
Abstract
Introduction
A previous review has summarized relevant work up to 2005 on topical PDT for noncancerous skin conditions, 9 but there have been no recent reviews on PDT and wound healing. A case report included a brief summary of studies pertaining to the effects of PDT on wound healing 10 but there was no critical analysis of the studies and findings or synthesis of ideas. It seems plausible that PDT performed using a suitable PS and route of administration, together with carefully chosen laser parameters, could be developed into an effective treatment modality to promote wound healing.
PSs can be divided into azine dyes (phenothiazines and acridines such as methylene blue (MB), toluidine blue O), macrocyclic photosensitizers (porphyrins, chlorins, phthalocyanines, and a naphthodiathrone known as hypericin), and others that are metallated derivatives. 11 –14 The chemical structures of some of the PSs show considerable similarity (see Pazos and Nadler 15 ). A variety of PSs from different groups including porphyrins, chlorophyll derivatives, phthalocyanines, and azines, has been effective in the photokilling of many Gram-positive and Gram-negative bacterial pathogens in addition to parasites, fungi, and viruses. 6 Several PSs are available for clinical use such as Photofrin (porfimer sodium) and Foscan (meta-tetra [hydroxyphenyl] chlorin [m-THPC]). They all aim to achieve high absorption of laser irradiation at longer wavelengths, thereby allowing the light to penetrate deeper and allowing the treatment of large tumors; have high production of ROS including singlet oxygen, low photobleaching (only a small decrease in photosensitizing ability upon exposure to light), high chemical stability, and preferential uptake by target tissue; and are not harmful to target tissue until the laser beam is applied.
Different types of PSs target different parts of the cell, for example, m-THPC has been shown to localize in the Golgi apparatus and endoplasmic reticulum, 16 5-aminolevulinic acid (5-ALA) has been shown to localize in the mitochondria, 17 and MB has been shown to localize in the lysosomes. 18 5-ALA is a prodrug that enters the heme biosynthetic pathway and is metabolized intracellularly to form the photosensitizing molecule PpIX. 19
Some PSs accumulate in endothelial cells of vascular tissues allowing “vascular targeted PDT”. 20
Treatment with PDT requires defining the parameters of both the PS and the laser irradiation used. For the PS, important parameters for in vivo wound studies include time of application relative to that of laser irradiation and wounding; number of applications (if more than a single application); and timing, route of administration, and dose given. For laser irradiation, important physical parameters are wavelength, spot size, power, power density, energy, energy density, number and duration of irradiations, frequency of irradiation if using a pulsed laser, and interval between consecutive irradiations. At present, the relevance of these parameters to the healing effects of PDT on skin wounds and conditions remains unclear. Choice of PS, laser light sources, and treatment parameters of PDT have varied considerably in different clinical trials and animal experiments. 9
This article extends previous reports in this area by critically reviewing those articles published up to August 2010. The aim was to review experimental studies of PDT in humans and experimental animals, and on cells in culture, to assess the possible effects of such treatment on wound healing, cell viability, and proliferation. It would be helpful to identify those sets of PDT parameters that stimulate wound repair and proliferation of cells such as fibroblasts, endothelial cells, and keratinocytes that are essential to the formation of granulation tissue, deposition of collagen, vascularization, and re-epithelization of wounds. Lymphocytes play an important role in wound healing through the release of secreted cytokines and growth factors, 21,22 and the effect of PDT on these cells is also relevant. Sets of PDT parameters having no significant effects on the measured wound outcomes could still represent an important treatment modality in terms of a possible antimicrobial action on infected wounds.
The current review included assessment of: 1. The quality of the study designs and protocols used 2. The experimental protocols and PDT treatments used for in vivo studies and the appropriateness of these to clinical applications in humans – including choice of PS; route of administration and dose of PS; wavelength, power density, energy density, duration, frequency of irradiation if pulsed; and number and interval of laser irradiations 3. The experimental protocols and PDT treatments used for in vitro studies including choice of PS; concentration of PS and duration of treatment of cells; and power density, energy density, duration, and number and interval of laser irradiations 4. The relevance of PDT parameters to any observed effects.
