
Abstract
Introduction
PDT has now been used for treating cancer cells (head and neck cancers, skin cancers) and some other non-oncological diseases (age-related macular degeneration), 1,6 –9 and there are some limited applications for destroying microorganisms, such as treatment of acne vulgaris. 10 –14 However, recent in vitro studies showed the rich potential of PDT to treat wound infections caused by antibiotic resistant bacteria. 15 –17
Toluidine blue, methylene blue, chlorin e6 conjugates, and porphyrin and its derivatives are commonly used photosensitizers in antibacterial PDT. 18 –21 Those photosensitizers can be excited by light sources mostly in the range of visible spectrum, which have limited penetration capacity in biological tissue. On the other hand, wavelengths in the range of near-infrared spectrum, such as 809 nm, have more capacity to penetrate biological tissue than rest of the spectrum. Penetration depth in biological tissue for the wavelengths ∼650 nm is 3–3.5 mm, whereas for near-infrared light it reaches up to 6 mm. 22 Therefore, infections spread to deeper wounds and burns can be treated by near-infrared wavelengths of light in combination with appropriate photosensitizers. Indocyanine green (ICG) is a specific photosensitizer for wavelengths in the near-infrared spectrum with a high absorption of ∼800 nm. ICG is a water soluble, anionic tricarbocyanine dye with almost no toxicity, and it is approved by United States Food and Drug Administration for medical applications to observe liver function, cardiac output, and blood volume. 23 –26 Therefore, PDT with ICG has been investigated to treat tumors, for example, pancreatic, lung, skin, colonic and breast tumors, 27 –30 and for bactericidal purposes in the treatment of acne vulgaris. 12,31 In addition to limited clinical studies on the treatment of acne vulgaris, 12,31 the bactericidal effect of PDT with ICG has recently been investigated in a few in vitro studies. 32,33
Some of the gram-positive (e.g. Staphylococcus aureus, Streptococcus pyogenes) and gram-negative bacteria (e.g. Pseudomonas aeruginosa, Escherichia coli) are the common multidrug-resistant (MDR) pathogens and important causes of various bacterial wound infections. 33 –38 Contamination of wounds by MDR bacteria causes delayed healing and mortality in further stages. The conventional treatment of pathogenic bacteria that cause lethal wound infections are antibiotics, and the rapidly increasing resistivity to these drugs makes conventional method difficult and even impossible. 33 Other antimicrobial agents such as topical antiseptics, for example, iodine-containing solutions, silver preparations, or surgical removal can be used as alternatives to antibiotics. There is not any resistivity mechanism for these methods, but still there are some limitations or disadvantages. They are not nontoxic and/or harmless. Generally they do not target only bacteria, but also normal cells. 39 –42 Some of them (e.g., hypochlorite) cause skin irritation. They kill keratinocytes and fibroblasts as well. They influence wound healing negatively. Systemic absorption of an antiseptic such as iodine compound can cause many adverse effects, from psychological disorders to skin reactions or acidosis, and also metabolic disorders such as hyperthyroidism. Severity of iodine solution application depends upon the concentration of iodine absorbed by tissue. It is highly possible to absorb more iodine compound for wounds or burns. Therefore, using iodine as an antiseptic on infected wounds or burns is not recommended. 39,41 Some silver preparations such as silver nitrate or silver sulfadiazine are used as antimicrobial agents, also. They are not capable of penetrating deep inside the tissue. 40 Therefore, those agents are not a good choice for deeply infected wounds or burns. These problems have motivated researchers to concentrate on the development of novel, convenient, and inexpensive antimicrobial treatment strategies for fighting pathogens and wound healing. 3 –5,12 –17
PDT has numerous advantages over antibiotics, antiseptics, and surgical removal. Multidrug-resistivity can develop after repeated use of antibiotics. However, development of photoresistance after multiple treatments of antimicrobial PDT has not yet been reported. 42,43 Because of its ease of application on the affected area, having many fewer side effects, being minimally invasive, and being cheaper compared with antibiotics, it is a good alternative tool for treatment of wound infections. 36
PDT with ICG and 809 nm is not currently used on wound or burn infections as an antibacterial treatment. Therefore, there are several parameters that need to be investigated, such as power and the energy dose of the laser light, exposure duration of the laser, concentration of the photosensitizer, optical properties, and location of the diseased tissue.
The aim of this study was to investigate the effects of PDT with ICG on the viability of wild type and resistant bacterial strains (S. aureus strain ATCC 25923, S. aureus clinical isolate 1755, P. aeruginosa strain ATCC 27853, and P. aeruginosa strain ATCC 19660) in vitro.
