
Abstract
Introduction
D
Excessive gingival display (EGD)–so-called “gummy smile”–can render a smile severe and unpleasant. 3,4 EGD is a clinical finding with many etiologies, 5 and may include extraoral or intraoral components. Some extraoral causes of a gummy smile are vertical maxillary excess (VME), hypermobile upper lip (HUL), or a short upper lip. VME can often be treated alone by orthognathic surgery. 6 Most patients who undergo this procedure require a hospital stay and a few days for recovery. Postoperative complications can include significant swelling, edema, bruising, and discomfort. 7 In some cases of VME, a multidisciplinary approach with either orthognathic surgery, orthodontic treatment, periodontal treatment, or restorative dentistry is required. 8 EGD can also be seen in patients with a short upper lip (measured from the subnasal to the inferior border of the upper lip). The average length of the maxillary lip is 20–22 mm in young adult females and 22–24 mm in young adult males. 9
HUL is considered to be the primary etiologic factor in EGD when the maxillary lip length is within a normal range and the lower third of the face is proportionate to the remaining thirds. HUL was defined as the amount of lip movement that occurs when the patients smile. This was calculated by subtracting the incisal exposure at rest from the dentogingival exposure during maximum smile. 5 HUL is caused by hyperfunction of the elevator muscle of the upper lip, and often results in EGD. In such cases, various treatment approaches have been used, with highly variable outcomes. Botulinum toxin, 10,11 lip elongation associated with rhinoplasty, 12 detachment of lip muscle, 13 partial removal, 14,15 lip repositioning, 16 –18 and lip repositioning combined with gingivectomy 19 are the reported treatment approaches.
Most of the surgeries associated with significant morbidity require hospitalization; a few week after botulinum toxin application, gingival display gradually increased. Therefore, lip repositioning is recommended as an alternative treatment for EGD.
The objective of lip repositioning is to minimize the gingival display by limiting the retraction of the elevator smile muscles (e.g., zygomaticus minor, levator anguli, orbicularis oris, and levator labii superioris). This procedure was originally described in the plastic surgery literature 30 years ago. 16
Because the different diagnosis brought different treatment modalities, for a correct diagnosis, a thorough examination must be performed. A flow chart that can help determine the correct etiology of a specific EGD case is shown in Fig. 1.

A flow chart to determine the correct etiology of excessive gingival display.
Currently, diode lasers are generally accepted and widely used as a tool for soft tissue management. 20,21 The energy level of the diode laser is absorbed by pigmentation in the soft tissues, making the diode laser an excellent hemostatic agent for soft tissue surgeries. 22 Other advantageous properties of diode lasers are relative ease of ablation of tissues, little wound contraction, minimal scarring, and less postoperative pain. 21,22 Therefore, the purpose of using lasers for the lip repositioning procedure [laser-assisted lip repositioning (LALR)] is reducing the reported pain, bruising, swelling, and discomfort reported in previous studies, 16 –18 with long-term aesthetic benefits. Because the worst part of undergoing the lip retraction surgical procedure reported in previous studies 16 –18 was the discomfort, pain, bruising, and swelling and the inability to move the lip during the early healing phase, 16 –18 laser-assisted surgery can be superior to conventional blade surgery because ablation, decontamination, and hemostasis are easier to achieve, and there is potentially less operative and postoperative pain, swelling, and bruising. 20 –22
Materials and Methods
Patient population
Ten female patients, ages 27.8±9.0 (range: 22–34 years) were enrolled in the study. The participants were chosen among individuals who were referred to the Bezmialem Vakif University, Department of Periodontology and Orthodontics with the chief complaint of the excessive display of gums while smiling. After a thorough extraoral and intraoral examination, patients diagnosed with HUL were informed about LALR treatment's method, risks, and potential benefits.
Inclusion criteria were as follows: patients needed to be adults (≥18 years), in good periodontal and systemic health with no contraindications for periodontal surgery, nonsmokers, with maxillary anterior teeth of normal dimensions, 23 and normal upper lip length (females: 20–22 mm; males: 22–24 mm), 24 hyperactive upper lip (lip mobility>8 mm), 8 and ≥3 mm continuous band smile line at anterior, left, and right posterior regions.
