
Abstract
Introduction
Materials and Methods
Patient population
Between January 2008 and September 2009, a total of 47 consecutive patients were treated with PCFD at Daegu Wooridul Spine Hospital. The inclusion criteria for PCFD were foraminal cervical disc herniations manifesting as radiculopathy. Both computed tomography (CT) scanning and magnetic resonance imaging (MRI) were performed for all patients. Patients with segmental instability, central disc herniation, ossification of the posterior longitudinal ligament (OPLL), or cervical myelopathy were excluded. Of the 47 patients, 24 patients were treated with laser-assisted PCFD, whereas the remaining 23 patients were treated with conventional PCFD. For the given criteria, the surgical technique was selected according to the preference of the surgeon on call. Surgeons with a preference for the conventional technique (Drs. Kang and Kim) performed conventional PCFD; whereas those with prior experience with the laser technique (Drs. Ahn and Hur) performed laser PCFD for the same disease entity.
Outcome measurements and statistical analysis
Clinical outcomes were evaluated using the visual analogue scale (VAS) for pain intensity, and the Neck Disability Index (NDI) 9 for functional status. Clinical outcomes were also classified as excellent, good, fair, or poor based on the modified MacNab criteria. 10 Surgical complications such as hematoma, infection, dural damage, neurologic deficit, recurrence, and instability were documented during the follow-up period. Comparison between the two groups was made using the independent two-sample t test for continuous variables. Fisher's exact test was performed for categorical variables. A two-tailed p value of <0.05 was considered significant.
Operative technique
The procedure was performed in two phases. First, a standard posterior cervical foraminotomy technique was performed; 11 second, a novel laser-assisted selective discectomy technique was performed. Under general anesthesia, the patient was positioned in a tilted and prone position on a radiolucent table, which is commonly used for conventional PCFD at our institution, Wooridul Spine Hospital (Daegu). The appropriate level for the incision was localized using a fluoroscope or lateral simple radiographs. After a small skin incision was made, a subperiosteal dissection was performed along the lamina surface to the facet joints. A self-retractor (Papavero-Caspar speculum, B Braun, Germany) was then used to expose the lamina and facet joints above and below the targeted disc space. The facet junction is the beginning of the entrance into the spinal canal and foramen. The lateral portion of the lamina and medial facet joints was drilled out using a high-speed diamond drill under a microscope. The lateral third of both the superior and inferior hemilaminae, as well as the medial half of the descending and ascending facets, were gently drilled until the underlying nerve root was exposed. To minimize damage to the nerve root or cord, drilling was performed parallel to the course of the nerve root from the medial to lateral direction, and over the spinal canal from the rostral to caudal direction. The collection of veins overlying the nerve root was coagulated and removed for better visualization of the nerve itself. Once the nerve root was identified in the conventional PCFD group, the extruded disc fragments and osteophytes were removed using pituitary forceps or curettage with gentle retraction of the nerve root. In contrast, the compressive disc fragments were removed by CO2 laser instead of mechanical instruments in the laser PCFD group. After removing any sequestered free fragments using forceps, the nerve root was retracted to reveal the compressive disc fragment. This fragment was then gradually evaporated using a CO2 laser (Sharplan 30C, Lumenis, Yokneam, Israel) attached to a microscope (Fig. 1). The laser aperture at the probe tip was connected to the microscope. Thus, the direction of the laser beam could be controlled using a joystick attached to the microscope. The unit could be activated for laser emission by a footswitch. The pinpoint size laser was used at a power level of 10 W, which allows safe and precise evaporation. The CO2 laser was also used to detach adhesions and sculpture osteophytes compressing the nerve root. Once the nerve root was adequately decompressed, it moved freely, and no pressure was felt. The photocoagulation effect of the CO2 laser may reduce bleeding from soft tissue and bone during the decompression process. In every case, thorough hemostasis was achieved and the wound was closed with insertion of Hemovac (EASY Medicare, Korea).
