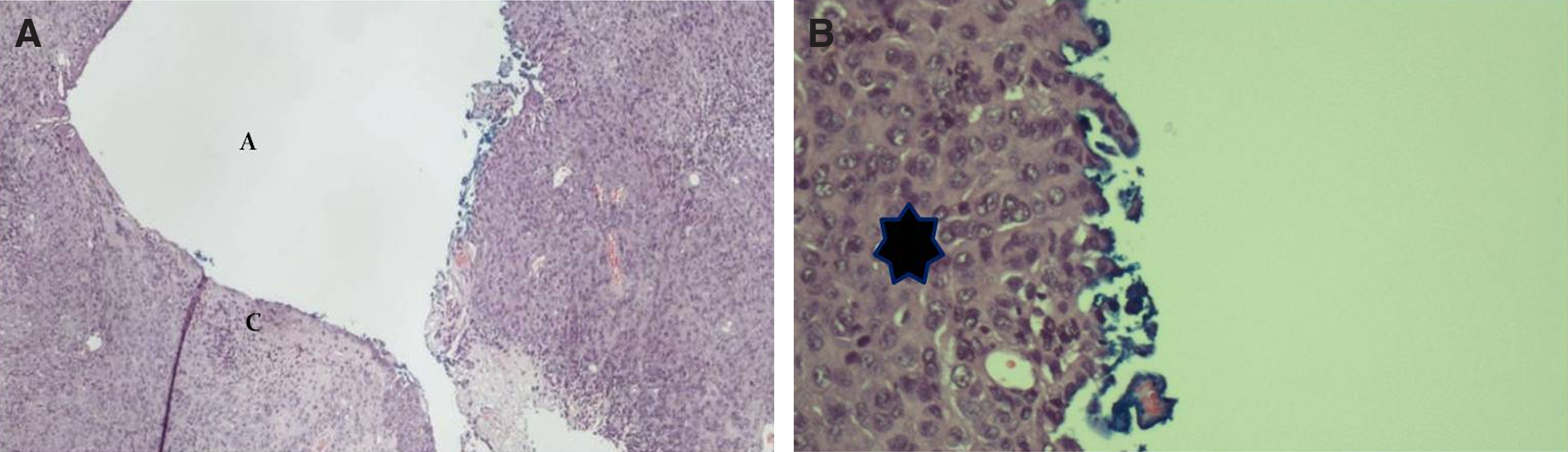
Photomicrographs of tissue changes after ultrasonic aspiration (CUSA) action.
Photomicrographs of tissue changes after bipolar forceps (set at 20% of its power) action.
Results
Laser effects
The effects of the 2-μm thulium laser on meningiomas clearly showed three distinct layers: a central crater (A), a vaporized zone (B), and a shrunken cells layer (C) (Fig. 2). These different layers were measured at the lesion point with a 6 W laser and a 12 W laser. The results of the laser effects and the cavitron ultrasonic surgical aspirator (CUSA) effects are summarized in Table 2. The average depth of the total incision at 6 and 12 W measured 1.7 and 2.51 mm, respectively. Regarding the laser settings, standard deviation was found to be 0.2 and 0.5 mm for 6 and 12 W, respectively.
A, central crater; B, vaporization and vacuolization; C, shrunken zone. A-C, total depth of tissue effect; Med, media; SD, standard deviation; CUSA, cavitron ultrasonic surgical aspirator.
The average depth of the central crater increased with increasing laser output and measured 0.8 mm with the 6 W settings and 1.2 mm with the 12 W settings. The vaporized zone showed a honeycomb aspect, and severe cellular damage was detected; the tissue was coagulated, and cells demonstrated intense pyknotic nuclei and eosinophilic cytoplasm. The average depth of the vaporized layer at the lesion point measured 0.32 mm for the 6 W laser and 0.72 mm for the 12 W laser. The shrunken layer was characterized by neoplastic cells, eosinophilic cytoplasm, and pyknotic nuclei. Deep within the tissue, the distribution of damaged tumor cells became gradually thinned. The median depth of the shrunken layer at the lesion point measured 0.39 and 0.44 mm for 6 and 12 W, respectively. Notably, there was an absence of hemorrhaging in the different areas described.
CUSA and bipolar forceps
As compared to the laser, the CUSA showed a less defined area of action (Fig. 3). Only two zones of tissue alterations were found: one central crater (A zone), which averaged 3.1 mm in depth, and a tiny layer of shrunken cells (C zone), with an average depth of 0.16 mm; a vaporized zone (B) was not seen in any sample (Table 2).
Bipolar forceps caused an irregular alteration area on the tissue (AESCULAP GN 300 BipoJet®, 20% of power). No sample showed a crater (Fig. 4). However, three zones of alteration were found in the tissue: a central, undefined crater-like zone that showed an average depth (measured at its deepest point) of 0.24 mm (A zone); a zone of irregular vaporization that was 0.5 mm in average depth measured at the deepest point (B zone); and an highly irregular zone of shrinked cells at an average depth of 0.55 mm at its deepest point (C zone).