LALR
The operator, patient, and assistant wore safety glasses. Highly reflective instruments or instruments with mirrored surfaces were avoided, as there could be reflection of the laser beam. Care was taken to avoid using laser in presence of explosive gases. The surgical treatment was performed by the same periodontist (S.Ö), as described by the Rubinstein and Kostianovsky 16 technique. Anesthesia was achieved by local infiltration (2% lidocaine with 1:100.000 epinephrine). The surgical area was outlined using an indelible pencil (Fig. 2A). The procedure was initiated with a diode laser, a wavelength of 940 nm, 4 W, continuous wave (cw) mode and 300 mm tip, by making a partial-thickness incision following the mucogingival junction extending from the right first molar to the left first molar (Fig. 2B). The procedure was repeated on the contralateral side. Followed by the vertical laser incisions, another second horizontal incision parallel to first was made in the labial mucosa 10–12 mm apical to mucogingival junction. These two laser incisions were connected at each end by creating an elliptical pattern.
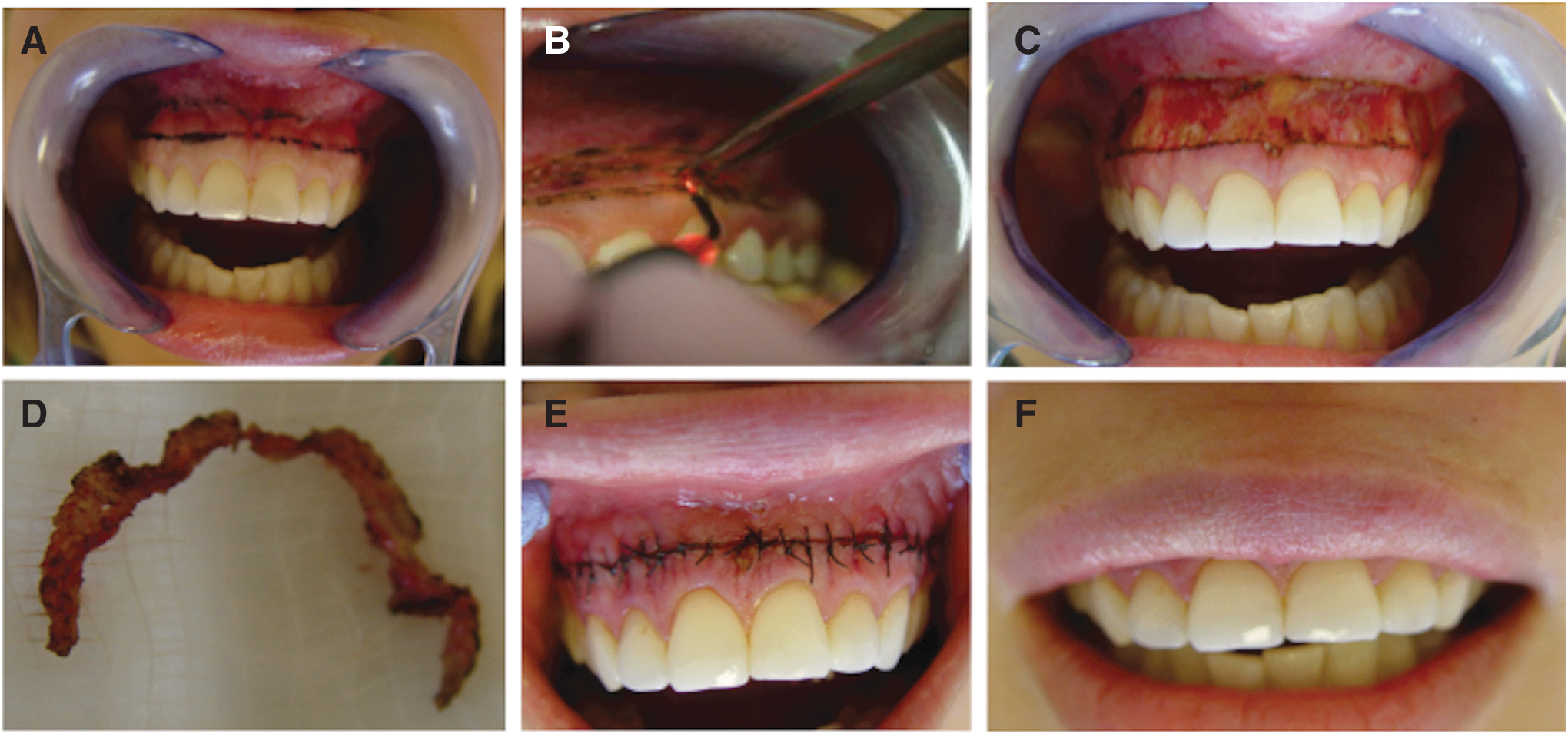
The partial-thickness flap was excised leaving the underlying connective tissue exposed to the oral cavity (Fig. 2C). The strip of outlined mucosa (Fig. 2D) was removed by laser dissection, leaving the connective tissue exposed. The diode laser does not cut the periosteum, but small horizontal movements must be performed to prevent thermal damage. Continuous interlocking 5-0 sutures (Ethicon, Johnson & Johnson nylon monofilament) were then used to stabilize the new mucosal margin to the gingiva (Fig. 2 E,F). Patients were recalled 1 week after the surgery to report any postoperative complications.
