
Abstract
Introduction
T
Thyroid hormones regulate the body's metabolism and, among other actions, stimulate cellular differentiation and proliferation. 10,11 When these hormones are below normal serum levels, they cause disturbances in the metabolic activation of the tissues, on the secretion of fibroblasts, and synthesis and deposition of collagen fibers, 5,12 extending from the inflammatory phase to the proliferative phase, as these are associated with the proliferative process in wound healing. 13
The literature has demonstrated that low level-laser therapy (LLLT) is able to induce several modifications during the cutaneous healing process, especially in favoring newly formed collagen fibers to be better organized and compactedly disposed. 14 Phototherapies have been extensively studied using several models of wound healing, and most previous reports have evidenced beneficial effects for this modality of treatment. 14,15 LLLT has the ability to incite some biological phenomena capable of modulating the morphological pattern of the connective tissue during repair and healing. 14 However, little is known about the tissue changes that may occur as a result of its use, particularly regarding the modulation of the extracellular matrix associated with hypothyroidism.
The mechanism of wound healing, as aforementioned, includes fibroblast proliferation, the production of type I and type III collagen, and dermal matrix remodeling. 16 The benefits produced by the interaction of laser light with biologic tissues determine its use as an adjuvant in the treatment of several complications, such as those associated with hypothyroidism. 17 Moreover, in view of the shortage of scientific studies aiming to characterize possible interferences of low-power laser regarding the synthesis and maturation of the fiber components of the connective matrix, such as type I and III collagen, the present study aimed to assess, immunohistochemically, the impact of hypothyroidism and the effect of laser phototherapy on the expression of type I and III collagen during wound healing.
Materials and Methods
Following the approval of the Animal Experimentation Ethics Committee of the School of Dentistry of the Federal University of Bahia, 48 young adult male Wistar albino rats with an average age of 2 months, and weighing between 200 and 230 g, were obtained from the vivarium of the Federal University of Bahia, and were kept at the Animal Experimentation Laboratory of this school. The animals were kept in individual plastic cages lined with wood chips and maintained at 25°C in a 12h/12h day/night light cycle.
The animals were fed a standard laboratory diet and had water ad libitum. After a regular quarantine period, the animals were randomly distributed into euthyroid and hypothyroid groups with 24 animals each, and these were divided into two subgroups of 12 animals each, according to the type of phototherapy to be received: unirradiated euthyroid (EC), euthyroid irradiated with laser light (EL), unirradiated hypothyroid (HC), and hypothyroid irradiated with laser light (HL) (Table 1).
CW, continuous wave.
Hypothyroidism was induced in rats by oral administration of propylthiouracil 100 mg (Biolab, Taboão da Serra, SP, Brazil) diluted in drinking water (0.05 g/100 mL) for 4 weeks and maintained until the end of the experiment. This model of induction to hypothyroidism has been described in the literature as a simple and effective method in the induction of this endocrine dysfunction. 18
Using intraperitoneal general anesthesia (ketamine hydrochloride 10%, 80 mg/kg and xylazine hydrochloride 2%,14 mg/kg, Syntec of Brazil, Cotia, SP, Brazil), blood samples were collected through the animals' jugular veins for plasmatic dosage of thyroid hormone. The plasmatic dosage of thyroid hormones was performed by chemiluminescence immunoassays, using commercial kits (Johnson & Johnson® Produtos Profissionais Ltda, São Paulo, SP, Brazil). 18 This chemical test is used to quantify a specific substance in a blood sample using an immunological reaction. It measures the formation of antibody-antigen complexes and detect then via an indicator reaction with a chemiluminescent molecule.
Next, the animals had their dorsa shaved and cleaned with 2% chlorohexidine solution (Merthiolate®, Hypermarcas S.A., Barueri, São Paulo, Brazil). A standardized excisional wound (1 cm×1 cm) was created with a scalpel in the mid-dorsal region of each rat and was left without suturing or dressing (Fig. 1).

Laser irradiation was started immediately after surgery and was repeated at every other day for 7 or 14 days (Fig. 1). The wounds were irradiated with laser light applied and fractioned on four different points corresponding to the angles of the wound [λ660 nm, 40 mW, continuous wave (CW), ø=0.04 cm2, irradiance 1 W/cm2, energy of 6 J per point, irradiation time 150 sec per point, and fluence 150 J/cm2 per point, Twin Flex Evolution®, MMoptics, São Carlos/SP, Brazil]. The irradiation was performed by contact with a probe positioned perpendicularly to the irradiated tissue (Table 1).