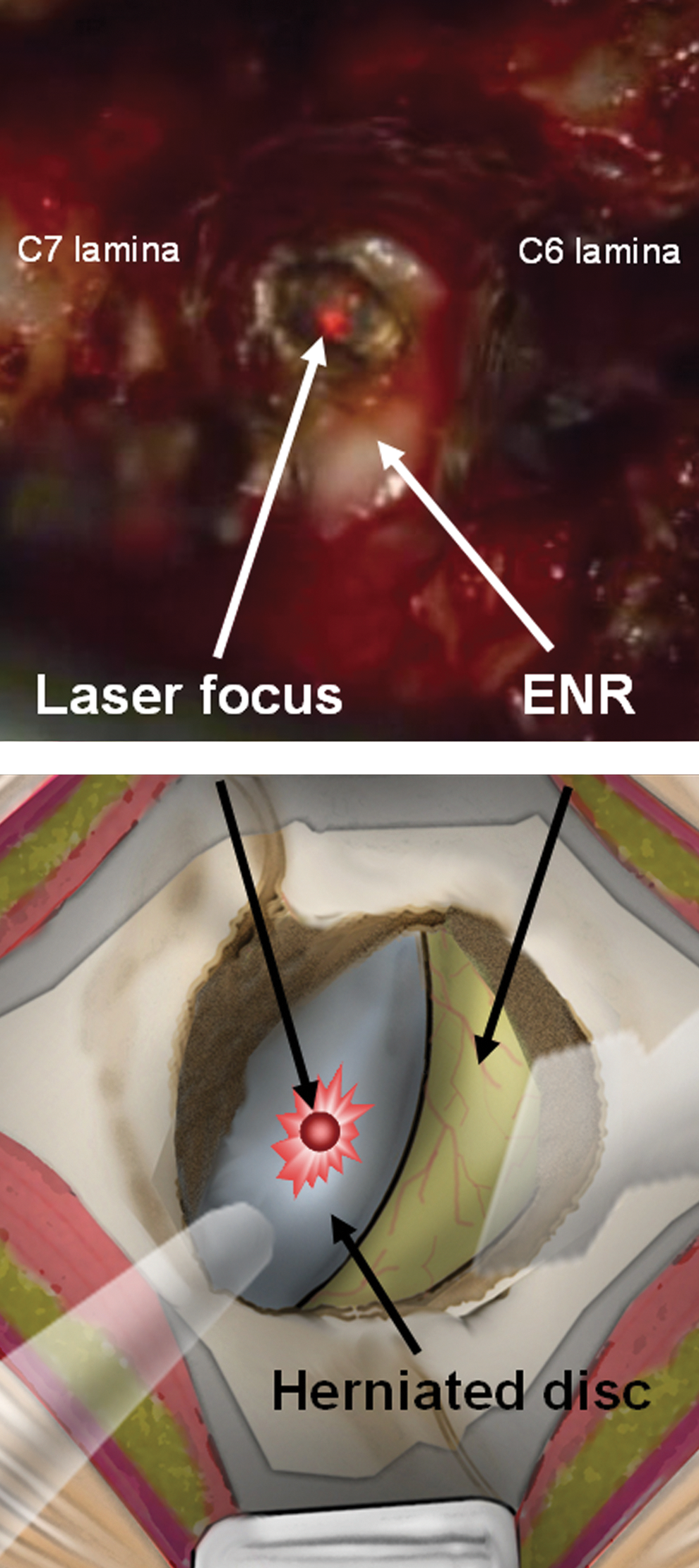
Intraoperative image and illustration. Intraoperative microscopic image (upper) and corresponding drawing (lower) demonstrating the anatomy of the foraminal region. Note the herniated disc, exiting nerve root (ENR), and pointed CO2 laser beam.