It is noteworthy that the amount of partial-thickness flap excised should be either double the amount of gingival display that needs to be reduced or a maximum of 10–12 mm tissue excision, in order to prevent the involvement of labial minor salivary glands, severing of which may lead to the formation of mucocele.
Postoperative protocol
Patients were prescribed ibuprofen as needed, and instructed to use 0.12% chlorhexidine rinse twice daily for 1 week. They were also instructed to consume only soft foods during the 1st week, to avoid any other mechanical trauma to the treated sites, and to minimize lip movement when smiling or talking during the first 2 weeks postoperatively. Patients were recalled every 3 months, until the final examination.
Initial therapy and clinic measurements
One week prior to starting the surgery, a session of prophylaxis was performed (mechanical treatment).
The following parameters were assessed during active smile, with a mm ruler in place, at the baseline (before the surgery), and 6 and 12 months after surgery, and were recorded to the nearest millimeter: the amount of gingival display from the inferior border of the upper lip vermillion to the gingival margin of the midbuccal central left incisor, and the mid-buccal gingival margin of left and right second premolar. When the lip covered part of the clinical crown (postoperatively), the amount of gingival display was set at zero. All measurements were recorded to the nearest millimeter over the midbuccal of the left central incisor, and the left and right midbuccal of the second premolars.
Surveys were given to the subjects 1 year after the procedure. The surveys included both a Likert scale and open-ended questions. The questions addressed subject satisfaction with smile, amount of gingiva displayed, best and worst aspect of the procedure, and whether subjects would undergo the procedure again (Table 1).
Questions and responses for the patients before the treatment and 12 months after the procedure.
Patient evaluation of postoperative condition and aesthetics
The postoperative discomfort and aesthetics were evaluated by the patients on a 100 mm visual analog scale (VAS). 25 The questionnaire was divided into two parts: the first part, regarding the postoperative morbidity and pain, was completed 1 week after surgery (VAS-P) (0 indicating very bad, 50 indicating average, and 100 indicating an excellent postoperative course), and the second part, concerning patient satisfaction with the aesthetic outcome, was completed at the 12-month follow-up (VAS-E) (0 indicating very bad, 50 indicating average, and 100 indicating excellent). 25,26
Statistical analysis
Data analysis was accomplished on SPSS software version 10.0. For all parametric variables, repeated measures ANOVA was used for examination of mean differences between baseline, 6 months, and 12 months. Results were presented as mean±SD. A p value<0.05 was considered as significant.
Examiner reproducibility
One examiner performed the clinical measurements and also assessed all patient related outcomes of treatment. To determine examiner reliability, parameters were measured in triplicate over 3 weeks; the coefficient of variation for all three parameters was 3%. 27
Results
All patients completed the study. None dropped out. Ten patients, mean age 27.8±9.0 (range: 22–34 years) were treated with LALR surgery. Postoperative healing was uneventful for all study participants. A minor scar was formed on the suture line but it was not apparent during the smile. All patients were systemically healthy and nonsmokers. Tables 1, 2, and 3 summarize the parameters of treatment modalities.