Materials and Methods
Bacterial strains
The bacterial strains used in this study were wild type S. aureus ATCC 25923 (Refik Saydam National Public Health Agency, Ankara, Turkey), resistant clinical isolate S. aureus 1755 (Gazi University, Ankara, Turkey), wild type P. aeruginosa ATCC 27853 (Gazi University, Ankara, Turkey), and resistant type P. aeruginosa ATCC 19660 (ATCC, USA). After overnight incubation in tryptic soy broth (Merck KGaA, Darmstadt, Germany) at 37°C, bacterial cells were harvested by centrifugation (3000 rpm for 10 min at 4°C) and the pellet was resuspended in phosphate buffered saline (PBS) to ∼106–107 colony forming unit/mL (CFU/mL) for S. aureus strains and 108–109 CFU/mL for P. aeruginosa strains.
Photosensitizer
ICG (Pulsion Medical Systems AG, Munich, Germany) was used as a photosensitizer in this study. Absorption and fluorescence maximum of ICG are in the near-infrared range. Wavelength ∼800 nm is suitable for this photosensitizer (Fig. 1). Fresh stock solutions were prepared in PBS before each experiment and kept in the dark. ICG concentrations used for S. aureus strains were between 0.5 and 8 μg/mL and for P. aeruginosa strains were between 50 and 150 μg/mL.

Absorption and fluorescence spectra of indocyanine green (ICG) (Documents from Pulsion Medical System).
Laser light
A computer-controlled 809 nm diode laser system was used for PDT experiments. This laser system was developed in Bogazici University, Biomedical Engineering Institute, Biophotonics Laboratory. 44 The distance of the laser probe to the plate surface was adjusted to apply 1.4 W/cm2 in each experiment (Fig. 2). Laser power was checked with an optical powermeter (Newport 1918-C, CA). The energy doses between 80 and 420 J/cm2 were applied by increasing the exposure duration from 60 sec to 5 min.
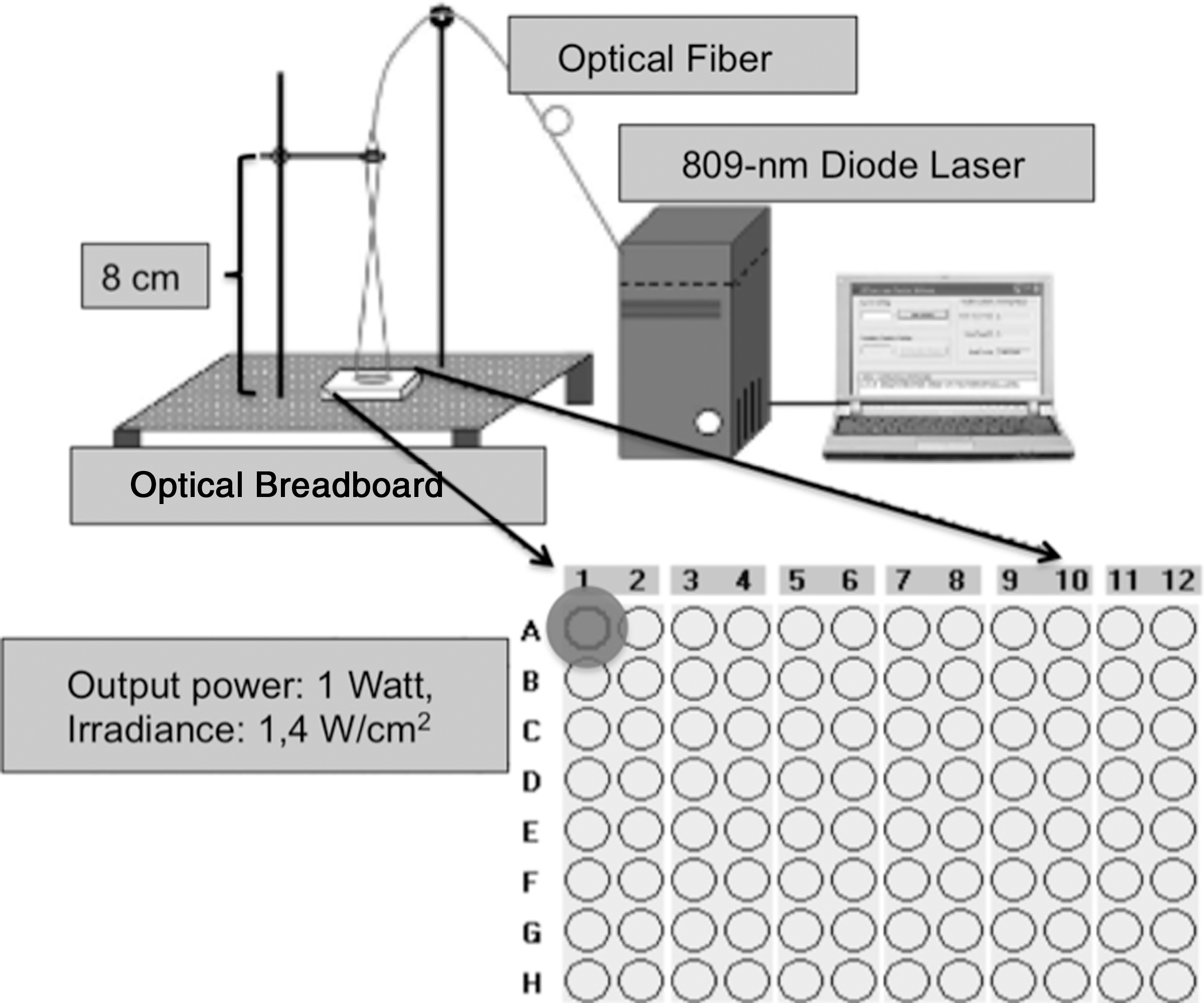
Laser setup; 809 nm diode laser is a computer-controlled system. The optical fiber of the laser system was adjusted to apply 1.4 W/cm2 on the plate surface. The distance between the laser probe and the plate surface was 8 cm.