Results
Demographics
The mean age of the 24 patients in the laser PCFD group was 50.7 years (range, 33–77 years) and that of the 23 patients in the conventional PCFD group was 54.7 years (range, 37–75 years). The mean follow-up period of the laser PCFD group was 27.6 months and that of the conventional PCFD group was 32.5 months. There was no significant difference between groups for sex ratio, age, or symptom duration. The treated level was C4-5 in 4 patients, C5-6 in 19 patients, C6-7 in 29 patients, and C7-T1 in 8 patients. The demographic data are presented in Table 1.
PCFD, posterior cervical foraminotomy and discectomy.
Surgical outcomes
Estimated blood loss values were significantly lower in the laser PCFD group than in the conventional PCFD group (p<0.05; Table 2). Mean blood loss and blood loss per level for the laser PCFD group were 161.0 and 128.8 mL, respectively. Mean blood loss and blood loss per level for the conventional PCFD group were 223.9 and 171.7 mL, respectively. The mean values for operative time and hospital stay were lower in the laser PCFD group than in the conventional PCFD group, but the differences were not statistically significant.
PCFD, posterior cervical foraminotomy and discectomy.
Clinical outcomes
The mean (±standard deviation) VAS score for radicular arm pain improved from 7.42±2.45 to 1.83±1.31 in the laser PCFD group and from 8.30±1.40 to 1.65±1.40 in the conventional PCFD group. The mean VAS score for neck pain improved from 4.67±3.31 to 1.29±1.40 in the laser PCFD group and from 5.61±2.82 to 1.09±1.65 in the conventional PCFD group. The mean NDI improved from 47.00%±20.93% to 10.46%±11.99% in the laser PCFD group and from 53.86%±24.53% to 10.02%±11.57% in the conventional PCFD group. Based on the modified MacNab criteria, the final outcome was found to be excellent or good in 21 of the 24 patients (87.5%) for the laser PCFD group and in 20 of the 23 patients (86.9%) for the conventional PCFD group. Differences between the groups in terms of clinical outcomes and pain scores were not statistically significant (Table 3). With regard to complications, one dural tear that required intraoperative primary repair and two cases of transient dysesthesia that recovered within 6 months were reported in the conventional PCFD group. One case of transient dysesthesia was reported in the laser PCFD group. There was no case of postoperative infection, recurrence, or postoperative segmental instability. Neither of the groups included reoperation cases during the follow-up period. Even in cases with an unfavorable outcome, the patients were treated with nonoperative management options such as medication, physical therapy, and cervical epidural blockade.
PCFD, posterior cervical foraminotomy and discectomy; VAS,visual analogue scale.
Discussion
Potential advantages and disadvantages of PCFD
Posterior cervical foraminotomy has several advantages compared with anterior cervical discectomy and fusion (ACDF) surgery, which is considered the gold standard technique for the treatment of cervical disc disease. 1,3,12 –15 First, a direct posterior approach offers excellent visualization of the intended foraminal area and cervical nerve root. Second, avoidance of a fusion procedure can maintain the functional motion segment and thus minimize adjacent segment disc degeneration and avoid postoperative neck immobilization. Third, it avoids the anterior approach and thus prevents anterior complications such as recurrent laryngeal nerve injury, Horner's syndrome, esophageal injury, carotid injury, and graft-related complications. Finally, it enables treatment of several spinal motion segments via multilevel foraminotomy.
There are, however, some disadvantages of conventional PCFD: postoperative neck pain with foraminotomy; the need for neural retraction; an inability to address central disc herniation; slightly more cumbersome positioning; and risk of instability 16,17 or recurrence, 18 although it is low. Among these disadvantages, the most troublesome disadvantage is that the nerve root cannot be retracted with ease, thus limiting exposure of the disc space. The route of the cervical nerve root is horizontal and overhangs the disc space. Therefore, neural retraction may be not sufficient to expose and remove the herniated disc fragment and achieve thorough decompression. Furthermore, the foraminal window and disc space are relatively narrower than those in the lumbar area. The extent of facet joint resection is also limited to <50%, to avoid postoperative cervical instability. Therefore, the surgical field is limited, and it may be difficult to achieve decompression using standard disc forceps.