Distribution of anterior, right posterior, and left posterior gingival display at baseline (preoperatively), and 6 and 12 months postoperatively.
Difference between time periods; between baseline, 6th month and 12th month, a p value<0.0001 (ANOVA).
AGD, anterior gingival display; RPGD, right posterior gingival display; LPDG, left posterior gingival display.
Distribution of VAS aesthetic at 12 months postoperatively and VAS pain during the postoperative period.
LALR, laser-assisted lip repositioning.
Anterior gingival display at baseline was 4.3±1.8 mm and changed significantly (p<0.0001) at 6 and 12 months postoperatively (Table 2). At 6 and 12 months, gingival display was 1.1±1.0 and 1.2±1.5 mm, respectively. The baseline gingival display differed significantly from that at both 6 and 12 months (p<0.01), which did not differ from each other. There was no significant difference in gingival display between 6 and 12 months.
Right posterior gingival display also varied significantly from 5.0±1.4 mm at baseline to 1.2±1.0 mm at 6 months and 1.3±1.1 mm at 12 months (p<0.0001). The baseline gingival display differed significantly from that at both 6 and 12 months (p<0.01), which latter did not differ from each other.
Left posterior gingival display at baseline was 4.9±2.2 mm (range: 4–7 mm) and changed significantly (p<0.0001) at 6 and 12 months postoperatively (Table 1). At 6 and 12 months, gingival display was 1.1±1.0 and 1.2±1.4 mm, respectively (Table 2). There was no difference in gingival display between 6 and 12 months
All patients completed the survey. Preoperatively, the majority of patients were not satisfied with their smile or the amount of gingival display, whereas the opposite was true postoperatively (Table 1), (VAS aesthetic) (Table 3). Patient satisfaction with aesthetics was very high. Postoperatively, 100% of subjects considered the amount of displayed gingiva to be “about right,” whereas preoperatively, 100% had considered it to be “way too much” (Table 1).
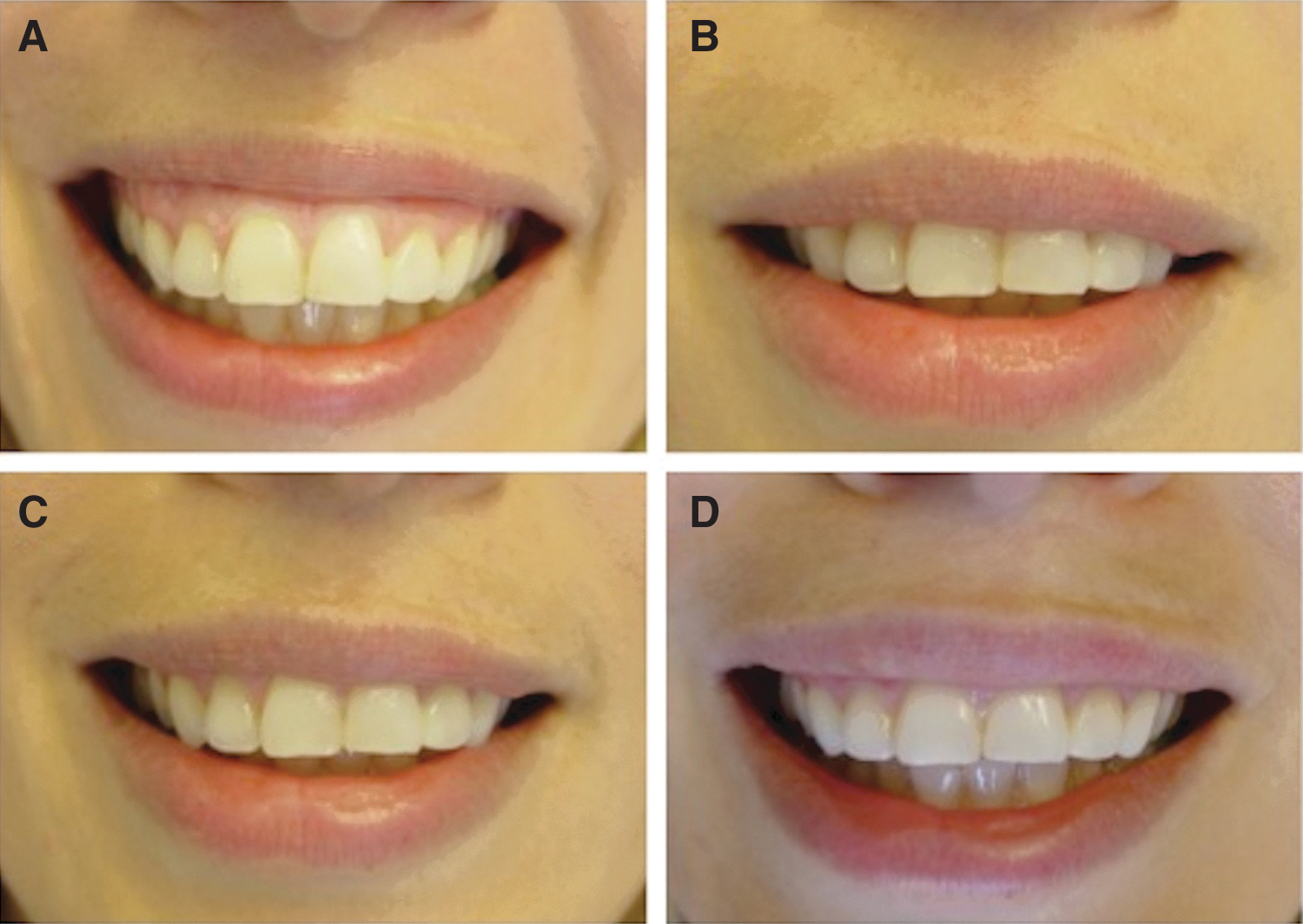
These results were compatible with the gingival display measurements. Preoperative image of the dynamic smile, the amount of gingival exposure on the 7th postoperative day and at 6 and 12 months are illustrated in Fig. 3 A–D. The 1st postoperative week, patients felt rarely discomfort and pain (VAS pain) (Table 3). Considering the procedure and postoperative experience, all of the patients said that they would likely choose to undergo the procedure again (Table 1).
Discussion
This case series reports the procedure, and the clinical and the patient-centered outcomes of an LALR technique, which is designed for the management of EGD.