Study design
The effects of ICG-PDT with different ICG concentrations and different energy densities were studied in vitro. The following groups were tested: 1. Control group: no ICG, no light 2. Laser-only group: irradiated without ICG 3. ICG-only group: incubation only with ICG 4. PDT (Laser+ICG) group: irradiated in the presence of ICG
Bacterial suspension (50 μL aliquots) was transferred into the wells of 96 well plate. In the ICG and PDT groups, 50 μL of ICG with a specific concentration was added to each well and mixed with bacteria. After addition of ICG, the wells were incubated in dark for 15 min. In the laser and control groups, the bacterial suspension in the wells was mixed with equal volume of PBS (50 μL). Then the bacterial suspension in the PDT and laser groups was irradiated. Following irradiation, bacterial suspension in all groups was diluted according to the serial dilution method. Then, diluted samples were plated on tryptic soy agar and incubated in dark for 24 h. The number of CFU were counted with the naked eye and multiplied by dilution factor to determine viable bacteria after each application. All experiments were repeated at least three times, and all conditions were reproduced in triplicate within each experiment.
Optimization of laser light dose
The killing effect of the laser light dose was investigated on S. aureus ATCC 25923 and P. aeruginosa ATCC 27853 wild type strains as described. Energy doses of 84, 252, and 420 J/cm2 were applied on bacterial suspension of S. aureus changing the exposure duration. Energy doses of 84, 168, and 252 J/cm2 were applied on P. aeruginosa. The temperature of the bacterial suspension in a well was measured with a noncontact infrared thermometer (ST Pro, Raytek Corporation, CA) immediately after each laser application. No temperature increase was recorded. Viable cells were counted by serial dilution method.
Effect of different ICG concentrations
The killing effect of ICG concentration was investigated on S. aureus ATCC 25923 and P. aeruginosa ATCC 27853 wild type strains without applying light. For S. aureus ATCC 25923, 0.5, 1, 2, 4, 6, and 8 μg/mL ICG were used. For P. aeruginosa ATCC 27853, 50, 100, 125, and 150 μg/mL ICG were applied. The viability was determined by serial dilution method.
Dose estimation for ICG-PDT on S. aureus wild type strain (ATCC 25923)
In the PDT groups of S. aureus ATCC 25923, bacterial suspensions were mixed with six different ICG concentrations (0.5, 1, 2, 4, 6, 8 μg/mL). After 15 min incubation with ICG, an energy dose of 84 J/cm2 was applied on the bacterial suspension. Immediately after the laser applications, bacterial suspensions were diluted to count viable bacteria.
Dose estimation for ICG-PDT on P. aeruginosa wild type strain (ATCC 27853)
In the PDT groups of P. aeruginosa ATCC 27853, bacterial suspensions were mixed with the concentrations of 50, 100, 125, and 150 μg/mL of ICG. After 15 min incubation with ICG, an energy dose of 252 J/cm2 was applied on the bacterial suspension.
ICG-PDT application on resistant strains of S. aureus 1755 and P. aeruginosa ATCC 19660
Optimum parameters of ICG-PDT were determined with wild type strains of S. aureus ATCC 25923 and P. aeruginosa ATCC 27853. An energy dose of 84 J/cm2 and 4-6 μg/mL of ICG concentrations were applied on the resistant strain of S. aureus 1755. An energy dose of 252 J/cm2 and 100–125 μg/mL of ICG concentrations were applied on resistant strain of P. aeruginosa ATCC 19660.
