
Abstract
Introduction
Although the exact underlying pathophysiology of RAS is not entirely clear, some evidence proposes that aphthous ulcers are related to a focal immune dysfunction in which T lymphocytes have a major role. 1,2 Many etiologic, predisposing, and precipitating factors, such as genetic factors, immunologic problems, trauma, hypersensitivity to foods and drugs, hormonal changes, hematologic deficiencies, cessation of smoking, psychological stresses, and viral infections are suggested. 2,4
There is no curative treatment available for RAS. A wide variety of topical and systemic agents have been suggested for the treatment of recurrent aphthous ulcers, such as topical corticosteroids; topical antimicrobials and anti-inflammatoryagents; topical analgesics; and systemic immunosuppressive agents such as systemic corticostereoids, azathioprine, levamisole, colchicine, thalidomide, pentoxifylline, dapsone, cimetidine, cyclosporine, cyclophosphamide, infliximab, and etanercept. In addition, local physical treatments have been used such as surgical removal, debridement, low dense ultrasound and physical barriers. 1 As there is no consensus regarding the cause of RAS, it is difficult to have completely effective treatment or prevention. 2 There are currently few agents that have been found in randomized controlled trials to be definitely effective in the management of RAS. 1 The goals of therapy are threefold: (1) to control the pain of the ulcer, (2) to promote ulcer healing, and (3) to prevent recurrence. 1,2
Recently, a few reports showed the merits of CO2 laser application in a non-thermal, non-ablative manner as a low power laser to reduce pain in aphthous ulcers. Pain relief was rapid and long term. 5 –7 In a case report, aphthous ulcers of two patients were irradiated with CO2 laser at 1.0–1.5 W power, with a defocused handpiece for 5 sec. Before laser irradiation, a thin film of elmex gel (a transparent gel with high water content) was placed on the lesion to reduce the beam absorption by the soft tissue. Anesthesia was not required, as the treatment was not painful. The patients reported immediate pain relief after laser irradiation. 5
In another study, the analgesic effect of a single session of non-ablative CO2 laser therapy was evaluated in minor aphthous ulcers as a prototype of painful oral ulcers. 6 Fifteen patients, each with two discrete minor aphthous ulcers, completed the RCT. In this RCT, before laser irradiation, a thick layer of transparent, non-anesthetic gel (Abzar Darman Co., Iran), with high water content (87.5%) was placed on both the laser-treated and placebo-treated lesions. The lesions in the laser group were irradiated with CO2 laser (1 W of power in defocused continuous mode, scanning rapidly over the lesion with circular motion for 5–10 sec) through the gel, with a technique that was called non-ablative CO2 laser therapy (NACLT) afterwards. The results of this RCT showed that a single session of non-ablative CO2 laser irradiation could reduce pain in miRAS immediately and significantly (p<0.001), with no visible side effects. The analgesic effect was sustained during the 4 day follow-up periods. The procedure was pain free and did not require anesthesia. The results of power metering and thermometery showed the low power, phototherapeutic nature of the applied CO2 laser in NACLT. 6
In another pilot study, the analgesic effect of NACLT was evaluated in five patients with major recurrent aphthous ulcers. The results of this RCT study suggested that a single session of NACLT could reduce pain in major aphthous ulcers immediately and significantly (p<0.001), without any visible side effects. 7 This study is in progress.
After the primary evidence of pain-relieving properties obtained by NACLT in reducing pain in some painful oral lesions such as recurrent aphthous stomatitis, 8 we decided to evaluate whether this technique could accelerate the healing period of oral lesions.
In this RCT, our objective was to evaluate the effects of a single session of non-thermal, NACLT in reducing the healing period of minor oral aphthous ulcers.
Materials and Methods
Study design
The study was designed as a placebo-controlled, clinical trial. The RCT protocol approval was obtained from the Clinical Ethics Committee of Tehran University of Medical Sciences branch of Academic Center for Education, Culture and Research (ACECR), Iran prior to patient recruitment.
Patient selection
Complete clinical and laboratory investigations were conducted for all patients before they enrolled in the study. They were carefully examined by a dermatologist and necessary laboratory tests were performed in order to rule out underlying diseases. In addition, a pathergy test was performed and the patients were visied by an ophthalmologist in order to rule out Behcet's disease.