The systemic status influences the healing process and photobiomodulatory effects are more evident with the use of red light with spatial average energy fluency (SAEF) near 20 J/cm2. 17 As there is no ultimate irradiation protocol for experimental models associated with hypothyroidism, we performed a pilot study to determine the most suitable amount of energy to use, and found a value of 6 J/cm2 per point. Moreover, the dose also was selected on the basis of previous studies by Pinheiro et al., 17 Ramalho et al., 18 and Meireles et al. 19 Each animal was euthanized with an overdose of general anesthetic at day 8 or 15 after surgery. Specimens were removed and fixed in 10% formalin for 24 h, after which they were routinely cut and embedded in wax and processed for immunohistochemistry.
The immunohistochemistry study was performed for all cases to evaluate the presence of anticollagen type I and anticollagen type III. Paraffin-embedded 3 mm thick sections were obtained and assembled on slides previously treated with aminopropyltriethoxysilane. After deparaffinization and pretreatment for antigen retrieval, the blocking of endogenous peroxidase activity was performed by incubation with 3% hydrogen peroxide solution for 45 min. Specimens were incubated overnight with the primary antibody anticollagen type I (clone COL-1, Abcam, Cambridge, MA) and anticollagen type III (clone FH-7A, Abcam, Cambridge, MA) diluted in phosphate-buffered saline (PBS)-0.1% bovine serum albumin (BSA) at dilutions 1:300 and 1:700, respectively, at 4°C for 18 h in a humidity-controlled chamber, according to the manufacturer's instructions. The sections were then washed twice with PBS and Tween 0.25% at room temperature. Immune complexes were subsequently treated with the EnVision Polymer (EnVision™ System, K406189-2 DAKO Corporation, Carpinteria, CA). Immunoreactivity was visualized with 3,3′-diaminobenzidine tetrahydrochloride (Liquid DAB+, K3468-1, DAKO), prepared according to the manufacturer's instructions. The slides were counterstained with Mayer's hematoxylin. Corresponding positive external controls were used for each antibody. Negative controls included replacement of the primary antibody with non-immune bovine serum.
The criteria used for the interpretation of immunohistochemistry staining for anticollagen type I and anticollagen type III antibodies consisted of the intensity of the immunoexpression presented by the type of collagen fiber in the wound area. The immunohistochemical analysis was performed by an experienced pathologist in a double-blind manner by light microscopy (AxioStar®, Zeiss, Germany) with high magnification (40×) and scored into the following four groups: absent (−), discrete (+), moderate (++), and intense (+++), when the wound area was compared with healthy subjacent tissue. The data were analyzed by nonparametric Fisher's exact test. The statistical significance level was set at 5%.
Results
During the postsurgery period, the animals remained healthy, with normal healing on the operated site, without clinical evidence of infection. The hypothyroid group had values for T4 significantly lower than those of the euthyroid animals (ANOVA, p=0.000). The values for euthyroid animals were 2.92±0.40 μg/dL, whereas those for hypothyroid animals were 0.66±0.06 μg/dL.
Seven days after the surgery, the euthyroid and hypothyroid groups irradiated with laser showed greater immunoexpression of type I collagen than unirradiated groups, but there were no significant differences among the groups (Fig. 2). When the EC and EL groups were compared with the HC and HL groups, respectively, the immunoexpression of type I collagen was significantly higher in the EC than in the HC group (Fisher's exact, p=0.019); however, there was no statistically significant difference when the irradiated groups were compared with each other (Table 2).
Immunoexpression of type I collagen in the groups evaluated at 7 days:
p<0.05. Group with significant intra- and intergroup differences (* ax,cx p=0.019; * ax,ay p=0.047; * bx,by p=0.023; * dx,cy p=0.019).
The immunoexpression of type I collagen was significantly higher in the EC and EL groups evaluated at 14 days than in EC group evaluated at 7 days (Fisher's exact, p=0.047 and p=0.023, respectively), and in the HC group evaluated at 14 days when compared with HL group evaluated at 7 days (Fisher's exact, p=0.019). No significant difference was found in the experimental period of 14 days among the groups (Table 2).