Advantages of laser-assisted PCFD (Fig. 2 )
The use of a microscopic CO2 laser can solve these problems. First, the pinpoint laser scalpel enables selective discectomy with minimal neural retraction. In spine surgery, use of a laser has benefits over use of a mechanical scalpel in terms of precision. 7 The long wavelength of the CO2 laser (10.6 μm) has high absorption in tissue and water, with rapid conversion of light energy into heat in a small volume of tissue. 19 This profile makes the CO2 laser an excellent cutting tool, as it causes minimal thermal damage to adjacent tissue; however, this profile limits its ability to coagulate large vessels. 20 The diameter of the focused beam of a CO2 laser is <0.5 mm, whereas the width of small disc forceps is ∼5 mm. This small spot size enables selective tissue ablation in a narrow surgical bed. Second, a laser scalpel can also effectively ablate bony stenosis or osteophytes. The vertical direction of the laser beam tangentially evaporates excessive bone growth compressing the neural tissues. Finally, sophisticated tissue dissection is possible without damage to the neural elements. Inflammatory fibrous adhesion or even scarring from a previous operation can be dissected using a CO2 laser. The use of a laser may reduce the risk of dural breach, intraoperative bleeding, swelling, and trauma to normal tissues. 7
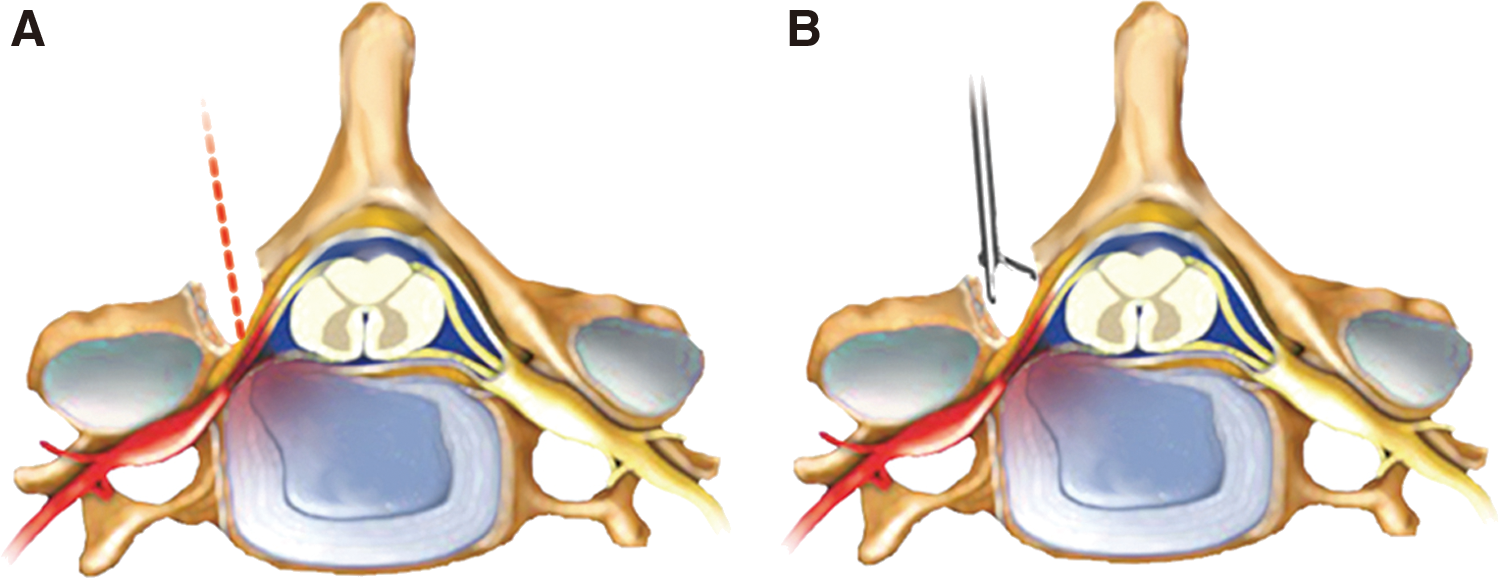
Schematic comparison of laser-assisted posterior cervical foraminal discectomy and conventional posterior cervical foraminal discectomy. The pinpoint laser scalpel enables selective discectomy with minimal neural retraction.