An initial questionnaire was filled for every patient before the procedure. A record of the name, age, sex, duration of ulceration, and size of ulcer (the largest dimension in mm, measured with a ruler) was made.
The inclusion criteria were as follows
The exclusion criteria were: age <12 years, pregnancy, any known systemic disease that could predispose the patient to miRAS, treatment of their current ulcers with any form of topical medications, or history of receiving any systemic treatment known to have any effect on RAS within the previous 3 months.
A detailed explanation of the experimental nature of the study and the whole process was given to the patients. If the subjects agreed with the conditions, informed consent was obtained.
Study procedure
For all patients, one of the aphthous ulcers was randomly allocated to be treated with NACLT while the other one served as placebo. Before irradiation, a layer of transparent, non-anesthetic gel (Abzar Darman CO. Iran) with high water content (87.5%) was placed on both of the laser-treated and placebo-treated lesions. Before laser treatment, patients and surgical staff were given appropriate protective eye shield and eye glasses matched to the laser wavelength (10,600 nm) to protect against inadvertent laser impacts. In order to irradiate the laser lesions by NACLT technique, the CO2 Laser (λ=10600 nm; Lancet-2, Russia) was operated at 1 W power with a defocused hand piece at 5–6 mm distance from the mucosal surface, in continuous mode, scanning rapidly over the lesion with circular motion for 5–10 sec. In any patient the placebo lesion was irradiated with the same laser, but with an inactive probe. The procedure was pain free and did not require anesthesia. No cooling system was used before and/or after NACLT.
The patients were visited every other day by a blinded physician. The outcome variable included the time needed for complete re-epithelialization of the ulcers. Any adverse reactions were recorded by the evaluator.
Statistical analysis
Data were analyzed using SPSS version 13. The results were expressed as mean±standard deviations. Statistical significance was tested using the Student's t test. The level of statistical significance was set at a two-tailed p-value of 0.05.
Results
