
Abstract
Introduction
Among the theories that have been proposed to explain CDH, such as the odontoblastic transduction theory 3,4 and the dentin innervation theory, 5 the hydrodynamic theory of Brännström 6 is the most widely accepted. This theory suggests that thermal, chemical, or mechanical stimuli induce rapid displacement of dentinal fluid. A shift in fluid in either direction can deform the odontoblast layer or stimulate nerve fibers and cause pain.
CDH symptoms are relieved using treatments that aim to decrease the diameter of dentinal tubules or occlude them, stimulate secondary dentin production, desensitize nerve fibers, or a combination of these methods. As a result, the market now offers a correspondingly diverse range of products: dentifrices or gels that contain fluoride (F) or other desensitizing agents (e.g., KNO3. 7 SnF2, 8 oxalates 9 ), formaldehyde, 10 and bonding agents, 11 . Laser irradiation 12 has also been applied alone or combined, to produce variable results. NaF is used widely, yielding predictable positive results in many cases. 13 Additionally, iontophoresis has been shown to increase the uptake of F. 14
A novel treatment has been developed to treat CDH. In NovaMin® (NM) (Denshield, NovaMin® Technology, FL), the active ingredient is a bioactive glass that has been ground into a fine particulate with a median size of <20 μm, composed of Ca, P, Na, Si, and O. When exposed to an aqueous environment, it releases Ca+2 and (PO4)-3 ions. Na ions in the particles exchange with H cations, which allows the Ca and (PO4)-3 ions to be released. A calcium phosphate layer then forms and crystallizes as hydroxylapatite. The chemical reaction that leads to hydroxylapatite is:
The physical occlusion of dentinal tubules results from both the hydroxylapatite layer and the residual NM particles, which is claimed to relieve hypersensitivity. 1,2 Farmakis et al. demonstrated the efficacy of bioglass treatment in combination with Nd:YAG laser irradiation. 17
In this study, the efficacy of NM paste, various power settings of Nd:YAG laser irradiation and their combination was evaluated in vitro by environmental scanning electron microscope (ESEM) to assess the percentage of occluded dentinal tubuli orifices, as potential treatments for CDH.
Materials and Methods
The study was conducted on extracted, impacted human molars. The protocol was approved by the ethics committee of the Dental School of the University of Athens. Informed consent was released by all patients. In total, 49 sound, recently extracted impacted human molars were collected. Any surrounding soft tissues were removed by immersion in 2.5% NaOCl solution for 10 min. The teeth were then stored in sterile saline (0.9% NaCl) until use. The cervical enamel of the buccal and lingual surfaces was removed exposing the underlying dentin using a diamond disc (Isomet 11–1180, Buehler Ltd, Evanston, IL) under tap water spray. The buccal area served as the experimental specimen, while the lingual area served as the control. Specimens were assigned randomly into seven equal groups. All specimens had the smear layer removed by ultrasonication in deionized water for 30 sec, followed by application of 0.5 M ethylenediaminetetraacetic acid (EDTA) (pH 7.4) for 2 min and a rinse by water spray for 30 sec. 18 This procedure was performed to create the patent tubules that are observed in clinical cases of CDH.
The presence of a smear layer positively influences the percentage of DOO after administration of NM and Nd:YAG laser irradiation. 17 Therefore, all experimental surfaces of all groups (A–G) were treated by one short passage of medium blue polishing Sof-lex discs (3M/ESPE, USA), followed by a 1 min water spray rinse to create a smear layer on all specimens, because the presence of a smear layer positively influences the percentage of DOO after administration of NM and Nd:YAG laser irradiation. 17
NM paste was prepared on site according to manufacturer's guidelines. For the Nd:YAG laser irradiation (Smartfile, DEKA M.E.L.A. SRL, Calenzano, Italy) the laser hand piece was securely mounted on a stand to allow a constant distance of the fiberoptic (0.3 mm in diameter) to the treated surface. Each specimen was mounted on a microscope observation glass slab and moved manually at ∼5 mm/sec in a sweeping motion, covering the total surface, 19 resulting in an overall irradiation time of 30 sec per sample. The treatment sequence of the groups was as follows: Groups A and B received NM for 5 min, rinsing with a water spray for 10 sec, followed by L (0.5 W/10 Hz/50 mJ and 1 W/10 Hz/100 mJ, respectively); groups Cand D received L (0.5 W/10 Hz/50 mJ and 1 W/10 Hz/100 mJ, respectively) followed by NM; group E received NM; groups F and G received L (0.5 W/10 Hz/50 mJ and 1 W/10 Hz/100 mJ, respectively) (Table 1).
