
Abstract
Introduction
However, transurethral laser coagulation is a promising alternative method to control vesical bleeding in these patients. Ravi first reported that treatment of radiation-induced HC using Neodymium:YAG Laser is safe and effective, but that care still must be taken not to cause bladder perforation. 8
Another kind of laser, potassium-titanyl-phosphate (KTP) laser (532nm, Greenlight,™ American Medical Systems, USA) has been widely used in the field of urology in recent years, for disorders including benign prostatic phyerplasia, 9,10 nonmuscle invasive bladder cancer, 11 glandular cystitis, 12 and urethral stricture. 13 In 2007, Chapin et al. Initially reported excellent results using KTP laser to treat radiation-induced HC in seven patients. 14 Herein we report our initial experience of using Greenlight KTP laser coagulation to achieve hemostasis in patients with radiation hemorrhagic cystitis.
Materials and Methods
Patients
From September 2004 to February 2011, we used transurethral Greenlight KTP laser to control intractable hematuria secondary to radiation cystitis in 10 patients. Demographics of patients are shown in Table 1. All 10 patients presented with severe HC that was refractory to conservative therapy, which included adequate hydration, hemostatics, and clot evacuation. Two patients with massive hemorrhage required multiple transfusions. Data were collected with regard to laser time during procedure, laser energy used, operative time, catheterization time, hospitalization time, follow-up time, hematuria-free interval, and complications.
Operative technique
The patient was placed in the lithotomy position under spinal or general anesthesia. First, clots were evacuated by a 25.6 French resectoscope and an Ellik evacuator. The bladder was then inspected to define the extent of cystitis, and to locate bleeding areas. After that we changed to a 22 French laser resectoscope with the bladder filled with sterile normal saline. A side-firing laser fiber was then introduced via the side working channel of the scope. The blue triangle and red aiming beam on the tip of the fiber indicated the position of laser emission. The Greenlight laser therapy system is a 532nm KTP laser system. The power setting was limited to 20–30 W with a pulse duration of 40 ms. We used a noncontact technique to treat the target areas. This technique requires that the laser be 3–5 mm away from the bladder mucosa, with the laser fiber being kept in constant motion over the target to avoid any injury to the underlying structures.
We used two major steps to perform the laser procedure. First, the areas of active bleeding and oozing were coagulated. After all bleeding and oozing sites were coagulated, we performed the second step. The areas that did not bleed or ooze but were angry looking, which indicated the possible source of bleeding, were coagulated. We did coagulation with caution not to damage the normal surrounding urothelium. In patients with diffused mucosal involvement, only the bleeding or severely congested areas were treated. For patients with lesions around the ureteral orifice, we inserted a double J stent before coagulating the lesions, and removed the stent 1 month postoperatively. At the end, the bladder was inspected thoroughly to ensure that all bleeding had ceased. After the procedure, a three-way 20 French Foley catheter was left indwelling, and continuous bladder irrigation with normal saline was applied. The Foley catheter was removed and the patient was discharged within 2–4 days, if the hematuria remained arrested.
Operative time was defined as the duration from the insertion of laser resectoscope to the indwelling of the Foley catheter. The laser time referred to the cumulative time that laser was activated by the foot pedal.
Follow-up investigations
Patients underwent cystoscopy after 3 months, to investigate the state of the bladder mucosa. Therapeutic efficacy was evaluated every 3 months in the first year and then semi-annually, up to 36 months.
Results
Control of bleeding was achieved in all 10 patients. Six patients had bleeding spot-localized to one or more walls, whereas the other four patients had the entire bladder involved. Application of laser to the bleeding spot resulted in mucosa blanching and immediate hemostatis (Fig. 1). For the two patients who had lesions near the ureteral orifice, double J ureteral stents were implanted before coagulation, and were removed 1 month postoperatively. Mean operative time was 24 min (19–45 min), mean laser time was 10 min (6–20 min), mean laser energy used was 16.38 kJ (7.32–36.18 kJ) (Table 2). No patient experienced bladder perforation, obturator nerve reflex, transurethral resection syndrome, bowel injury, or damaged ureteral orifice.