Discussion
History of laser in neurosurgery
In neurosurgery, the laser was used for the first time in 1966 during the surgical removal of a supratentorial glioma. 23,24 A CO2 laser was used in 1968 for the removal of a recurring glioblastoma. 4,5 Ascher and Takizawa discussed the first large clinical series. 1,7 However, Deruty and Tew described the technical limitations of the CO2 laser, including reduced coagulation power (which always required bipolar cautery) and a large “laser unit” size, which was ergonomically unsuitable in the surgery room. 25,26
Many other laser prototypes have been used in neurosurgery. 1 –3,7,10,11 Argon lasers (with wavelength 488–516 nm) show an extended effect; their wavelength is absorbed by hemoglobin with excellent hemostasis, but they generate a large and undefined area of damage. 8 The Nd:YAG laser was used in a series of 120 intracranial tumor surgeries by Beck et al.; its cutting and hemostatic properties were stressed by the authors. 2 Despite this finding, its wavelength is poorly absorbed by water molecules, and its penetration through tissue is deeper. 8,10.11
Laser alterations on tumors have been studied and described by several authors. 3,10 –12 In 1984, Yamagami et al. measured the depth and width of the histological change on seven samples treated with a Nd:YAG laser. 11 They found three layers of altered tissue: one layer of vaporization and one layer of coagulation with vacuolated cells, both of which were surrounded by a third layer of tissue edema. All of these layers together were 10 mm in depth from the surface.
Between the 1990s and 2000, interest in the use of lasers in neurosurgery decreased, mainly because of a lack of solutions for the bulky nature of the CO2 laser and the higher penetration (without control) of the Nd:YAG laser. 8 In 2010, Ryan et al. 9 described a CO2 laser that was conveyed through optical fibers: a prototype that resolved the ergonomic issues of the past; however, the energy absorption by water molecules does not allow endoscopic and microsurgical use.
Applications of 2-μm thulium laser
In 2005, the 2-μm thulium laser was introduced in clinical practice, mainly in urological surgery for bladder neck incisions and for vaporesection of the prostate. 15 –18 Recently, Bach et al. reported excellent results at the 1-year follow-up of patients who had bladder neck incisions using the 2-μm thulium laser. 17 In neurosurgical practice, the 2-μm thulium laser was used in third ventriculostomy procedures. 20 Used in continuous modality, the laser cuts and vaporizes tissue with a limited degree of penetration and diffusion. Water, despite increasing heat, maintains its absorption properties more than hemoglobin during laser incision. Moreover, the thulium laser's wavelength is close to the absorption band of water (1.92 nm); therefore, thermal damage is limited and the cutting precision is higher. 22 In an aqueous medium, the laser effect on tissue is restricted to <2 mm before the tip of the fiber, and any tissue that is further afield is shielded by the medium. Laser irradiation is delivered to the surgical site through flexible fibers that are ideal for microsurgery and endoscopic use.
Histological findings
The thulium laser effect on meningiomas was standardized in all cases analyzed; all lesions produced by the laser were clearly detected upon histological examination. Three distinct zones were defined: a central crater (A zone), a vaporized zone showing a honeycomb structure (B zone), and a shrunken zone with nuclear pyknosis (C zone) (Figs. 1 and 2). The average depth of the crater increased with increasing laser output and measured 0.8 mm for the 6 W laser and 1.2 mm for the 12 W laser. The average depth of the vaporized layer at the lesion point measured 0.32 mm for the 6 W laser and 0.72 mm for the 12 W laser. The median depth of the shrunken layer measured 0.39 and 0.44 mm for the 6 and 12 W lasers, namely. Furthermore, deep within the tissue, the distribution of damaged tumor cells became gradually coarser. One very important observation was the absence of an area of hemorrhage within the different areas described.
The shrunken zone explains the large shrinking effect of the tumor and the small vessel coagulation. The average penetration depth measured at its deepest point was 1.7 mm (laser used in continuous mode, 6 W of power) and 2.51 mm (laser used in continuous mode, 12 W of power), respectively; low power settings (6 W) caused a shallow penetration of the tissue. However, histological alterations under the cutting zone were < 0.62 mm in depth in all samples, confirming that vaporization and coarctation were strictly limited and well controlled.
It is important to stress that the crater area (A zone, Fig. 2) was 0.8 mm at 6 W and 1.2 mm at 12 W.
Conversely, these settings showed no marked differences in the B zone (the area with higher histological damage) and in the C zone (the area of typical cell alteration, like pyknosis). Differences in the mean depth of these layers, when comparing the 6 and 12 W settings, were lower (e.g., B area - 0.5 mm at 6 W and 0.7 mm at 12 W; C area - 0.39 and 0.45 mm at 6 and 12 W, respectively). These data clearly showed that the extension of thermal damage was reduced to an average depth of 2 mm, with a larger effect on the central pit (A area) and limited damage to the surrounding tissue.
Differences in penetration depth might be related to the consistency and histology of the tumor. Standard deviation of the value of depth penetration was found to be acceptably low.
The CUSA also causes crater lesions, but the three layers of tissue alteration induced by the laser could not be identified (Fig. 3). Vaporized tissue was lacking, and the shrunken layer was extremely tiny. Compared with the laser, the CUSA only removed tissue without shrinking and cautery.
Bipolar cautery produces histological alterations similar to those caused by lasers, with three visible layers of tissue alteration; however, the different zones are defined less clearly, and the crater-like zone is smaller compared to that induced by the laser. In tissue, the bipolar forceps (set at 20% of its power) causes a tiny crater-like zone (A), a vaporization zone (B), and a shrunken zone (C) (Fig. 4). The dimensions of these layers are similar to the laser alterations, but their edges and extensions highlight a gradient of undefined changes.
Conclusions
The thulium laser can be used as a safe and effective surgical aid in the surgical treatment of intracranial meningiomas. The laser is effective in water, and its energy can be conveyed through optical fibers. These features make it suitable for microneurosurgery and endoscopic neurosurgery. As compared with the ultrasonic aspirator, the 2-μm thulium laser is characterized by the ability to shrink and coagulate tumor tissue. In contrast, when compared with bipolar cautery, the laser causes a more defined and precise cut on the tumor, with a higher vaporization power.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.