Data and statistical analysis
In each experiment, some of the wells were used for experimental groups and others were assigned to control samples. In order to keep the conditions constant, viable cell counts determined after serial dilution method were normalized by taking the ratio with corresponding control groups on each 96 well plate. Normalized data were analyzed for statistical significance with one way ANOVA and two tailed Student's t test. The results were considered significant when the p value was <0.05.
Results
Effect of laser light only
Three different light doses were applied both on S. aureus ATCC 25923 and P. aeruginosa ATCC 27853 to determine the effect of laser light on bacterial viability. Even the highest doses (420 J/cm2 for S. aureus and 252 J/cm2 for P. aeruginosa strains) tested did not cause significant cell death as expected. Figures 3 –6 show the results of cell viability for every bacterial strain after the application of their corresponding energy dose.
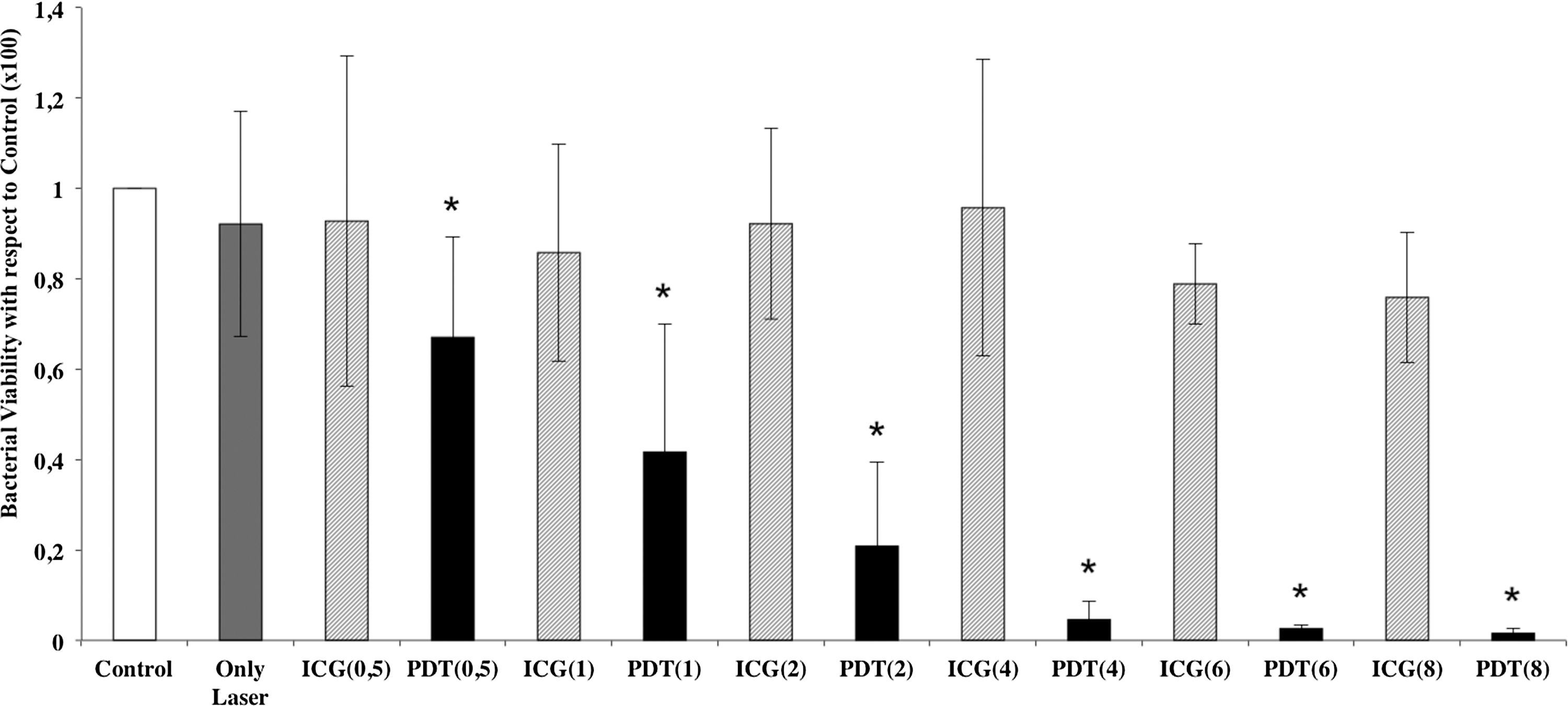
Effect of indocyanine green (ICG), laser, and photodynamic therapy (PDT) applications on wild type Staphylococcus aureus ATCC 25923. Cell viability of S. aureus ATCC 25923 after laser only, ICG only, and PDT applications was determined by viable cell count as described. Bacterial cell count in each experimental group was normalized with the untreated control group (light dose: 84 J/cm2 and ICG concentrations: 0.5, 1, 2, 4, 6, 8 μg/mL). Each column indicates normalized data±standard deviation (n>8). *Indicates the statistical significance (p<0.05) in comparison with the untreated control group.