Next, all specimens were stored in sterile saline (0.9% NaCl) for 24 h at room temperature, then assessed under an ESEM XL 30 (Phillips, Preston, VA) in generic stream encapsulation (GSE) mode using 1000× and 3000× magnification. Photographs were taken. Each specimen was evaluated with regard to the percentage of occluded dentinal orifices on a scale of 1 to 4 (1: 0–24%, 2: 25–49%, 3: 50–74%, and 4: 75–100%). There were four blinded evaluators, three of whom had to agree for a score to be recorded.
Statistical analysis
The distribution of DOO by group was summarized in a two way table of absolute and relative frequencies. For descriptive purposes, mean DOO scores (±1.96 SD) were also graphed. Overall differences in DOO score by group were examined by exact test, because of the small sample size.
The sample size was estimated as follows: assuming seven groups with average percentages for scores 1, 2, 3, and 4 ranging progressively from 52%, 23%, 16%, and 9% for group 1 (corresponds to a mean score of 1.83) to 1%, 4%, 12%, and 83% for group 7 (mean score 3.79) and an analysis performed via a global exact test for independence of proportions (i.e., ignoring the order of scores), the power to detect such a difference at an α level of 0.05, using seven specimens per group, was 79%. Post-hoc calculations based on the observed score distribution and the current design led to an estimated power of 98.4% at an α level of 0.05.
Kendall's tau-c was used for post-hoc pairwise comparisons between groups. The specific statistic and the corresponding test were chosen because tau-c is a measure of association between ordered categorical variables. When focusing on pairwise comparisons, the “group” variable had only two levels (therefore it could be considered ordered) and score was an ordered variable also.
The intra- and inter-evaluators' agreement were assessed through the weighted version of Cohen's κ, which is suitable for ordinal data. The estimated values of κ for all pairwise comparisons of the four raters ranged from 0.96 to 1.00 with the proportion of agreement ranging from 98.6% to 100.0%. Similarly, values of κ for test–retest agreement of the same rater were >0.96 for all raters, with the proportion of agreement being >98.6% in all cases.
Results
The DOO results by group are summarized in Table 2 and representative pictures are shown in Fig. 1. One specimen in group B was ruined during the handling and observation by ESEM, immediately prior to being photographed; despite receiving the highest score, the observed remnants were recorded as a missing value, leaving group B with six specimens. The treatment modality significantly affected DOO (p=0.012), group B showing the best performance (mean 4,0 [SD 0,0]), closely followed by group G (mean 3,9 [SD 0,4]). All other groups ranged below these values as summarized in Table 2.

Combined photograph of all experimental groups (×1000 magnification).
Mean (±1.96 SD) DOO scores are shown given in Figure 2. Scores in groups B and G were significantly higher than the combined results of groups A, C, D, E, and F (Kendall's tau-c [p-value] 0.357 [0.004] and 0.342 [0.007], respectively). The difference between groups B and G was not significant (p=0.440).