Methods
A systematic review of the relevant literature was performed. Original research articles investigating the effects of PDT on wound healing in humans and experimental animals, together with effects on human and animal cells in culture, and published up to August 2010, were retrieved and used for this review. Relevant articles were sought and obtained from library sources and the online databases PubMed and Medline using EndNote X1 (Thomson Reuters, Carlsbad, CA).
Search terms were “photodynamic therapy”, “photosensitizer”, “laser ”, and “wound healing”. Additional secondary sources of information included reference lists from retrieved articles, and pertinent articles identified by hand searches of relevant journals not found from the databases.
We included studies that met the following c riteria: 1. PDT was investigated as the primary intervention (independent variable) 2. The type of PS, route of administration, and dose were defined for studies in vivo for humans or experimental animals 3. The type of PS, concentration, and duration of treatment were defined for studies in vitro using human or animal cells or cell lines 4. The type of laser or light source and precise wavelength were defined or implied 5. At least one outcome or index of wound healing, cell viability, cell proliferation, or cell morphology was reported 6. Studies related to wound repair, soft tissue regeneration, cell viability, or cell morphology
Studies excluded from this review are summarized in the flow chart, Fig. 1.
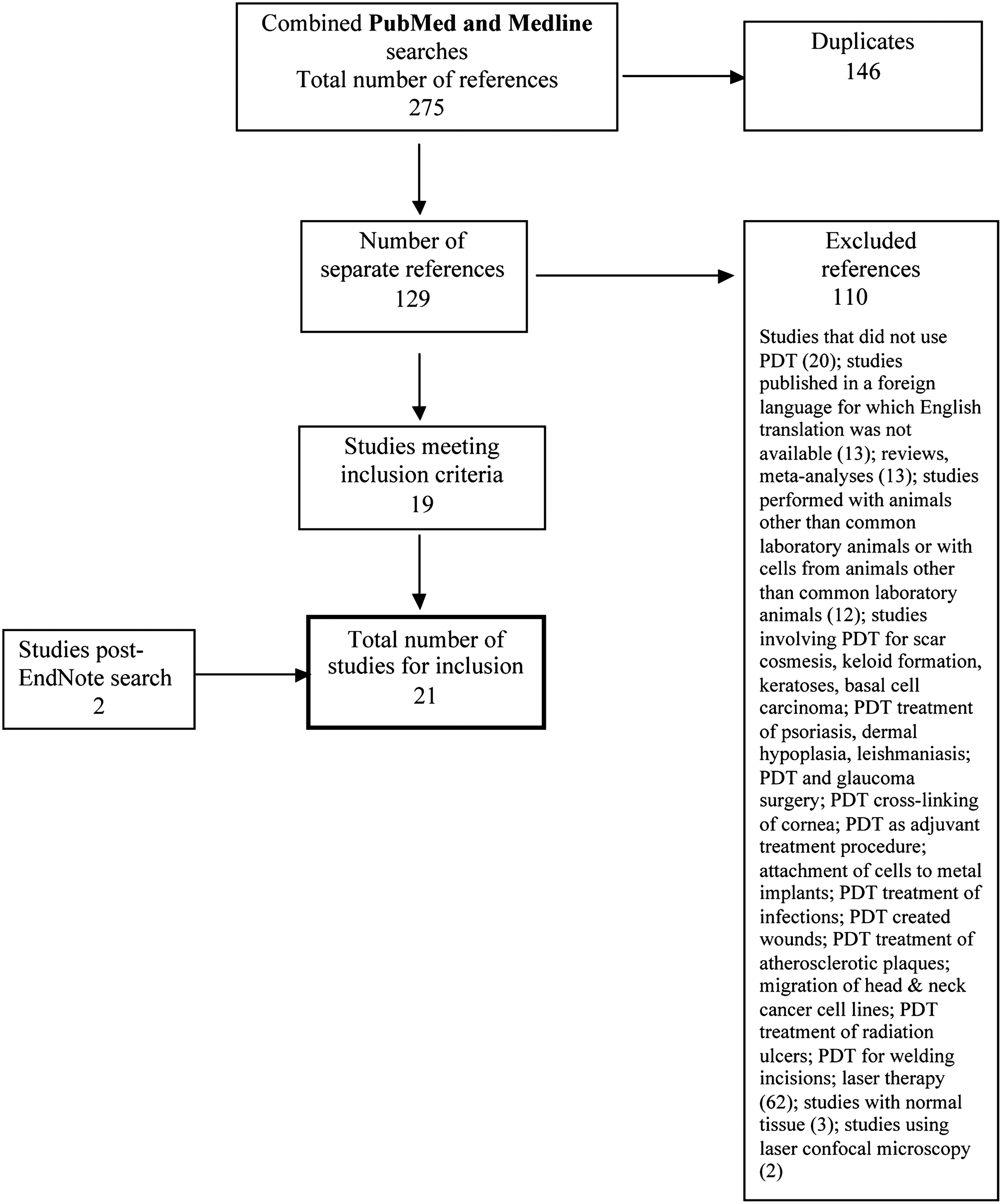
Flow chart of literature search: Studies of PDT on wound healing and cells in vitro.