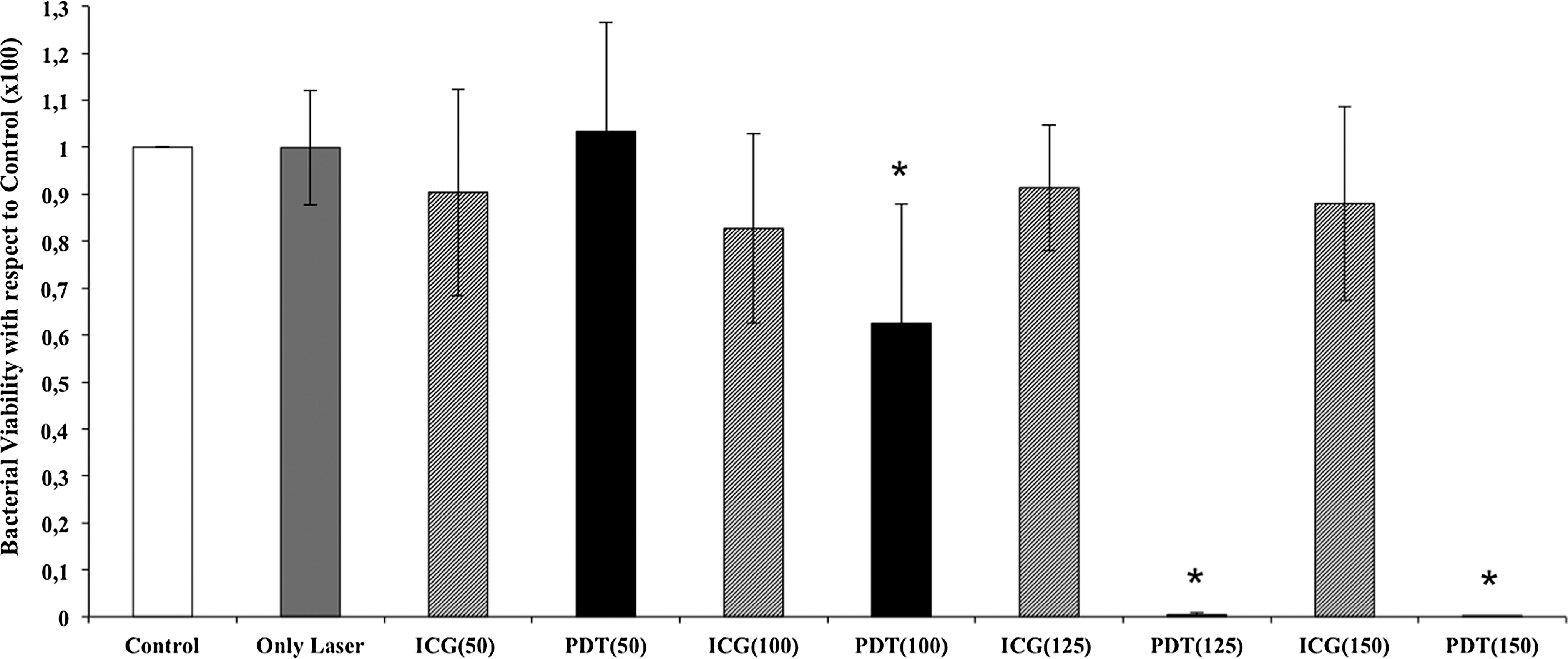
Effect of indocyanine green (ICG), laser, and photodynamic therapy (PDT) applications on wild type Pseudomonas aeruginosa ATCC 27853. Cell viability of P. aeruginosa ATCC 27853 after laser only, ICG only, and PDT applications was determined by viable cell count as described. Bacterial cell count in each experimental group was normalized with the untreated control group (light dose: 252 J/cm2 and ICG concentrations: 50, 100, 125, 150 μg/mL). Each column indicates normalized data±standard deviation (n>8). *Indicates the statistical significance (p<0.05) in comparison with the untreated control group.