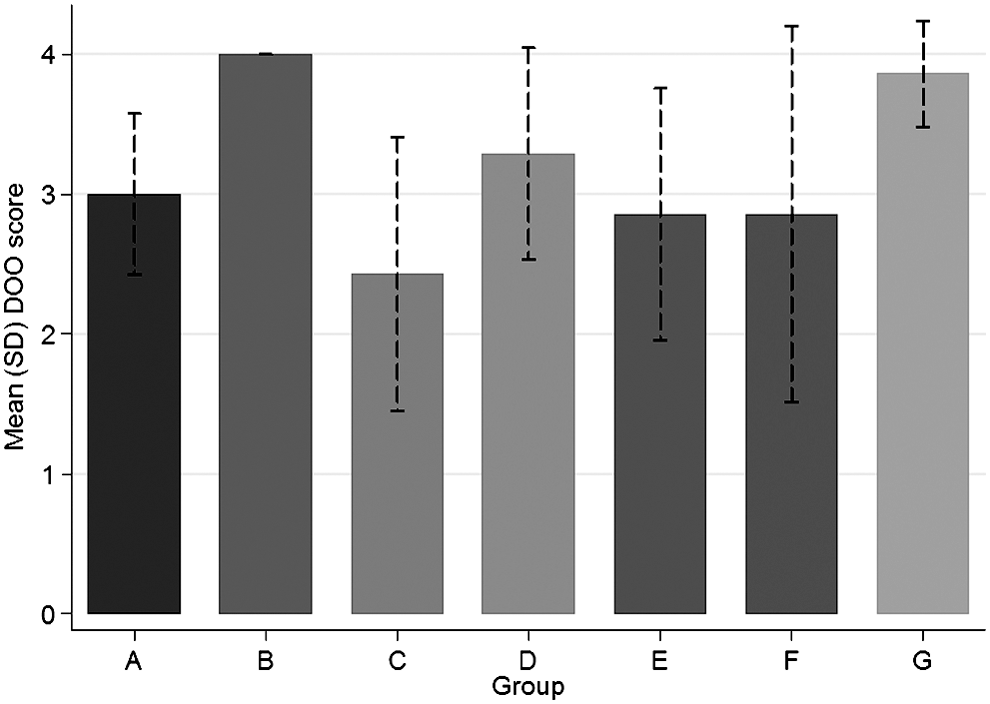
Mean (standard deviation) of dentinal orifice occlusion (DOO) score by group (bar chart).
Treatment modality significantly affected DOO (p=0.012). Groups B and G achieved higher DOO scores than the other groups. By ordinal logistic regression (with bootstrap standard errors), the combination of NM paste, followed by 1 W Nd-YAG laser irradiation (group B), significantly (p<0.001) contributed to DOO compared with groups C, E, and F.
Additionally, a granular layer was observed in many areas of the experimental surfaces of specimens in groups B and D.
Discussion
CDH is observed frequently among adults, especially following periodontal treatment. The dentin becomes permeable because of the exposure of the dentinal tubules that run through from the enamel or cementum to the pulp. The tubules vary in quantity and diameter, based on the location that is examined, that is, decreasing from 45,000/mm2 at the pre-dentin border to 20,000/mm2 at the dentin–enamel junction. 20
Deposition of peritubular dentin reduces dentin permeability during aging. In CDH, dentinal tubules are increased in number and diameter compared with normal teeth. 21 Treatments aim to decrease their diameter, occlude them, and/or desensitize the nerve fibers. Of all applied clinical modalities, none have proved superior and permanent.
