
Abstract
Introduction
Low-level laser therapy (LLLT) stimulates the proliferation of osteoblasts, collagen formation, and bone regeneration. 6 –8 LLLT has been shown to have several different effects, including pain relief, wound healing, and nerve regeneration. LLLT also has biostimulating effects when applied to oral tissues; it improves wound healing, 9,10 enhances epithelialization after periodontal surgery, 11,12 minimizes edema after third molar surgery, 13 and prevents induced oral mucositis. 14 In a prospective cohort of 20 patients with bisphosphonate-induced ONJ (ONJ-BP) who underwent pulsed diode laser (GaAs) irradiation, LLLT reduced pain, clinical size, and edema. 15 In another clinical study, seven patients affected by ONJ-BP were treated using a double diode laser simultaneously emitting two different wavelengths (λ650 nm and λ904–910 nm; spot size, 8 mm2). All patients were irradiated with a fluence of 0.053 J/cm2 for 15 min five times over a period of 2 weeks, in a noncontact mode, ∼1 mm from the pathologic area. Six patients showed significant pain reduction, and only one patient reported worsening symptoms, which was likely related to reinfection of the ONJ-BP site. 16 The aim of this article is to report a case of ONJ-BP of the jaw treated by curettage of necrotic bone, LLLT with GaAlAs (860 nm), and antibiotic therapy.
Materials and Methods
An 82-year-old man with melanoderma presented at the Stomatology Clinic of the School of Dentistry of the Federal University of Bahia complaining of trismus and pain in the posterior jaw region, which was making it difficult to eat. Clinical anamnesis examination revealed that the patient was undergoing chemotherapy treatment for prostate cancer with docetaxel (75 mg/m2) combined with prednisolone (5 mg twice a day) in 21-day cycles, for a total of six chemotherapy cycles. Based on the presence of bone metastasis, the oncologist started treatment with intravenous bisphosphonate (zoledronic acid, 4 mg), which was maintained until the time of dental evaluation. The patient reported that a tooth extraction (unit 47) performed 6 months previously did not heal.
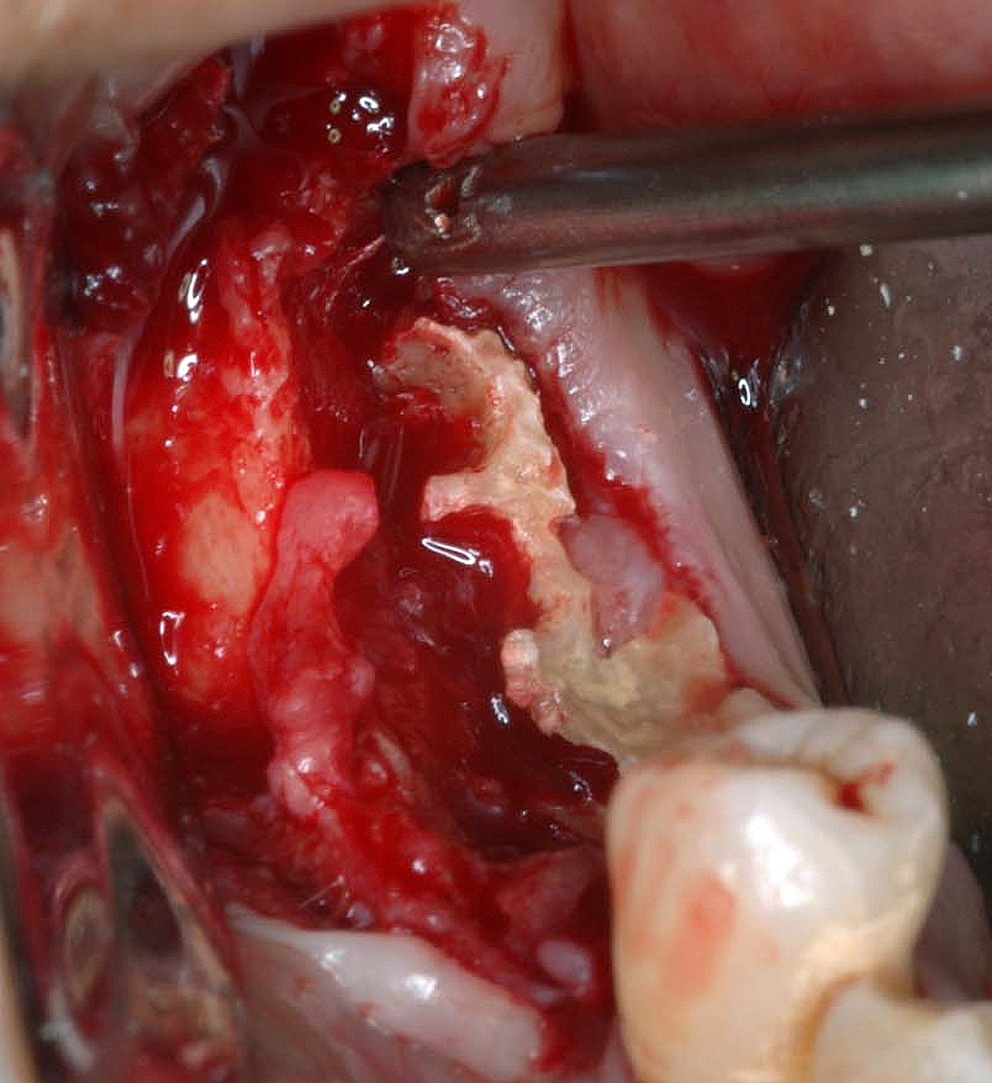
In the region of tooth 47, there was exposed necrotic bone (Fig. 1) and increased volume of hyperplasic buccal mucosa in this area. On panoramic radiography, a diffuse bone rarefaction was observed in this region (Fig. 2). A CT scan showed a hyperdense area compatible with mandibular bone sequestration. Hematological laboratory test results were within reference values. Pathological examination revealed nonspecific inflammation associated with the presence of bone necrosis, confirming the diagnosis of osteonecrosis.

Intraoral aspect showing exposed necrotic bone.

Panoramic radiography revealing diffuse bone rarefaction in the region of the right mandible.
The surgical treatment consisted of the extraction of tooth 46, curettage of necrotic bone (Fig. 3), copious irrigation with chlorhexidine 0.12%, suturing the area, and then prescribing the use of amoxicillin (500 mg) every 6 h for 10 days. The removed tissue was sent for pathological examination.
Curettage of necrotic bone after extraction of tooth 46.