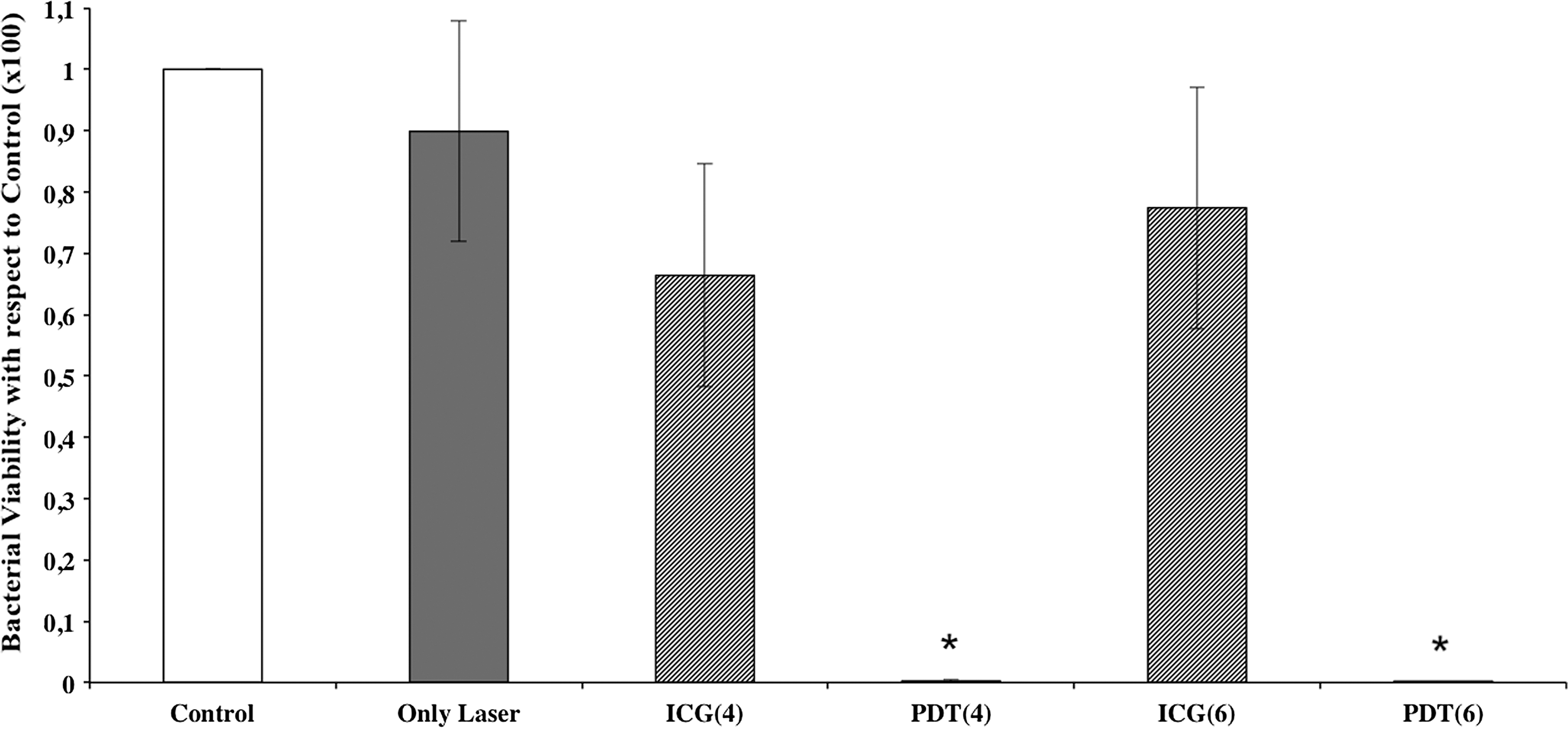
Effect of indocyanine green (ICG), laser, and photodynamic therapy (PDT) applications on resistant strain Staphylococcus aureus 1755. Cell viability of S. aureus 1755 after laser only, ICG only, and PDT applications was determined by viable cell count as described. Bacterial cell count in each experimental group was normalized with the untreated control group (light dose: 84 J/cm2 and ICG concentrations: 4 and 6 μg/mL). Each column indicates normalized data±standard deviation (n>8). *Indicates the statistical significance (p<0.05) in comparison with the untreated control group.

Effect of indocyanine green (ICG), laser, and photodynamic therapy (PDT) applications on resistant strain Pseudomonas aeruginosa ATCC 19660. Cell viability of P. aeruginosa ATCC 19660 after laser only, ICG only, and PDT applications was determined by viable cell count as described. Bacterial cell count in each experimental group was normalized with the untreated control group (light dose: 252 J/cm2 and ICG concentrations: 100 and 125 μg/mL). Each column indicates normalized data±standard deviation (n>8). *Indicates the statistical significance (p<0.05) in comparison with the untreated control group.