EndNote searches were performed by one of the authors and the findings were confirmed by a second person. Articles for inclusion and exclusion were identified independently, and confirmed, thereby minimizing bias. For included articles, the following data were extracted and tabulated by one of the authors and confirmed by a second person:
research method (in vivo studies: controls, randomization, blinded outcome assessment; in vitro studies: controls, minimizing variability in experimental conditions)
subject and sample type (human subjects, animal species, sex, age and/or body weight, number of subjects or animals, division into groups, group sizes, strain of animal species)
description of wounds (type of wound, method of creation, number of wounds, location, distance apart for multiple wounds, area of wounds)
cell type (human or animal cells; source, and for the latter the species);
description of cells (normal cells, tumor cells, cell lines, group sizes, number of replicates)
PS parameters
laser irradiation parameters
experimental outcomes
authors' conclusion: (results of PDT exposure)
Results
Results from the literature search are summarized in Fig. 1. Twenty-one searched articles were included in this review, 23 –41 and are summarized in Tables 1 –11.
Fluence rate or flux.
Fluence.
Fluence rate or flux.
Fluence.
Klebanov, G.I., Shuraeva, N.Y., Chichuk, T.V. et al. (2005). A comparative study of the effects of laser and light-emitting diode irradiation on the wound healing and functional activity of wound exudate cells. Biophysics 50, 980–985.
SOD, superoxide dismutase.
Fluence rate or flux.
Fluence.
Fluence rate or flux.
Fluence.
Fluence rate or flux.
Fluence.
Fluence rate or flux.
Fluence.
Fluence rate or flux.
Fluence.
The concentration of FBS in culture medium has been given but not of antibiotics or other additives.
Fluence rate or flux.
Fluence.
MEM, minimum essential medium; FBS, fetal bovine serum; ZnPcBr8, octalbromide zinc phthalocyanine.
The concentration of FBS in culture medium has been given but not of antibiotics or other additives.
Fluence rate or flux.
Fluence.
MEM, minimum essential medium.
The concentration of FBS in culture medium has been given but not of antibiotics or other additives.
Fluence rate or flux.
Fluence.
The concentration of FBS in culture medium has been given but not of antibiotics or other additives.
Fluence rate or flux.
Fluence.
In three of the searched articles, two separate studies were described, 31,33, 37 for a total of 24 studies.
The main findings are summarized in the following sections.
In vivo and in vitro models
The sex and age of animals were often not reported for the in vivo studies. In those in which the sex was indicated, six had used males, one had used females, and one had used both males and females.
Also, two studies were performed using incisional wounds; in one the incisions were sutured and would have healed by first intention, whereas in the other it appears that the wounds were not sutured and would have healed by second intention.
In one of the excisional wound studies, a cylinder with an expanded collar was introduced into the wound and the top was covered with a cellophane film to prevent drying and contamination of the wound. In none of the other excisional wound studies were the wounds reported to be covered and prevented from becoming desiccated.
Only in a few of the in vivo studies were inbred strains of animals used; three studies used hairless or “fuzzy” Sprague–Dawley rats, one used Lewis rats, and one used BALB/c mice. In the in vitro studies several different cell types and cell lines were treated by PDT.