Immediately after surgery, the area was exposed to focused and continuous irradiation with a diode laser set for low-intensity infrared emission (GaAlAs; λ860 nm, 70 mW; Twin Flex Evolution® MMoptics; São Carlos, SP, Brazil). Irradiation was applied in a punctual contact manner at three points along the wound, with an energy density of 4.2 J per point for 1 min and 30 sec of irradiation, every 48 h for a period of 10 days. The patient underwent a total of five treatment sessions.
Results
After 7 days, the sutures were removed and revealed good healing of the operated area, without evidence of complications until the 30th day of follow-up (Fig. 4). From the second session onward, the patient reported gradual improvement in the tenderness of the region. Solid food intake was possible after the third session. This aspect is important because it shows that well-being greatly improved during treatment, leading to a better quality of life.

Postoperative aspect of the operated area showing good healing on the 30th day of follow-up.
Discussion
No definitive standard of care has been set for ONJ-BP. For most patients, a complete cure is not possible. Numerous clinical protocols to treat areas of exposed bone have been proposed, and reduction or even resolution of clinical signs has been reported using conservative treatment modalities. Osteonecrosis has been treated by prophylactic procedures such as use of chlorhexidine 0.12%, curettage, or wide and radical surgical resection, depending upon the severity of the injury. 17,18 Extensive and radical surgical resection rarely results in long-term successful wound closure and sometimes leads to worsening of disease.
Few studies have reported the long-term management and outcome of ONJ-BP patients treated with laser therapy. Scoletta et al. reported a prospective cohort of 20 patients affected by ONJ-BP in which patients were exposed to a 904-nm infrared laser (50 kHz; energy density, 28.4 J/cm2). 15 Four weeks after LLLT, a statistically significant decrease in reported pain, clinical size, edema, and presence of pus and fistulas was observed. 15 In another clinical study, significant pain control was achieved using a double diode laser simultaneously emitting two different wavelengths (λ650 nm and λ904–910 nm); patients were irradiated with a fluence of 0.053 J/cm2 for 15 min five times over a period of 2 weeks. In contrast, the present study used curettage and antibiotic therapy in combination with LLLT. Furthermore, we used a different LLLT protocol: we used an energy density of 4.2 J per point for 1 min and 30 sec per point. This protocol successfully improved bone healing in several conditions, such as alveolus of dental extraction, especially during the early stages of healing. 19
The low-level laser is a potential biostimulant when applied to oral tissues 15,20 and may stimulate neoangiogenesis of blood and lymphatic vessels. 20 Positive effects on the synthesis of DNA and RNA and on synthesis of collagen and its precursors have also been reported, as were positive effects on the levels of prostaglandin, phagocyte cytoplasmic granules, neovascularization, and cell proliferation. Laser therapy influences the production of adenosine-5′-triphosphate (ATP) 19 and accelerates cellular metabolism, which results in enhanced healing processes.