Ten patients (one man and nine women), with 20 minor aphthous ulcers recruited in the study. The patients' age ranged from 22 to 56 years, with an average of 35.6 years. The duration of lesions before enrolling in the study, were 2.2±0.42 and 2.5±0.71 days in laser and placebo groups, respectively, and there was no significant difference between study groups (p=0.26). There was no significant difference in the size of lesions between the study groups (4.4±1.7 mm in laser group versus 4.4±1.4 mm in placebo group). Healing time after treatment were 4.8±2.4 day in the laser group and 7.6±2.5 day in the placebo group, which was statistically significantly shorter in laser group (p=0.02) (Fig. 1). There was no visible side effect such as ablation, ulceration, or erythema following NACLT. The patients reported no warmth in their lesions during laser treatment.
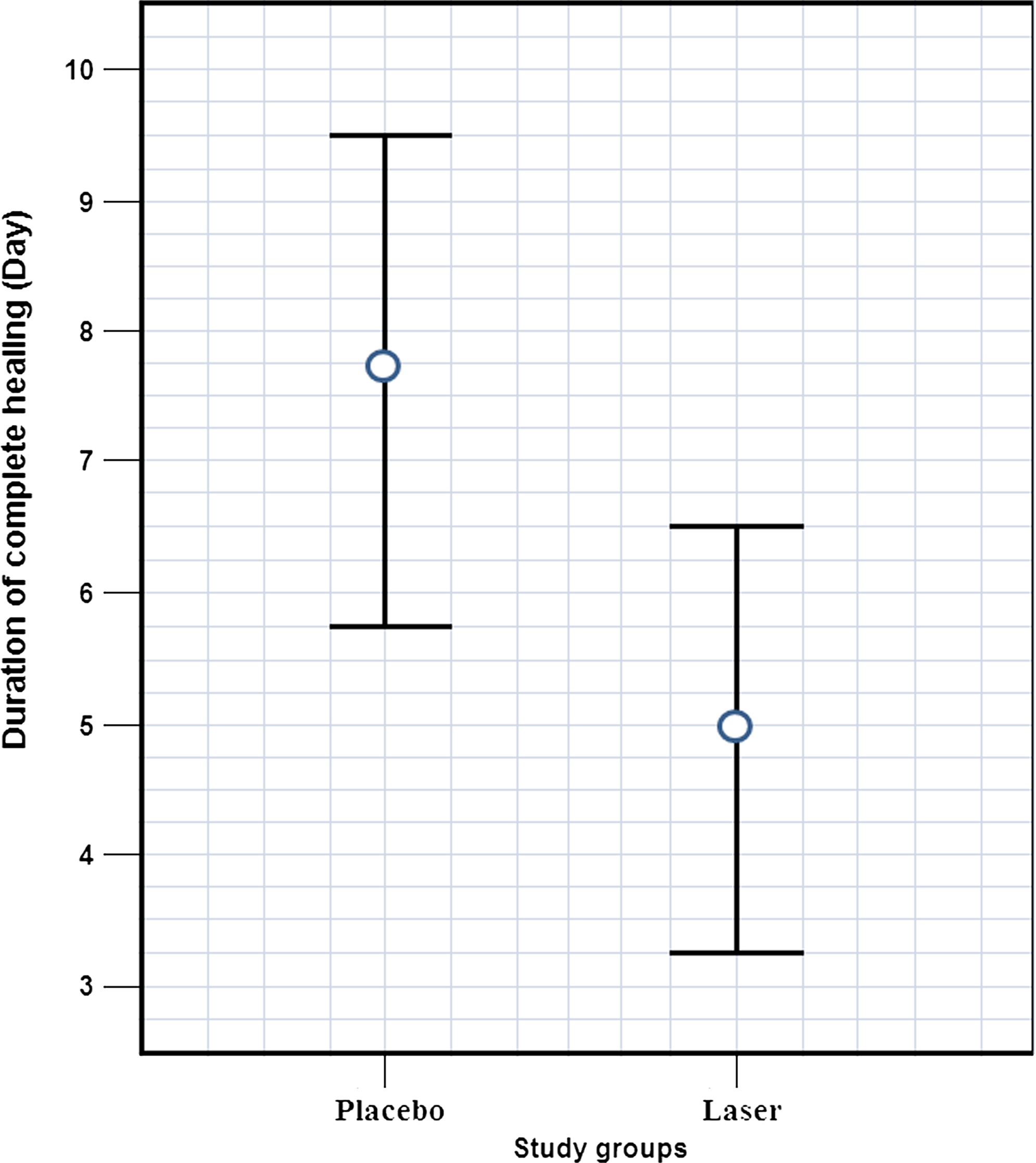
Comparison of healing time between study groups.
Discussion
The results of this RCT suggested that a single session of non-thermal, NACLT could be used to promote wound healing in minor aphthous ulcers (p=0.02). There were no visible side effects or aggravation of the lesions following NACLT of the aphthous ulcers. The procedure was painless and did not require anesthesia.
In order to use the conventional, high-power CO2 laser as a low-power, non-thermal, phototherapeutic laser for NACLT, the CO2 laser beam was irradiated through a thick layer of transparent, non-anesthetic gel with high water content. In addition, the CO2 laser was operated with a defocused handpiece, scanning rapidly over the lesion with a circular motion. With these considerations, CO2 laser has been applied as a non-destructive, non-thermal, phototherapeutic laser (NACLT) to reduce pain in some oral mucosal lesions. 6 –9 In these studies, the analgesic effect has been instant and significant (p<0.001), so that after NACLT, the patients in these studies have been able to eat and drink easily at once. Up until now, in the series of NACLT studies, we have not observed any visible side effects following careful performance of the technique. 8
This RCT was designed to evaluate whether NACLT had any promoting effects on the healing process of minor aphthous ulcers. The results of this RCT suggest that NACLT could be used to promote wound healing in minor aphthous ulcers as well (p=0.02), although its healing effects are not as significant as its pain relieving effects (p<0.001).