Application of photosensitizer and laser light
There was considerable variation in the way PDT was performed: 1. A variety of PSs was used and at different doses, including pheophorbide a, hematoporphyrin, benzoporphyrin derivative, PpIX, Photofrin (porfimer sodium), 5-ALA, methyl aminolevulinic acid (MAL), chloroaluminum phthalocyanine (AlClPc), chloroaluminum sulfonated phthalocyanine (CASPc), octal-bromide zinc phthalocyanine (ZnPcBr[8]),MB, toluidine blue-O, Q-switch dye II, and hypericin 2. Several different routes of administration of PS in vivo were used, which included topical application, intravenous injection, intraarterial injection, intracardiac puncture, intraperitoneal injection, and oral administration 3. There were differences in the time that wounds and cells were exposed to PS prior to irradiation 4. Different wavelengths of laser light were used even for the same PS and wound model (e.g., CASPc-treated rat incisional skin wound: 675 nm; 703 nm) 5. Light scattering in vitro was minimized by placing dark barriers between wells 6. Irradiations were performed in the dark of PS-treated cells in vitro to minimize possible effects of ambient light
Photosensitizer parameters
Type of PS
Many of the studies have been performed with first generation PSs such as hematoporphyrin, 5-ALA, Photofrin, MB, and toluidine blue-O.
Second generation photosensitizers include the phthalocyanines, and have improved photophysical properties as indicated by their activation at longer wavelengths (absorption peak ∼680 nm) compared to hematoporphyrin derivatives. In addition, phthalocyanine-based dyes can be selectively accumulated in and eliminated much more efficiently from the targeted tissue. Aluminum and zinc metal ions have been incorporated to increase phthalocyanine phototoxicity. 42,43
Dose of PS
In the rat in vivo studies, dosage varied from 0.25 mg/kg for benzoporphyrin derivative monoacid ring A (intracardiac puncture) to 10 mg/kg for chloroaluminum sulfonated phthalocyanine (intracardiac puncture or intravenously) and 12–15 mg/kg for chloroaluminium phthalocyanine (topically). Even for the same PS there was a range of doses used, for example, 1, 5 and 10 mg/kg for chloroaluminum sulfonated phthalocyanine, with 1 and 10 mg/kg having been given intravenously and 5 and 10 mg/kg having been given by intracardiac puncture.
For cells in culture it ranged from 1000 to 0.00001 μg/mL (1.67 mol/L–0.017 nmol/L) for Photofrin treatment of human ocular fibroblasts.
Route of administration of PS
In most in vivo studies, the PS was given intravenously or intraperitoneally; only in five studies was it administered locally.
Time of exposure to PS
For in vivo studies, time of exposure varied from 2 min for MB to 48 h for Photofrin. For cells in culture, time of exposure ranged from 30 min for chloroaluminum phthalocyanine to 48 h for 5-ALA.
Irradiation parameters
Irradiation parameters reported in the reviewed articles varied widely, and for some there was incomplete reporting of relevant parameters: 6 of the 13 in vivo studies and 8 of the 11 in vitro studies did not provide sufficient information to allow calculation of missing parameters (see Tables 1 –11). Such variation in parameters or lack of specification of key details limits comparison between studies.
Wavelength (nm)
Wavelength was reported in all of the studies. Whereas wavelengths in the visible red range (620–720 nm) were most commonly investigated (13/13 for in vivo studies, 9/11 for in vitro studies; either in isolation or in combination with other wavelengths), wavelengths ranged from 514 nm (green) to 1600 nm (infrared). The predominance of the use of red wavelengths is in keeping with current clinical practice for laser applications in healing and cell proliferation. Whereas most of the reported findings of the in vivo studies were, regardless of wavelength employed, positive in respect of PDT-stimulating effects, the in vitro studies mainly showed inhibitory effects on a wide variety of cell types and cell lines (see Tables 12 and 13).
√ Denotes positive effect.
HPD, hematoporphyrin derivative.