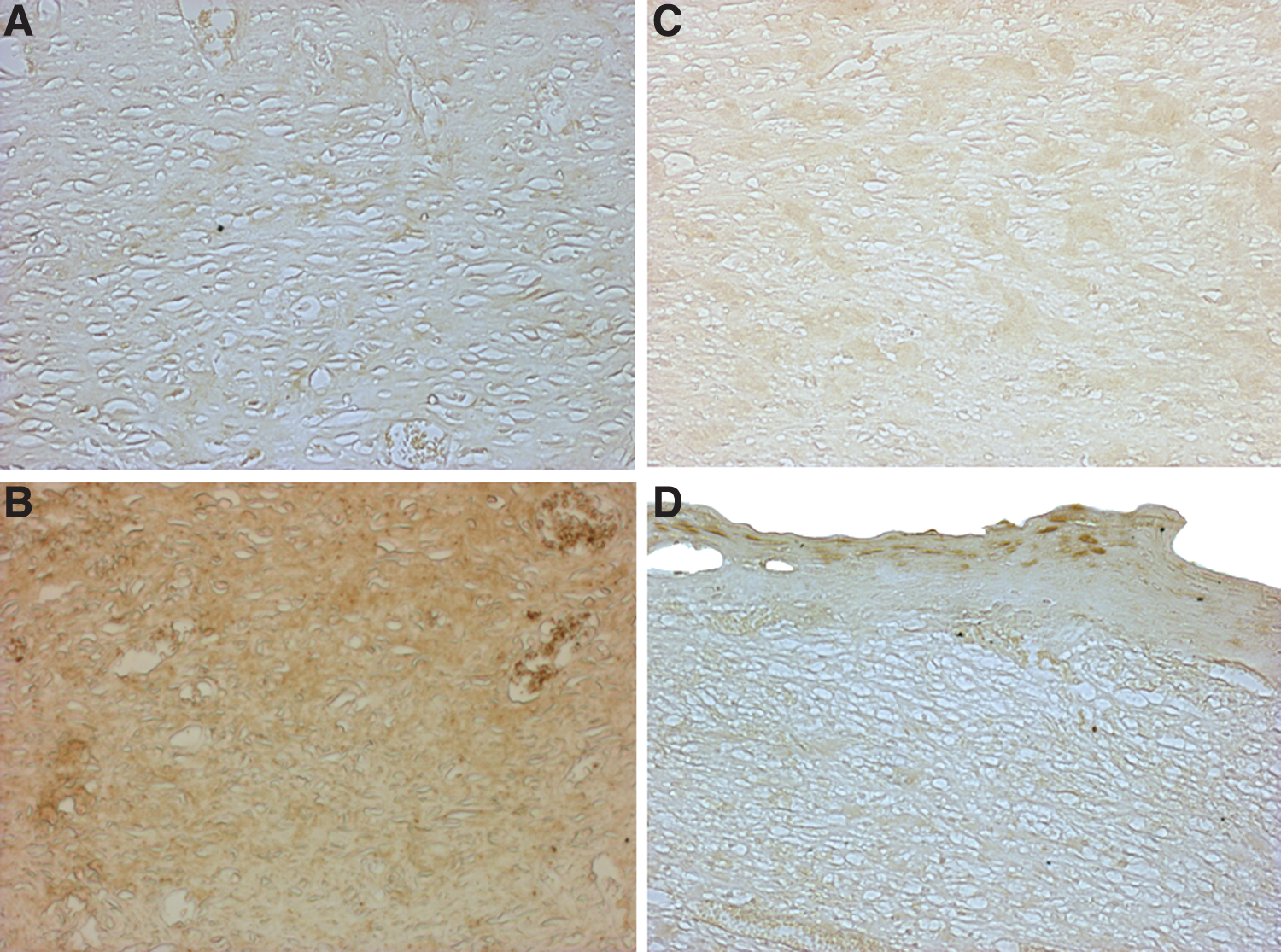
In the euthyroid group, the immunoexpression of type III collagen 7 days after the surgery was predominantly moderate in the EC group (66.7%) and discrete in the EL group (100%). In the hypothyroid groups it ranged from discrete (50%) to moderate (33.3%) and intense (16.7%) in the HC group, and ranged from discrete (16.7%) to moderate (83.3%) in the HL group (Fig. 3). Statistical analysis revealed that the EC group presented immunoexpression of type III collagen significantly higher than did the EL group (Fisher's exact, p=0.047). The EC and HL groups also showed immunoexpression of collagen III higher than did the HC group, but this was not statistically significant. The immunostaining was significantly higher in the HL group than in the EL group (Fisher's exact, p=0.019) (Table 3).

