
Abstract

First reports on LLLT on OM originated from Nice, France in 1992, and since then there have been reports of several randomized control studies with promising outcome. 4 –8 In 2007, Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC-ISOO) Mucositis Guidelines have upgraded LLLT as a “recommended” method for the prevention of OM during HSCT. 9
LLLT of an output power range from 5 to 200 mW with helium/neon (He/Ne) laser of wavelength 632.8 nm or diode lasers of various wavelengths ranging from 630 to 680 nm, 700 to 830 nm, and 900nm is an efficacious, simple, and atraumatic technique in the treatment of OM, with no known toxicity in clinical setting. 8,10,11 In addition, LLLT has been found to reduce the total duration and severity of OM in all the studies, with a few exceptions in which the laser parameters were, perhaps, inadequate. Another debilitating effect of OM is orofacial pain, which often depends upon existing oral health; underlying disease, type of treatment, severity of OM, and pain threshold. It has been shown that there is considerable reduction in orofacial pain in those patients who underwent LLLT. Although side effects were reported, none of them was different from those experienced by the control group, which is a clear indication of how well LLLT was tolerated by cancer patients, irrespective of their mode of cancer treatment. 5 –7,10
Perhaps one of the main pitfalls in past reports of studies with LLLT is the inconsistency in the parameters used, the calibration of the laser device, and the manner in which LLLT was delivered to the site. It is vital to formulate a protocol on parameters from the existing data on what is best for both a prophylactic dose and therapeutic effect. Briefly, we recommend a fairly simple regimen as follows, when considering a commercially available device: wavelength for a red light source at 633–685 nm, infrared 780–830 nm; output of diode between 10 and 150 mW; dose in the range of 2–3 J/cm2 for prophylaxis, and not less than 4 J/cm2 for therapeutic effect; application on single spot on a lesion rather than a scanning motion over the entire lesion. Also one should follow a simple formula such as
Lesions must be evaluated and therapy should be provided by a trained clinician and should be repeated daily or every other day during RT or other chemotherapy regimens and HSCT, or a minimum of three times per week until resolution.
Options on commercially available devices are of extra-oral devices and intra-oral devices (Fig. 1) targeting structures such as cutaneous and oral mucosal surfaces, respectively. Effects of an extra-oral device (Fig. 2) for LLLT over the cutaneous surface of the affected face may well reach the intra-oral structures such as the buccal mucosae, vestibule, and inner epithelial surfaces of the lips, with wavelengths ∼830 nm, but not with 630–660 nm. A combination of the above two devices must be considered while managing the head and neck RT-induced effects, but not necessarily for chemotherapy induced intra-oral effects, for which an intra-oral device would suffice.
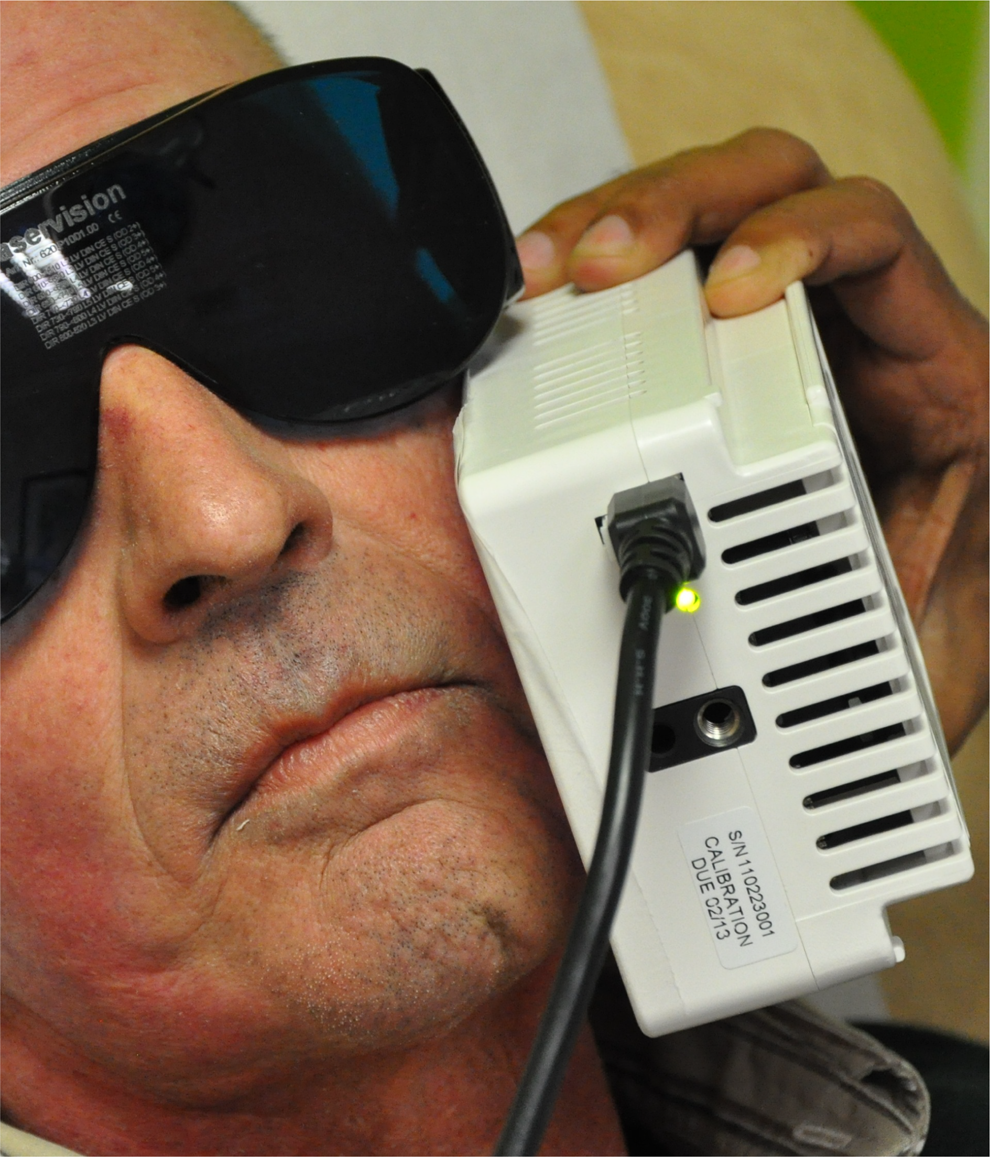
Transcutaneous laser application.

Intra-oral laser application.
Finally, following good practice guidelines, such as therapeutic optimization of a commercially available device by calibrating according to the need, such as RT of the head and neck, chemotherapy, or a combination of the foregoing by following the previously mentioned recommendations is critical. We acknowledge the clinical trials, recent reviews, and guidelines on LLLT and the solid research data generated, which has tremendously helped us, but it is beyond the scope of this Editorial to list them all.
The emerging role of phototherapy in OM is clear, and it is pragmatic to envisage LLLT in prophylactic and therapeutic intervention protocols of OM in cancer patients. A joint consensus on this is perhaps the next step, from the wider community of clinicians such as radiation oncologists, medical oncologists, hematologists, oral medicine specialists, nurses, and other professionals involved in supportive care in cancer.