Power (mW)
In eight of the in vivo studies (8/13) and eight of the in vitro studies (8/11) the power output of the light-emitting device employed was not reported. In the remaining studies, specified power output varied widely from 1 to 991 mW for in vivo studies and from 30 to 10,000 mW (10W) for in vitro studies, with the use of higher power outputs associated with a visible red argon dye laser system having a large spot size or an infrared Nd:YAG laser system. The potential relevance of this parameter to observed PDT-mediated effects was not specifically investigated in any of the reviewed studies, nor is the relevance clear from the reported findings.
Irradiance (mW/cm2)
In low level laser therapy, irradiance (or ‘power density’) is specified in mW/cm2, and derived from power (mW) and spot size or area of irradiation (cm2). Four of the in vivo studies (4/13) and five of the in vitro studies (5/11) did not specify this parameter; three of the in vitro studies did provide sufficient information on other parameters to allow this parameter to be calculated. Where specified (or calculable), irradiance ranged from 2.87 to 500 mW/cm2 for in vivo studies and from 3.22 to 65,000 mW/cm2 (65 W/cm2) for in vitro studies.
Energy (Joules, J)
Energy is derived from power (W) and time of irradiation(s). Time of irradiation where specified for in vivo studies (5/13) ranged widely from 91 to 600 sec; and where specified for in vitro studies (5/11), varied from 3 to 300 sec. Such variation reflects, in part, the range of energies or dosages used, and the reciprocity with laser power outputs (i.e., longer times are required with lower output powers to achieve a specified dosage). Energy as a parameter was specified in only one of the reviewed studies, and was 900 J. Its relevance was not specifically investigated (see radiant exposure, described in the next section), but where this could be derived from other specified parameters (10/16), its value ranged widely from 4.05 to 683 J for in vivo studies and from 9 to 650 J for in vitro studies.
Radiant exposure (J/cm2)
Radiant exposure or energy density (J/cm2) is generally considered and reported as the most appropriate means of specifying dosage, at least in the case of experimental studies. It is derived from time (sec) and irradiance (W/cm2), which is in turn derived from power (W) and area of irradiation (cm2). Radiant exposures were reported in all articles except for one of the in vitro studies, but for which it was calculable, and ranged from 1 to 100 J/cm2 for in vivo studies and from 4.5 to 2039 J/cm2 for in vitro studies. This was the parameter most commonly reported, and in some studies to assess the “dosage-dependency” of observed effects.
Irradiation regime
Considerable variation was found in the duration of irradiation, the number of irradiations, and the interval between successive irradiations. The duration of irradiation varied between 812 and 1000 sec, the number of irradiations varied between one and seven doses, and the time interval between successive irradiations varied between 1 and 7 days for in vivo studies. All of the in vitro studies involved a single irradiation and duration of irradiation varied between 3 and 1553 sec.
Measurement of outcomes
Wound healing studies
There were 13 searched studies on wound healing (n=12, animal studies; n=1, human studies). A variety of acute wound models was included in the studies (incisional; excisional − full thickness; burns − thermal; skin flaps; vascular injury; colon anastomosis). Further details regarding these studies are given in Tables 1 –7.
In vitro studies
There were 11 searched studies describing in vitro studies (n=2, animal studies; n=9, human studies). A variety of different cell types were exposed to PDT, as well as certain cell types incubated on PDT-treated three-dimensional matrices. These are summarized in Tables 8 –11.
Discussion
Research design and reporting of studies
As in other recent reviews, by far the largest number of in vivo studies were performed in the rat, mostly using outbred strains such as Sprague–Dawley and Wistar. A small number of carefully chosen inbred strains would be beneficial in reducing the numbers of animals used. There was also an under-representation of females in the animal studies. It would seem important that studies should obtain data from sufficient numbers of both males and females to ascertain whether there are any differences in healing outcomes between the two sexes. Very few of the studies provided any rationale for the selection of strains or sexes of animals. Also in females there may be a hormonal influence on wound healing, 44 and it was reported that the thinner skin of female rats allows a faster rate of wound healing with a higher rate of wound contraction than in male rats. 45
The models used were mostly of acute wounds. There were no studies using impaired healing models (e.g., diabetic-impaired) which would have relevance to stimulating the healing of slow-to-heal wounds. Also, there was considerable variation in the size, number, and location of wounds in individual animals. It is of concern that in creating multiple wounds, the healing of wounds made subsequently may be influenced by mediators (e.g., growth factors, cytokines) released from tissues injured when the first wounds were created. Also, for the majority of reviewed studies, the wounds were not reported to be covered, and therefore wound contraction would have been the main contributor to wound closure.