Immunoexpression of type III collagen in the groups evaluated at 7 days:
p<0.05. Group with significant intra and intergroup differences (* ax,bx p=0.047; *dx,bx p=0.019; * by,bx p=0.019).
When both groups evaluated at 7 and 14 days after surgery were compared, the immunoexpression of type III collagen was significantly higher in the EL group assessed at 14 days than in the same group evaluated at 7 days (Fisher's exact, p=0.019). The EC group also showed greater immunoexpression of type III collagen at 14 days than the same group evaluated within 7 days, but there was no statistically significant difference. There were no statistically significant differences among the groups studied in the experimental group at 14 days (Table 3).
Discussion
The values for T4 levels found in this study allowed us to observe the success of the method used to induce hypothyroidism, because the hypothyroid rats had values for T4 lower than those of the euthyroid animals. When thyroid hormones are below normal serum levels, they cause disturbances in the metabolic activation of the tissues, delaying the wound healing process 5,12,18,20 by prolonging the inflammatory phase, decreasing the amount of collagen fibers, and delaying their maturation and organization. 5 However, the influence of thyroid hormone on wound healing is not fully understood, 20 and the small number of studies limits our discussion about the relationship between thyroid hormones and skin wound healing.
Several factors may interfere with the structural pattern and the amount of collagen fibers deposited during the healing process. We had previously demonstrated that hypothyroidism delays wound healing, as the wounded area of euthyroid rats was significantly smaller than that of hypothyroid ones in the experimental period of 7 days. 21 In the present study, the distribution pattern of collagen I and III between euthyroid and hypothyroid rats mostly at day 7 of the experiment reinforced the interference of this systemic condition in tissue repair, as also observed by Biondo Simões et al. 12 and Zimmerman et al. 5 However, the literature has few experimental models that assess the process of cutaneous wound healing associated with deficiency of thyroid hormones. The difficulty of spontaneous healing, especially in cases of chronic skin lesions associated with factors that interfere with the repair process, such as systemic dysfunctions, justifies the use of therapeutic resources, such as laser phototherapy, which can accelerate it.
The literature has demonstrated the effectiveness of laser phototherapy in the acceleration of tissue repair, 22 –27 particularly regarding its influence on the modulation of the wound healing process, 8,15 accentuating the cellular biochemical reactions and thereby contributing to a significantly more efficient resolution of the wound. 15 However, there are limited studies that assess the association of laser light with systemic involvement, such as diabetes, malnutrition, and anemia. 17 –19,28,29
A variety of studies in the literature have shown the effect of light on fibroblastic proliferation 30 –32 and the deposition and organization of collagen fibers during the repair process, accelerating wound healing. Medrado et al. 14 and Pugliese et al. 15 evaluated the effect of laser phototherapy (λ670 nm) in the production of collagen fibers during the process of wound healing, and observed higher expression of the collagen fibers in the groups irradiated with lasers, when compared with unirradiated tissues. Garavello-Freitas et al. 33 and Fung et al. 34 also observed that LLLT induced the formation of more compact, thicker, and parallel-disposed collagen fibers.
Collagen is the main component of the extracellular matrix of tissues, and is important in the remodeling process of the wound. A healthy dermis contains ∼80% type I collagen and 20% type III collagen. Granulation tissue expressed 30–40% of type III collagen, considered an immature collagen. 35 However, the literature has not demonstrated specifically which type of collagen fiber is interfered with by thyroid hormone deficiency. Therefore, this study chose to evaluate the immunoexpression of type I and III collagen during the repair process, as these are main components of the extracellular matrix, responsible for the remodeling phase and essential to ensuring the tissue's resistance.
The quality and the amount of collagen fibers in the extracellular matrix, as well as their thickness and distribution in the remodeling and maturation of tissue, are responsible for providing greater resistance to wound healing tension. 5,13 In the early stages of tissue healing, collagen fibers are delicate and are loosely arranged, being represented predominantly by type III collagen. On the other hand, in the later stages of the repair process, type III collagen is resorbed and a thicker collagen is produced and organized along the lines of tension, which increases the tensile strength of the wound, 36 exhibiting a more compact organizational pattern; these denser beams are mainly represented by type I collagen. 14 The highest percentage of type I collagen compared with type III collagen indicates the state of collagen maturation. 37
Regarding the characterization of the collagen presented by newly formed tissue, Melo et al. 38 observed that in the groups irradiated with laser and evaluated at 7 and 14 days, there were, respectively, a tendency to the predominance of type III collagen, or mixture of type I and III collagen, in equal proportions, whereas in the control group, type I collagen predominated. In our study, when the irradiated groups were compared with unirradiated groups, there was higher predominance of type I collagen in both the experimental periods (7 and 14 days).
