
Abstract

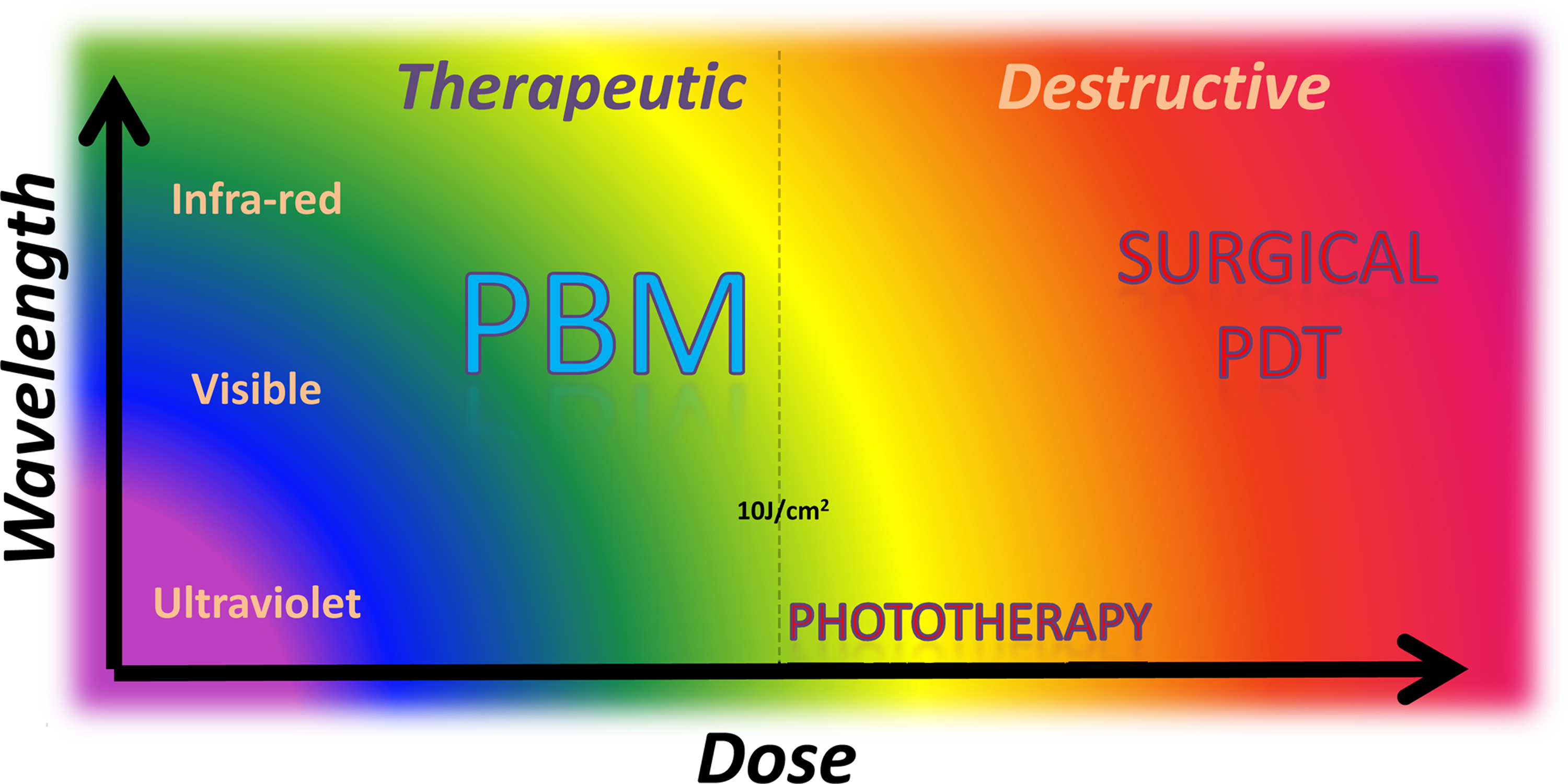
Spectrum of biological responses in photomedicine. PBM, photobiomodulation; PDT, photodynamic therapy.