In only a few studies was it indicated that animals were randomly assigned to treatment groups. Also, only two of the studies reported that the histology slides were examined by a pathologist blinded to the treatment groups. Randomization and blinding are important to minimize bias.
Experimental models and influence of PDT on healing
A variety of in vivo animal models was used in the studies and included cutaneous wounds (incisional, excisional, burns), fasciocutaneous flaps, vascular injury, and colon anastomosis. Most of the studies had been performed in an outbred strain of rat, thereby requiring large group sizes to show statistically significant changes brought about by PDT. For one of the two incisional wound studies in the rat, the sutured wounds would have healed by first intention; in the other study, the non-sutured wounds would have healed by second intention. In both of these studies multiple wounds were made. This has the disadvantage that the healing of untreated wounds (dark controls) could have been inadvertently affected by laser light exposure and by the release of biologically active agents from the treated (irradiated) wounds, as well as by PS in the systemic circulation. The series of wounds could also have been influenced by agents released or diffusing from adjacent wounds. In all except one of the rat excisional wound studies, the wounds were not covered by a film dressing and healing would have occurred by second intention, with the wound margins being pulled inwards by contraction. There was also a single case report on a human patient with recurring basal cell carcinoma treated with Mohs micrographic surgery followed by PDT.
The rat in vivo studies have been critically analyzed to identify those in which a positive effect of PDT on wound healing was demonstrated, and are summarized in Table 12. These studies involved excisional wounds, third-degree burn injury, and vascular injury in rats, and they used low doses of PSs together with visible red laser light, wavelengths ranging from 632.8 to 685 nm, or combined with infrared light (1064 nm). They all showed improved histological wound outcomes, and there was an enhancement compared to using laser alone for all those studies in which a “laser-only” group had been included. However, it is unclear whether the laser treatment alone was performed with optimum parameters for healing. PDT using Photofrin had an inhibitory effect on the healing of rat skin flaps; whether such an effect on the healing of skin flaps is brought about by PDT with a different PS is unknown. In addition, PDT with 5-ALA did not affect the healing of mouse colon anastomosis.
In general, the groups of animals treated with laser alone demonstrated positive effects on healing outcomes, and these were further improved by combining PS and laser light. The latter included such findings as reduced leukocyte activity in wound exudates, connective tissue remodeling, increased re-epithelization of wounds, and re-endothelization of injured arteries.
Types of cells used and influence of PDT on cellular parameters
Cell types exposed in vitro to PDT were human endothelial cells, human keratinocytes, human lymphocytes, mouse and human fibroblasts, human laryngeal carcinoma cells (HEp-2 cell line), and human lymphocyte cell lines. Endothelial cells, keratinocytes, and fibroblasts are essential for wound repair, with fibroblasts and endothelial cells involved in the laying down and vascularization of granulation tissue in the wound bed, and keratinocytes in the re-epithelization of wounds. Lymphocytes have important immune functions and secrete products that modulate the functional activities of many other types of cells. Except for human lymphocytes from healthy donors and human fibroblasts (from lung) in which little or no change in cell viability occurred on exposure to 5-ALA and helium-neon laser or xenon (non-laser) light, respectively, all of these studies showed inhibitory effects on cell viability brought about by PDT or PS alone (Photofrin). Q-switch II dye at a nontoxic dose enhanced the cytotoxic effect of laser irradiation (Nd:YAG, 1060 nm) at temperatures as low as 36°C; at temperatures as low as 24–34°C, cell duplication was inhibited, but cell viability was unaffected. These effects are summarized in Table 13.