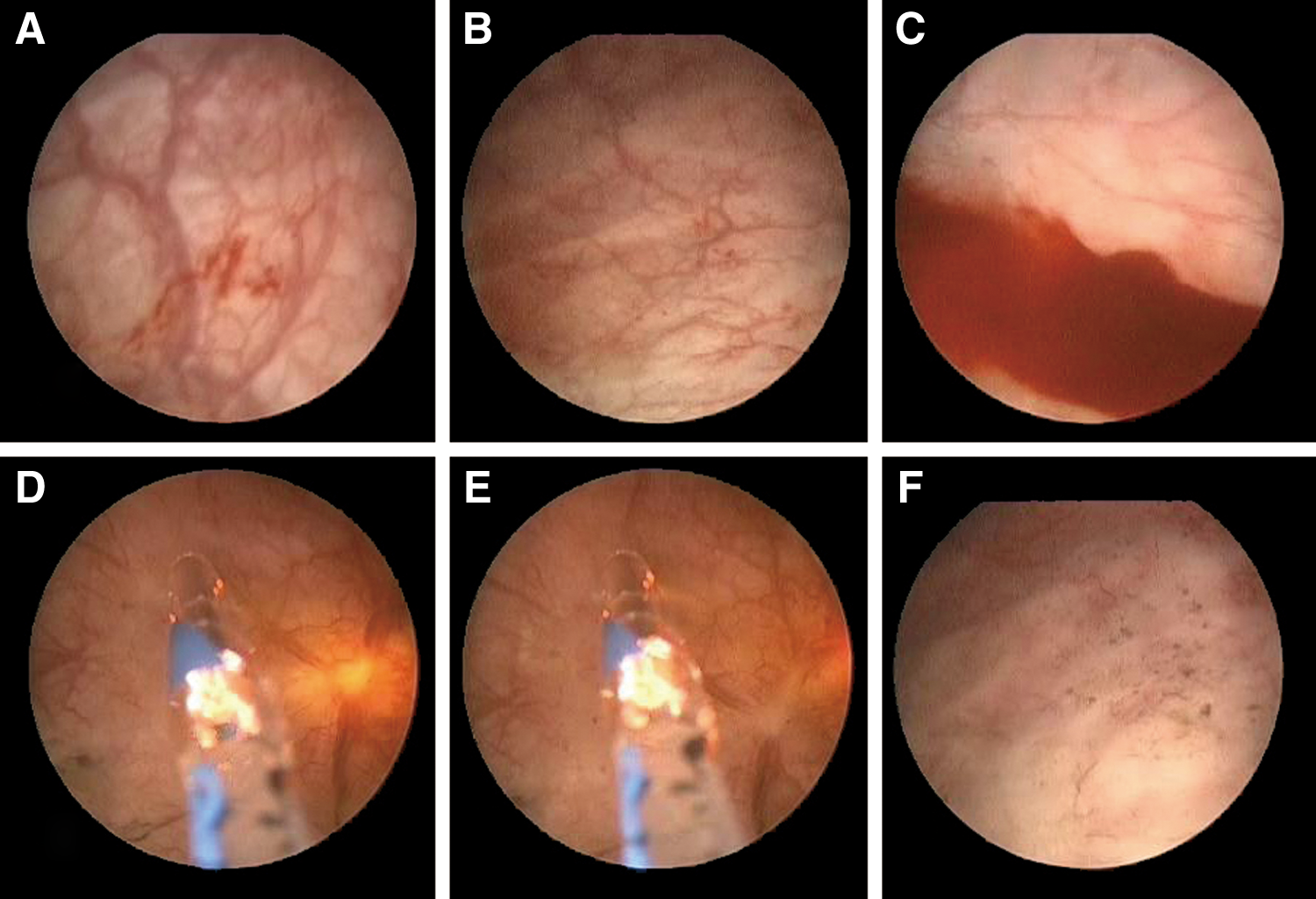
Coagulation for hemorrhagic cystitis (HC) using Greenlight KTP laser. (
All patients underwent cystoscopy 3 months postoperatively, and no bleeding or significant scarring area was found. With a mean of 17 months (6–36 months) follow-up time, recurrence of significant bleeding was seen in only one case, which recurred 7 months after operation, and was again cured by KTP laser.
Discussion
In this article, we describe a new technique using the Greenlight KTP laser for the treatment of refractory HC. It is called “Greenlight laser” because it has a wavelength of 532 nm, which is in the visible portion of the spectrum. It is also called “selective light” because the laser can be selectively absorbed by hemoglobin in tissue or blood vessels. Greenlight KTP laser has a penetration depth of only 0.8 mm and a coagulation depth of 1–2 mm, and can close blood vessels instantly.
15
The 80 W KTP laser has been widely used to treat benign prostate hyperplasia for >13 years.
16
Several randomized controlled trials have proven that it is superior to transurethral resection with regard to less blood loss and shorter catheter indwelling time and hospital stay.
17,18
As the laser
Our study does show effective control of hemorrhage where other methods have failed. No patients had hematuria immediately after operation. Cystoscopy at 3 months revealed no recurrence of bleeding. And with a mean 17 months follow-up, only one case recurred 7 months postoperatively, and it was again cured by the laser. In 2009, Tabatabaei et al. reported their experience of controlling HC using the same laser. 19 Control of bleeding was achieved in 13 patients after one session, and in 4 patients after two sessions of laser coagulation. Only one patient was refractory to all efforts, and ultimately underwent urinary diversion. No complication or recurrence was documented. Therefore, we believe that Greenlight KTP laser is a promising novel approach for the treatment of refractory HC induced by radiation.
As it is absorbed selectively by hemoglobin, produces no electric current, and has a very limited coagulation depth, Greenlight KTP laser has many advantages over electrocoagulation for the treatment of HC. These advantages include less damage to mucosa, immediate cessation of bleeding, no obturator nerve reflex, no bladder perforation, no significant scarring, and quick recovery after operation. In addition, in the present study, no bladder irritation symptoms after operation were observed.
Neodymium:YAG laser has been reported to be safe and effective for radiation-induced HC by Ravi. 8 However, he emphasized that caution must be exercised, as bleeding in radiation cystitis is purely from mucosal lesions. He proposed that use of 532 nm KTP laser that coagulates the tissues less deeply may be safer in these patients. We agree with him, because the coagulation depth of Neodymium:YAG laser is ∼4–6 mm, 20 whereas Greenlight KTP laser has the energy focused on the superficial layer of the tissues and has only a 1–2 mm coagulation depth. Large tissue necrosis is commonly seen with the Neodymium:YAG laser, which may lead to long-lasting irritative symptoms caused by sloughing off of necrotic tissue. 21
Recently, Kaushik et al. described a new technique using the 980-nm diode laser for effective management of refractory HC in four patients. 22 The outcome is promising and we are looking forward to their further research.
Safe as Greenlight KTP laser is, it is still important that coagulation be accomplished by moving the laser beam in a “painting” fashion with the fiber 3–5 mm away from the lesion.
We have to point out that although relapse may occur, bleeding can be controlled by another procedure of laser coagulation without any additional adverse reaction.
Conclusions
With its ability for instant hemostasis, a high level of safety, and quick postoperative recovery, we recommend transurethral Greenlight KTP laser coagulation as the initial treatment of choice in patients with refractory hemorrhagic radiation cystitis.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.