A laser can be used to remove herniated disc material or osteophytes, and reduce intradiscal pressure by vaporization. 8,21,22 We have performed CO2 laser-assisted microscopic surgeries for lumbosacral spinal disease since 1991, and the use of laser microdiscectomy for treatment of lumbar disc disease has been reported previously. 5 –7 However, very few studies have reported the use of a CO2 laser for cervical spinal surgery. 23 To the best of our knowledge, this is the first case series report on the use of a CO2 laser in PCFD.
Clinical outcomes and operative data
In our series, 98% of the patients exhibited clinical improvement. This result is comparable to that of previous studies. 3,18,24 There were no statistical differences in various clinical outcomes between the groups. However, the operative data showed definite differences. Estimated blood loss was less in the laser PCFD group; differences in both total blood loss and blood loss per level were statistically significant. Intraoperative bleeding is a major technical problem during posterior cervical foraminotomy because of the engorged epidural veins in the foraminal area. 25 Massive intraoperative bleeding may hinder effective foraminal decompression and affect the operation time and postoperative recovery. Although the difference between the two groups did not achieve significance, the operation time and hospital stay tended to be shorter for the laser PCFD group than for the conventional PCFD group. The reduced intraoperative bleeding in the laser PCFD group could be attributed to selective discectomy with less manipulation of the surrounding vascular tissues. As mentioned previously, the CO2 laser enables thorough fragmentectomy via a narrow cervical foraminal corridor without over-retraction of the nerve root or excessive removal of the facet joint, while preserving spinal stability and preventing postoperative neck pain. Decompression with mechanical tools in a limited surgical field can result in dural injury, with cerebrospinal fluid (CSF) leakage being the most commonly reported complications of this technique. 1,26,27 In the present study, there was only one case of dural tear requiring repair in the conventional PCFD group, whereas no cases of dural breach occurred in the laser PCFD group. One of the possible complications of laser discectomy is laser-induced thermal injury to the neural tissues, which can result in motor weakness or postoperative sensory changes. Only one patient in the laser PCFD group complained of mild dysesthesia in the arm and fingers, which spontaneously improved within 6 months. Theoretically, the thermal conduction of a CO2 laser is minimal; therefore, the risk of thermal injury by conduction to neighboring neural tissues is negligible. 20 Another possible complication related to the CO2 laser is the potential for vascular damage caused by the laser during discectomy. 5 However, none of our patients experienced laser-related vascular complications. Avoiding focusing the laser on the surface of critical structures and inserting a small amount of saline at the bottom of the intradiscal space during use of the laser can prevent the occurrence of such a complication. 5 Posterior foraminotomy involves partial resection of the facet joint to achieve nerve root decompression. Studies have shown that there is an increased risk of instability if >50% of the facet joint is removed. 17 No patient developed significant segmental instability requiring subsequent fusion surgery during the follow-up period. The preservation of stability may be attributable to the precision of laser-assisted decompression, which enabled effective foraminotomy while avoiding excessive removal of the facet joint and lamina; however, long-term follow-up is necessary to make definitive conclusions.
This is the first study to evaluate the clinical outcomes of CO2 laser-assisted posterior cervical microdecompression. To evaluate the definitive effectiveness of this novel technique, a randomized controlled trial with a long-term follow-up period is necessary in the future.
Conclusions
PCFD is an effective surgical option for the treatment of cervical radiculopathy. A CO2 laser can be used as a sharp cutting tool in a narrow surgical field and may improve efficiency by reducing intraoperative bleeding, operation time, and risk of tissue damage.
Footnotes
Acknowledgment
This study was supported by a grant from the Wooridul Spine Hospital.
Author Disclosure Statement
No conflicting financial interests exist.