There was a marked difference in responsiveness to 5-ALA-mediated PDT of blood lymphocytes from healthy human subjects and leukemic patients. In most cases, a high percentage of leukemic cells was quite easily damaged by this PDT without needing to resort to higher PS concentrations or irradiances. It was almost impossible to obtain any appreciable damage of normal lymphocytes even with the highest PS-PDT doses tested. These contrasting reactions have been explained as caused by peculiarities of heme metabolism in leukemic cells. 37 An increase in heme formation inhibits the activity of a rate-limiting enzyme aminolevulinate-synthase and decreases 5-ALA concentration. If exogenous 5-ALA is introduced, the limiting step is bypassed, and the process proceeds down the chain to synthesis of PpIX. In normal lymphocytes, the PpIX by means of ferrochelatase joins Fe2+ being transformed to heme, which unlike PpIX has no photosensitizing properties. In leukemic cells, ferrochelatase activity is low, 46 as are also intracellular Fe2+ stores. 47 Consequently, in leukemic cells, PpIX is accumulated, giving rise to the cellular photosensitivity. Furthermore, in a study examining 5-ALA-esters to improve PDT on cells in culture, long-chain esters were 30- to 150-fold more efficient in inducing PpIX in carcinoma cell lines WiDr and NHIK 3025, but the efficiency was only 1–2.6 times better in the normal fibroblast cell line V79. This could be because of low esterase activity in fibroblasts, or the lower levels of 5-ALA needed to reach a maximum of PpIX accumulation in V79 cells compared to that in the carcinoma cell lines. The maximum content of PpIX brought about by 5-ALA was 3 times higher for WiDr cells than for V79 cells, indicating a higher photosensitivity of WiDr cell line compared to V79 cell line. 48
Care is needed when attempting to extrapolate findings in vitro to an in vivo situation, as in the latter there are multiple cell types present as well as an extracellular matrix consisting of a complex network of macromolecules secreted by the cells. Therefore, both cells and extracellular matrix could possibly be affected by PDT treatment. Two studies were found in which cells were cultured on PDT-treated matrices. For one of these, an extracellular matrix was prepared by culturing bovine endothelial cells at confluence for 7–8 days, and the matrix subsequently treated by PDT (chloroaluminum sulfonated phthalocyanine 5 μg/mL, 675 nm 100 J/cm2). When bovine endothelial cells were cultured on the PDT-treated extracellular matrix, there was increased endothelial cell basic fibroblast growth factor (bFGF) mRNA expression at 24 h and increased proliferation up to 72 h. In the other study, human fibroblasts were cultured on a gel matrix prepared from bovine collagen type I and collagen type III that had been exposed to PDT (MB2 μg/mL, 660 nm 100 J/cm2). Fibroblast proliferation was decreased and there was a marked reduction of fibroblast transforming growth factor beta (TGF-β)1 mRNA expression and bFGF mRNA expression. These findings are summarized in Table 14.
An extracellular matrix functions not only as an inert structural support, but also regulates attachment, proliferation, migration, differentiation, and survival of cells. 49 Whereas some of the responses of cells are mediated by various macromolecular constituents of the extracellular matrix (e.g., collagen, laminin, fibronectin, heparan sulfate proteoglycans), 50,51 active molecules such as growth factors and enzymes that are firmly associated with the extracellular matrix may also be involved. 15 It is known that bFGF is bound to heparan sulfate in the extracellular matrix with a low affinity 52 and can be released by heparan sulfate-degrading enzymes, heparin and heparan sulfate, and proteases that degrade the extracellular matrix. Endothelial cells are capable of solubilizing bFGF from the extracellular matrix, which would then be able to support proliferation of these cells. PDT treatment of the extracellular matrix inactivated bFGF without compromising the functional integrity of the matrix-resident low-affinity bFGF receptors (heparan sulfate). 53 Hence, exogenous bFGF-replenishment of the PDT-treated extracellular matrix resulted in restoring cell proliferation to a level comparable with normal untreated extracellular matrix. A collagen gel matrix, although providing structural support, would be unlikely to influence the behavior of cells in the same manner as an extracellular matrix laid down by the cells themselves. Also the mechanical properties of a collagen gel matrix affect the behavior of cells. 54 PDT of collagen gels induces matrix changes, including cross-linking, which cause a marked reduction in fibroblast migration. 55
Clinical relevance and further studies
Studies of the combined effects of PS and laser irradiation on experimental wounds in rats and mice are important for understanding the healing process involved after PDT.