Effect of ICG concentrations on bacterial viability
In order to find the safe working range for ICG, six different ICG concentrations (0.5, 1, 2, 4, 6, 8 μg/mL) were tested on S. aureus ATCC 25923 and four different ICG concentrations (50, 100, 125, 150 μg/mL) were tested on P. aeruginosa ATCC 27853. Among the concentrations used in this study, ICG induced- cytotoxicity was not observed.
Dose estimation for ICG-PDT on S. aureus wild type strain (ATCC 25923)
The lowest light dose (84 J/cm2) was used with previously tested ICG concentrations (0.5, 1, 2, 4, 6, 8 μg/mL) on S. aureus ATCC 25923. In the PDT groups, all of the applications caused significant decrease of cell viability. A more than 90% decrease with the application of 84 J/cm2 of light dose and 4 μg/mL of ICG concentration was observed. When the concentration of ICG was increased (6 and 8 μg/mL) in the PDT group almost 100% cell death was achieved (Fig. 3).
According to these results, 4 μg/mL of ICG concentration is the critical threshold with 84 J/cm2 of light dose. Both of the laser and ICG were nontoxic when they were applied alone.
Dose estimation for ICG-PDT on P. aeruginosa wild type strain (ATCC 27853)
Light dose (252 J/cm2) was used with four different ICG concentrations (50, 100, 125, 150 μg/mL) on P. aeruginosa ATCC 27853. This energy dose was not phototoxic when applied alone. Only a 1% decrease in the bacterial load was observed. Similarly, none of these ICG concentrations was cytotoxic on this strain when applied alone. ICG (150 μg/mL) caused the highest cytotoxicity, and it was only a 12% decrease in the bacterial load and not statistically significant. All the PDT applications caused significant decrease, except the PDT application with 50 μg/mL of ICG. Among them, the combination of 252 J/cm2 light and 125 μg/mL ICG concentration achieved>99% killing effect on these gram-negative bacteria (Fig. 4).
ICG-PDT application on resistant strains of S. aureus and P. aeruginosa
After dose estimation of ICG-PDT on wild type strain S. aureus ATCC 25923, the combination of light dose (84 J/cm2) and ICG concentrations (4 and 6 μg/mL, which were effective on wild type strain) were applied on resistant strain S. aureus 1755. It was observed that the applied doses were effective in the photoinactivation of the resistant strain. Nearly 100% bacteria were killed after PDT application with these combinations (Fig. 5).
Similarly, optimum doses (252 J/cm2 of light dose and 100–125 μg/mL of ICG concentrations) determined for the photoinactivation of wild type P. aeruginosa ATCC 27853 were applied on resistant strain P. aeruginosa ATCC 19660. These PDT combinations were effective for the photoinactivation of this resistant strain, also. Almost 100% of bacteria had died after the PDT application with 100 μg/mL of ICG, whereas for the wild type, 60% of the bacteria were alive after the same dose of PDT. PDT with 125 μg/mL of ICG and 252 J/cm2 of light killed all the bacteria. There were no viable bacteria counted after this application (Fig. 6).
Discussion
Although the near infrared spectrum is highly advantageous because of its deeper ability to penetrate biological tissues, almost all antibacterial PDT studies were performed with visible light. So far, the only antibacterial PDT study that reported the lethal photosensitization of ICG on S. aureus, S. pyogenes and P. aeruginosa was by Omar et al. 33
In our study, PDT with the combination of ICG and 809 nm light was investigated on wild type and resistant strains of S. aureus and P. aeruginosa. In the first part, dosimetry study was performed on wild type strains. For gram-positive S. aureus, the same bactericidal effect was achieved with almost fivefold lower dose of laser (84 J/cm2) and approximately six times less ICG concentration (4 μg/mL) compared with the study by Omar et al. 33 Similarly, for the gram-negative P. Aeruginosa, both the laser dose (252 J/cm2) and ICG concentration (125 μg/mL) was found to be twofold lower. The output power and the bacterial strains are different between our study and the report of Omar et al. These could be the reasons to achieve the same bactericidal effect with lower ICG concentrations. First, Omar et al. applied 470 mW as output power to reach 411 J/cm2 of energy dose, 33 whereas 1 W of output power was used in this study. This output power could be strong enough to kill a higher amount of bacteria with lower energy doses. Second, bacterial strains of S. aureus and P. aeruginosa were different between these two studies. The efficiency of PDT seems to be unpredictable, and may or may not differ among the different strains of the same species. 