The present study assessed the action of LLLT on wound healing, with emphasis on type I and III collagen evaluation. When the euthyroid group was compared with hypothyroid groups, it was observed that in both experimental periods, the euthyroid group showed greater deposition of both collagen type I and type III collagen. However, the difference was statistically significant only among unirradiated control groups that were evaluated after 7 days, showing that the laser light was able to promote collagen deposition in hypothyroid rats irradiated with laser light similarly to rats without associated systemic dysfunction irradiated with laser light. Moreover, the comparison between euthyroid and hypothyroid groups irradiated with laser revealed no statistically significant difference among the groups, demonstrating that phototherapy was able to improve the healing process in a similar way in both groups, even in the presence of hypothyroidism. It is believed that this is because the biomodulative effect depends upon the physiologic status of the cell at the irradiation time, because cells with low redox potentials, such as in certain pathological conditions, become more sensitive to irradiation. This may explain why the biomodulative effect is not always detectable. 17
In comparison between the experimental periods of 7 and 14 days, it was observed that in both euthyroid and hypothyroid groups assessed at 14 days, the deposition of type I collagen was greater than that observed at 7 days. A higher percentage of type I collagen is important to the tissue, as it indicates that the state of collagen maturation is more advanced. 37 However, the excess type I collagen can be responsible for a healing of poor quality, showing hypertrophic appearance, but this undesirable effect can be minimized by applying correct dosages of laser irradiation in order to avoid overstimulation of fibroblastic activity. Furthermore, the predominance of type III collagen provides a fragile scar, but its presence together with type I collagen can allow a balance between characteristics of these collagen fibers in the newly formed tissue. 14,38
As no sign of excessive collagen synthesis was observed, it is possible to suppose that the protocol of photobiomodulation employed in this study was suitable to be applied in this experimental model. Also, the presence of both type III and I collagen, closely resembling the appearance of the normal tissue, seems to point out an important role played by LLLT in the architectural organization of the collagen during wound healing, as suggested in the literature. 14 However, the exact explanation for these results is not fully understood, so that further investigations are needed to elucidate the mechanisms underlying the observed effect in this study.
A similar in vivo study performed by Ramalho et al. 18 evaluated the influence of hypothyroidism and the effects of laser light (λ660 nm, 30 mW, ø3 mm) and polarized light (λ400–2000 nm, 40 mW, ø10 mm), adjusted to dosages of 20 and 40 J/cm2, on tissue repair. It was observed that laser light adjusted to 20 J/cm2 was more stimulating for collagen deposition in irradiated groups, but that there was no difference between the hypothyroid and euthyroid groups treated regarding the collagen amount. Moreover, the arrangement of collagen fibers in the hypothyroid group seemed to be a looser and more disorganized pattern than that in the euthyroid group.
The literature includes several studies with positive biomodulation results with the use of laser phototherapy on tissue repair. However, there is still controversy about the results observed. 15 Such discrepancies may be associated with the wide variety of experimental models available, method of assessing results, and variability of parameters used in irradiation protocols—such as differences in wavelength, energy density, power and irradiance, time and frequency of irradiation, and number of sessions—in addition to treatment conditions, making it difficult to compare studies. 6 Most of the studies in the literature associating this phototherapy to systemic involvement have been performed on healthy experimental models. Nevertheless, there is still no established best irradiation protocol and no consensus in the literature regarding the best dosage, potency, and application times.
Given the benefits offered by phototherapy and the need for tissue repair in patients affected by chronic lesions, investment in research on the therapeutic resources available to accelerate the healing process becomes increasingly necessary. These resources are of particular import to patients affected by a systemic dysfunction that interferes with the repair process. In time, these therapies may allow such patients to return as soon as possible to their work activities.
Conclusions
Our results indicate that hypothyroidism is related to wound healing delay and that laser light, used with the parameters of this investigation, increased type I collagen immunoexpression during the early phases of tissue repair. This information is, therefore, relevant, because it suggests that laser photobiomodulation improves newly formed tissue quality even in the absence of exogenous thyroid hormone intake.
Footnotes
Acknowledgments
The authors gratefully acknowledge the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and the Fundação de Amparo à Pesquisa do Estado da Bahia (Fapesb), for financial support.
Author Disclosure Statement
No competing financial interests exist.