When PDT is used for stimulating wound healing, it is important to minimize any damage to intact tissues, and this may be dependent upon the dose and concentration of the PS used. Some pre-clinical studies have demonstrated that the ratio of tumor to normal tissue damage after PDT is related to PS concentration, laser irradiance, and time interval between drug administration and irradiation. 56 –58 The ratio of PS concentration in tumor tissue and normal tissue is often not >2:1; often higher concentrations exist in the surrounding normal tissue than in the tumor cells. 59 As PDT might be developed into an effective treatment for slow-to-heal wounds, further studies should be performed using animal models with delayed and impaired wound healing; for example, genetic diabetic mice in which the wounds are covered by an occlusive dressing. We have shown that covering full-thickness excisional wounds in genetic diabetic mice with a transparent adhesive dressing causes a retardation of contraction, and such wounds are described as “splinted”. 60 The healing of these wounds is delayed compared to unsplinted wounds, but is stimulated by irradiation at 660 nm, and mimics that in human patients. 61,62 This makes it a highly suitable animal model for examining the effects on wound healing by various PSs combined with different sets of laser parameters.
In examining the effects of PDT on cells in vitro, it would be relevant to study other cell types, such as diabetic fibroblast, wounded fibroblast, and diabetic wounded fibroblast cells. Diabetic fibroblast cells are fibroblasts grown in a medium with a high concentration of glucose (17 mM); wounded fibroblast cells are fibroblasts that have been grown to confluence and then wounded by scratching with a sharp pointed instrument such as the tip of a glass pipette, or alternatively are cells harvested from wounds (see Peplow et al. 63 ). Also, further studies should be performed in which cells are cultured on a PDT-treated extracellular matrix, as well as PDT treatment of cells cultured on an extracellular matrix. A recent study has suggested that sufficiently lowering the dose of laser light in a PDT would have a biostimulatory effect on cells similar to that in low-level laser therapy. 64 Also, tumor cells enriched with small amounts of PS may proliferate better after laser irradiation because of the low concentrations of ROS generated. 65 These possibilities must be considered when using PDT.
Conclusions
The reviewed studies showed that PDT of acute wounds can lead to an improvement of healing outcomes over those brought about by laser alone. Several first and second generation PSs have been used at low doses, administered topically or by intraperitoneal or intravascular injection, and with laser irradiation performed at wavelengths ranging from 630 to 690 nm. In contrast, the healing of skin flaps after being subjected to ischemia was impaired by PDT treatment, although only one PS (Photofrin) was tested. Further studies are required using animal models that are more sensitive to alterations in the wound healing process, and mimic better the healing of human wounds for which the main processes are re-epithelization and granulation tissue formation. In future studies, it is important to reduce risk of bias by blinding of human participants, blinding of outcome assessment, and obtaining and reporting of complete outcome data.
The reviewed studies indicated that exposure of cells in culture to PDT mostly had an inhibitory effect, reflected in a marked decrease in cell growth or viability. More appropriate in vitro cell models include diabetic fibroblasts, wounded fibroblasts, diabetic wounded fibroblasts, and cells cultured on a matrix synthesized by the cells. In PDT, irradiation of cells with low energy doses or irradiation of cells enriched with small amounts of PS may stimulate proliferation. In using PDT clinically, it is essential to use the appropriate dosimetry of both the PS and the activating light source in order to achieve cell death for cancer therapy, or regeneration for wound therapy.
PSs are being developed with a faster clearance time from normal tissues, making them more selective for tumor cells. PDT may be athermal but it is almost always traumatic as compared with the athermal and atraumatic nature of low-level laser therapy. PDT can cause burns, swelling, pain, and scarring in nearby normal tissue. 66
Footnotes
Acknowledgments
The authors acknowledge the invaluable support of Brigid Ryan and David Jackson in the preparation of the manuscript. Ms. Ryan and Mr. Jackson were supported through the Centre for Physiotherapy Research, University of Otago, Dunedin, New Zealand. No financial support has been received in conjunction with the generation of this report.
Author Disclosure Statement
No competing financial interests exist.