The Path Ahead …
There appear to be two concrete and interconnected directions the field needs to take currently to move forward to mainstream acceptance. First, the major bottleneck is our lack of understanding of the triad representing precise molecular mechanisms, biological contexts, and related dose for each application (Fig. 2). It is well established that no single drug or surgical procedure can address all medical ailments. Hence, it would be unreasonable to expect a single light dose or mechanism to be a universal panacea. 4,5 There appear to be two schools of thought on the predominance of energy (fluence, J/cm2) versus power (irradiance, W/cm2) for the efficacious dose, the right dose must also include two other inherent, critical variables, namely, time and biological context. 6 There are also a plethora of instrument choices available with each light device such as wavelengths, pulsing, distance, coherence, beam profile, spectral width, among others that need to be carefully vetted for specific clinical use with respect to the appropriate biological molecular interactions. 7 For example; the rationale for 670 nm use has been clearly validated by the identification of its biological photoacceptor, the mitochondrial enzyme cytochrome c oxidase. 8 –11 The primary photoacceptors for other wavelengths currently, despite demonstration of their clinical efficacy, remain to be elucidated.

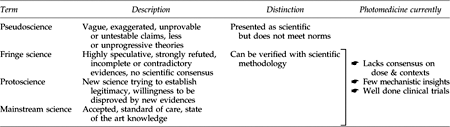
Progression of fields of science and current limitations in the field of photomedicine.
This leads us to the second potential direction forward: lack of consistency or consensus on terminology or guidelines. The often cited MeSH term “low level laser therapy” (LLLT) itself is vague as to what connotes “low” and “level” (dose?). Moreover, the limitation of “laser” is no longer accurate, as other light devices, such as LEDs, are fast becoming equally popular. Further, despite the lack of precise mechanisms and, therefore, inability to define ideal dose–disease guidelines, there is already a plethora of clinical literature available. The PBM literature is replete with reports on numerous successful treatments as well as many instances of inefficacious or negligible potency. Whereas negative studies are excellent harbingers of exploring true efficacy, studies that are poorly done because of technical inadequacies make for significant barriers to progress of the field. This is where photomedicine journals – a cornerstone of scientific methodology via peer review – play key roles for quality assurance and must facilitate rigorous and unbiased evaluation of the scientific evidences presented. In evaluating these evidences, and inherent to its progression from a fringe science to a protoscience, PBM must be open to new evidences and evolve with them to newer predictions and theories. The cornerstone of scientific methodology is the ability to reproducibly and reliably demonstrate efficacy, without bias, and with statistical rigor. Given the sophistication and resources available for elucidating these scientific evidences, exploration at the whole organismal level and dissecting the tissue, cellular, molecular, and even atomic scale is now feasible and must be encouraged and pursued. Another avenue to develop consensus is collaborations between the major stakeholders: the photomedicine societies. Organizations such as World Association for Laser Therapy, North American Association for Light Therapy, American Society of Laser Medicine and Surgery, American Society of Photobiology, and International Society for Optics and Photonics, among others, must step up and take a lead in outlining guidelines by discussion and debate, giving all evidences their logical and fair inputs, which is sorely lacking in the field.
Let Us Not Miss the Forest for the Trees. …
Concurrent to the exploration of molecular mechanisms, providing the best clinical care as judged by each of our patients' subjective satisfaction and comfort is the foundation and practical reality of modern medicine. Although this is still the basic yardstick we must aspire to in PBM, “the patient getting better” must be more objectively assessed with the use of standardized assessment tools and, whenever feasible, the use of relevant and sensitive biomarkers. This can add immeasurably to the progression of the field by establishing a reliable and robust clinical evidences database. How these uniform evaluation criteria can be established and the database developed, evaluated, and organized remain practical challenges for the field. Although the gold standard for clinical research remains a multicenter, placebo-controlled, double-blind, randomized clinical trial, the funding priority for photomedicine applications and costs are massive prohibitive barriers. Alternatively, innovative approaches such as the recently launched practice-based research networks (PBRNs) aim to tap into the vast, conventional clinical care networks to actively involve and promote clinical research. 12
Other Future Avenues …
In addition to the two major avenues to forge PBM into mainstream medicine via basic mechanistic research and well-designed clinical studies, there are exciting parallel avenues that currently utilize low-energy light-based devices such as common laboratory tools (spectroscopy, microscopy, and optical traps) and clinical modalities (skin resurfacing technology and in vivo imaging). These modalities could be exciting new avenues to further explore the biological basis of light-biological interactions that could complement the progress in the field of PBM.