19,21,45 For example, Grinholc et al. 45 investigated the effect of protoporphyrin diarginate (PPArg2) on eighty clinical S. aureus strains (40 resistant strains and 40 susceptible strains) to reveal the efficiency of photodynamic therapy on different strains. It was concluded that bactericidal effect of PPArg2-PDT was strain dependent, with no obvious correlation between photoinactivation and drug resistance. For the gram-negative Pseudomonas species, higher doses of laser energy and ICG compared with S. aureus was required for 99% killing efficiency. The difference in ICG concentrations for two different types of bacteria could be explained by the structural differences, such as the structure and arrangement of peptidoglycan layers and the presence of outer membrane that is anionic in structure in gram-negative bacteria. The highly anionic nature of the outer membrane of gram-negative bacteria will most likely to have a negative impact on the amount of ICG that can either attach or penetrate into the bacterial cell. The preference for wavelengths in the visible spectrum that have suitable cationic photosensitizers seems to be the explanation of limited data on near-infrared light and ICG in antibacterial applications. However, our findings on P. aeruginosa were still lower than those of the earlier report, and were within the safe working concentrations and fourfold less than clinical acne studies. 31 George et al. 32 investigated the bactericidal activity of anionic and cationic photosensitizers on gram-positive Enterococcus faecalis and gram-negative Actinobacillus actinomycetemcomitans. Cationic methylene blue and rose bengal and anionic ICG were used as photosensitizers with appropriate wavelengths. It was observed that methylene blue was the most effective photosensitizer among the others. The relatively low efficiency of ICG in this report 32 could easily be explained by insufficient analysis of parameters, such as the too-low energy dose of 3.6 J/cm2. Among the cationic photosensitizers, the efficiency of photoinactivation also differs depending upon the structure, amount, and distribution of the positive charge. For example, Banfi et al. 18 investigated the effect of seven different porphrin derivatives in combination with halogen-tungsten lamp with 266 J/cm2 on E. coli, S. aureus, and P. aeruginosa strains in vitro. It was reported that cationic derivatives of porphyrin were more effective than the non-ionic derivative of porphyrin, and that gram-positive S. aureus was more sensitive to these compounds than were the gram-negative E. coli and P. aeruginosa. 18
For the first time, the antibacterial effect of ICG-PDT on wild type and drug- resistant strains of two different bacterial species were examined comparatively in this study. Keeping the applied energy dose constant for both wild type and resistant strains, it was found that even much lower ICG concentrations had equally effective bactericidal activity on both resistant strains of S. aureus and P. aeruginosa. Therefore, it might be speculated that resistant strains of S. aureus and P. aeruginosa were even more susceptible to ICG-PDT than wild type strains. Although the mechanism is not still understood clearly, even the different strains of the same species of bacteria could respond differently in PDT applications. It was hypothesized that this difference might be the result of variation in structures on the outer layers of bacteria, which might possibly effect the binding or uptake of the photosensitizer.
21,45
In parallel with our study, the work by Tseng et al.
19
that investigated 60 different clinical isolates and wild type P. aeruginosa had shown that a multidrug-resistant P. aeruginosa strain was more susceptible to toluidine blue O (TBO)-PDT than were non-resistant forms. Similarly, Tang et al.
21
investigated the effect of two cationic photosensitizers, TBO and poly-
Conclusions
In conclusion, this study shows that PDT with nontoxic ICG and low energy doses of 809 nm laser light is an alternative powerful tool to destroy wound-infecting antibiotic-resistant microorganisms. As future work, it would be important to investigate reasons for strain-dependent photoinactivation and the effect of the output power of the light source. It would be valuable to investigate the thermal effect and to detect the safe thermal area of this wavelength on an animal model during antibacterial PDT. It could lead to a wide range of clinical applications. Wound infections could be life threatening for patients with deep burns or diabetic ulcers. Infections easily proceed deep inside these tissue types. PDT with ICG and 809 nm laser is a powerful alternative to treat these infections, because of the penetration capability of this specific wavelength. This method would be also useful for surgical site infections, soft-tissue infections, gastric infections, and oral and dental infections. 5
Footnotes
Acknowledgments
This work was supported by the Bogazici University Scientific Research Projects (BAP 5892 to M.G. and BAP 6380 to S.Y.) and the Scientific and Technological Research Council of Turkey (TUBITAK 111E255 to M.G.). We thank Nedim Sultan from the Department of Microbiology, Gazi University (Ankara, Turkey), for providing some of the strains used in this study. We also thank Ozgur Tabakoglu, Temel Bilici, Ayse Sena Sarp, and Ozguncem Bozkulak for their help and valuable opinions.
Author Disclosure Statement
No competing financial interests exist.