Studies have investigated the effectiveness of low-intensity lasers using infrared light to stimulate bone production. 6,21,22 Use of low-intensity lasers improves bone mineralization in traumatized sites, particularly in inorganic compounds. 6,21 –23 Therefore, one could postulate that the use of low-intensity lasers can be useful in the treatment of osteonecrosis.
In the present case, the patient presented with ONJ-BP after tooth extraction. The patient was receiving intravenous bisphosphonate for the treatment of prostate cancer. The association of bisphosphonates with osteonecrosis in the jawbones has been reported. 2,17,24,25 Ruggiero et al. reported 63 cases of osteonecrosis, and 56 of these were positively associated with the use of bisphosphonates. 26 Bisphosphonates have an affinity for hydroxyapatite crystals located in areas of bone resorption and bone remodeling 24 and are therefore able to inhibit bone resorption in both normal and pathological bone. 26
Multiple mechanisms may explain the pathogenesis of ONJ-BP. One possibility is the inhibition of osteoclastic action, 27 –29 through increased apoptosis and inhibition of the development of osteoclasts, inhibition of bone-marrow precursor recruitment, and osteoblastic stimulation. These effects on osteoclastic action result in the release of osteoclast inhibiting factors, which slow the progression of bone destruction and improve the chances of healing and recovery of bone strength and density. 24,29 Interference in the angiogenic process has also been reported. 27 In vitro and animal studies have shown that the bisphosphonates pamidronate and especially zoledronate have direct antiangiogenic effects on endothelial cells, causing a sharp reduction in intraosseous blood flow. 30,31 Bone remodeling enables the bone to achieve functional requirements, and bisphosphonates bind avidly to bone absorption gaps, especially at sites of intense remodeling, such as in gnathic bone. These bisphosphonates are not metabolized, remain at high concentrations for long periods, 32 and decrease bone resorption. Decreased bone resorption inhibits the normal turnover of bone, resulting in the accumulation of microdamage and reduced mechanical properties; 26,33 this constrains the repair of physiological microfractures that are caused by chewing forces, 33,34 trauma, or invasive dental procedures. 28 Therefore, osteoclastic inactivity causes osteonecrosis of the jaws in 1.8–12% of bisphosphonate users by impairing the repair of these microcracks. 5 Although the aforementioned mechanisms are considered a determining factor for the occurrence of this injury, 35 relative ischemia of the bone, 30,31 underlying disease, chemotherapy, and corticosteroids may also be supporting the promotion of infection and necrosis. 36 The type of dental intervention, number of treatment cycles, exposure time, and route of administration of bisphosphonates (oral or intravenous) are among the main factors that seem to affect the incidence of osteonecrosis. 35 Intravenous bisphosphonates can dramatically influence bones, leading to an increased risk of developing osteonecrosis. 17 The patient described in this study possessed several of the major aggravating factors reported to be responsible for the development of osteonecrosis.
Although many cases osteonecrosis occur spontaneously without any apparent trauma or the use of concomitant bisphosphonate, ∼60% of cases occur after tooth extraction, 35 which was the case in this study.
Laser phototherapy is an effective therapeutic alternative for biomodulation of tissue healing and pain control; it is easy to perform and does not increase morbidity or cause side effects when an appropriate protocol is used. 15,37 The effect of laser therapy on bone regeneration depends not only on the total dose of irradiation but also on the irradiation time and the irradiation mode. 19 The laser irradiation protocol adopted for the present patient was effective because from the second session onward, the patient reported decreased pain, and positive tissue healing effects were observed within 7 days after phototherapy treatment.
Conclusions
The present therapeutic protocol showed positive effects on tissue healing and remission of painful symptoms, thus improving oral health and patient quality of life. Larger, randomized clinical trials are required to further investigate the efficacy of this protocol for the treatment of bisphosphonate-induced osteonecrosis.
Footnotes
Author Disclosure Statement
No competing financial interests exist.