Laser irradiation was introduced as a treatment for CDH in clinical practice in 1985. 21 –23 Two types of lasers with different power settings have been used with varying levels of success: (1) low-power lasers (e.g., diode, 24 Ga-Al-As 25 ) and (2) medium-power devices, such as CO2 26 and Nd:YAG 23,27 The effect of laser treatment in CDH can be explained by three mechanisms: sealing of dentin tubules, analgesia of dental nerves, or a placebo effect. 28
Both pulsed and continuous wave low-level lasers are used in the treatment of CDH. The effectiveness varies between 55% and 100%. The exact mechanism of He-Ne-lasers is not completely known. He-Ne laser irradiation does not influence group A or group C nerve fiber nociceptors. 29
An electric potential is generated, however, which increased 33% after a single transcutaneous laser irradiation. 30 This gain of the action potential could be verified even 8 months after laser treatment by Rochkind et al. 30
Gallium, aluminium, arsenid (GaAlAs) diode lasers are also used for treatment of CDH, emitting three different wavelengths: 780, 830, and 900 nm. 31
For low-output power lasers (e.g., diodes and He-Ne lasers), the desensitization is attributed to laser activity at the nervous level 32 or based on the therapeutic response of odontoblasts to low-level laser therapy (LLLT). Pereira et al. demonstrated that LLLT influenced the behavior of odontoblast-like cells in a significant way. 33
A recently published literature review (including publications from 1923 to 2010) on the enhancement of cell proliferation agrees that, with the appropriate use of LLLT, the proliferation rate of cultured cells, including stem cells, can be increased. The results of LLLT vary according to the applied energy density and wavelengths to which the target cells are subjected. This review suggests that an energy density value of 0.5–4.0 J/cm2) and a visible spectrum ranging from 600 to 700 nm of LLLT are very helpful in enhancing the proliferation rate of various cell lines. 34
Nd:YAG laser irradiation is purported to temporarily alter the ending of the sensory axons and block C and AB fibers. 35,36 Additionally, the specific laser irradiation melts the superficial layer of dentin. When re-crystalization occurs, the melted dentin seals the dentin tubules at a depth of 3–4 μm without associated cracked dentin surfaces. This effect is enhanced when used with fluoride-containing substances. 37,38 An in vitro study that utilized the aforementioned treatment, reported a 90% occlusion of the exposed dentinal tubules by SEM. 37 When the energy and power settings of the laser remain within the reported range (as used in this study), pulpal damage does not occur. 39
A recent systematic review concluded that laser therapy has a slight clinical advantage over topical medicaments in the treatment of dentin hypersensitivity, 40 although a placebo effect that contributes to the therapeutic outcome must be considered. 32
Bioactive glass (NM) has been introduced as a new treatment paradigm. Its proposed mechanism of action is a series of reactions that are initiated by the aqueous environment, leading to hydroxylapatite formation onto available nucleation surfaces, similar or identical to endogenous tooth and bone substances. 41
The presence of a smear layer appears to have a strong influence on effective tubular occlusion, possibly acting as a substrate with multiple nucleation sites, thus accelerating apatite formation. 17 Combination of the treatment modalities proved superior to each modality applied separately. The combined treatment utilizing NM application followed by laser irradiation (groups A and B) surpassed the DOO recordings of the combination laser irradiation followed by NM application (groups C and D). The groups using the combination NM/laser application (groups A [0.5 W] and B [1 W]) performed almost equally on DOO as groups F and G (0.5 W and 1 W laser irradiation alone). In this study, 0.5 W Nd;YAG laser irradiation was less effective in producing DOO than the 1 W energy level, in either treatment scheme. It may be that the laser energy applied is sufficient in achieving high DOO; however, the combined treatment modality resulted also in generating a layer that preliminary work reports to be firmly attached to the dentinal surface. 17 If this proves long lasting, it may serve as a better long-term device for the treatment of CDH than the 1 W treatment alone. This layer can be seen as a continuous source of Ca, P, and Na ions for hydroxylapatite formation, thus stabilizing the result.
Another recent in vitro study that incorporated CO 2 laser irradiation following bioglass application observed increased dentin–bioglass interaction, 42 but because energy levels did not vary, the optimum combination of laser intensity and DOO was not determined.
A preliminary investigation demonstrated that the layer in group E withstood storage for 6 months in sterile saline (0.9% NaCl), followed by 10 min ultrasonic bathing. 17
Future research should examine the penetration depth of the bioglass particles inside the dentin tubules, the chemical composition of the resulting “plugs,” and the achievable duration of DOO.
Conclusions
Under the experimental conditions and within the limitations of this study, we concluded that laser irradiation with 1 W Nd:YAG (alone or combined with NM) is superior to other treatment modalities with regard to DOO and holds promise as an effective clinical treatment for CDH.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.