In our previous studies, the results of powermetery showed that in NACLT, the resultant laser power output after passing through the gel, was 2–5 mW. Thermometery also showed no significant temperature rise on the surface of the ulcers, under the gel layer, during laser irradiation, supporting the low power nature of the applied CO2 laser in NACLT. 6 It seems that as the gel has high water content, it absorbs CO2 laser irradiation considerably; therefore, the power output drops notably (200–500 times) after irradiation through the gel. In fact, by irradiation of CO2 laser through a transparent gel, with high water content (NACLT) CO2 laser can be used as a low-power, photobiomodulative laser. 6
There are perhaps three main areas of medicine where low-level laser therapy (LLLT),,also known as “low intensity laser therapy,” “phototherapy,” “cold laser therapy,” “photobiostimulation,” and “photobiomodulation,” has major roles to play. These are (1) pain relief, (2) promoting wound healing and tissue repair, and (3) relief of inflammation. 10
There have been numerous reports in the literature over the last 30 years that LLLT with various optical parameters can stimulate wound healing and tissue repair in both animals and humans. 10 –14 Despite many reports of positive findings from experiments conducted in vitro, in animal models and in human studies, LLLT remains controversial. 15,16 This is likely for two main reasons; first, the exact biochemical mechanisms underlying the positive effects are not completely understood, and second, the complexity of the parameters involved in LLLT such as wavelength, total fluence, fluence rate, coherence, pulse structure, or continuous wave and polarization state has led to the publication of a number of negative studies as well as many positive ones. In addition, a biphasic dose response has also complicated these controversies. Biphasic dose response is observed where low levels of laser/light have a much better effect on stimulating and repairing tissues than higher levels of laser/light. 10,15,17,18
The cellular responses observed in vitro after LLLT, which can explain the stimulating effects of LLLT, can be broadly classed under increases in metabolism, migration, proliferation, increases in synthesis and secretion of various proteins, and modulating the production of growth factors and cytokines. 10,19 Some studies on a cellular level report an increase in proliferation of various skin cell types, including fibroblasts, endothelial cells, and keratinocytes. 15,20 –25 It has been suggested that LLLT stimulates cell growth directly by regulating the expression of specific genes, as well as indirectly by regulating the expression of the genes related to DNA synthesis and repair, and cell metabolism. 10,26 It has been suggested that LLLT can induce the expression of cytokines and growth factors known to be responsible for the many phases of wound healing, including increased interleukin (IL)-1 and IL-8 in keratinocytes, 27 which are the cytokines responsible for the initial inflammatory phase of wound healing, upregulating cytokines responsible for fibroblast proliferation and migration, increase in growth factors such as vascular endothelial growth factor (VEGF) responsible for the neovascularization necessary for wound healing, 28,29 and upregulation of transforming growth factor (TGF)-β, a growth factor responsible for collagen synthesis from fibroblasts. 30
On the other hand, low power photobiomodulative lasers have anti-inflammatory effects as well, including the activation of suppressor T lymphocytes and the modulation of the secretion of cytokines and inflammatory mediators such as histamine, kinin, and tumor necrosis factor, which seem to lead to a reduction in the inflammatory response. 31 –33 Studies have shown elevated levels of interferon (IFN) γ, tumor necrosis factor (TNF)-α, and interleukins 2, 4, and 5 in aphthous ulcers. 34 RAS can be prevented by treatments that involve the synthesis of endogenous TNF-α, such as thalidomide and pentoxifylline. 35 Low-power lasers can modulate the levels of some other cytokines and pro-inflammatory mediators, such as interleukins, TNF-α, IFN-γ, and TGF-β; 33,36 –42 however, their effects on aphthous ulcers have not been definitely established. 43
We do not know whether the mechanisms by which NACLT promotes wound healing in aphthous ulcers are the same as those of classical low-power lasers, or not. Further basic studies are necessary to elucidate this question.
Although in this study, we used eye glasses matched to the CO2 laser wavelength (10,600 nm), we presume that it might be much safer to use eye glasses matched to both the 10,600 nm and the guiding beam to protect the eyes from the reflected beam from the surface of the gel.
Conclusions
In conclusion, this RCT suggested that NACLT could be used to accelerate wound healing in minor aphthous ulcers without visible side effects, although its analgesic effects are much more significant than its healing effects. Certainly, controlled clinical trials with larger sample sizes will more definitely be able to demonstrate the wound healing effects of NACLT in minor aphthous ulcers.
Footnotes
Acknowledgments
This study was funded by the research deputy of the Academic Center for Education, Culture and Research.
Author Disclosure Statement
No competing financial interests exist.