The results showed that the LALR procedure successfully reduced the preoperative gingival display in all cases, with low morbidity, and that results were stable for the 12 months of follow-up. Patient satisfaction was high 1 year after the surgery. To the best of our knowledge, this is the first study to report on lip repositioning surgery with laser-assisted, clinical, or patient-centered outcomes.
Investigations have shown that minimal gingival display during smile is considered more attractive. The amount of gingival display that is considered attractive is 1–2 mm. 28 All the cases treated in this study had baseline gingival display ≥3 mm at the anterior region, and ≥4 mm at the posterior region. Using a criterion of ≤2 mm of postoperative gingival display, the lip repositioning surgery was successful in all of the patients. Although the results of lip repositioning surgery appear stable for up to 1 year postoperatively, longer follow-up periods are necessary to establish the long-term success of this procedure.
The literature is mostly composed of the case reports of different treatment options for “gummy smile,” depending upon the etiology, but it is lacking in outcome studies. Case reports can found for the treatment of delayed passive eruption with aesthetic crown lengthening 29 and for the treatment of excessive maxillary growth with orthognathic surgery. 30
Cosmetic surgeons Rubinstein and Kostianovsky 16 originally described the treatment of a gummy smile caused by a hypermobile lip by lip repositioning. Once this surgical procedure was compared with orthognathic surgery, it was found to be less aggressive, and was thought to have fewer postoperative complications. Litton and Fournier 13 advocated the procedure again for the correction of EGD in the presence of a short upper lip. This was accomplished by detaching the muscles from the bony structures to coronally position the upper lip, and no complications were reported. Miskinyar 14 modified the original technique, 16 but did not report when or how much relapse had occurred. The treatment group consisted of seven patients who had to have repeat surgery, and a more aggressive approach was used, which included myectomy and a partial resection of the levator labii superioris, with nerve repositioning before amputation of the muscle. Muscle resection was thought to eliminate muscle regeneration, making the results more permanent. The author reported that one patient experienced postoperative parasthesia that lasted 2.5 months.
In cases of “gummy smile” associated with hyperactive upper lip, outcomes have been reported for treatments with botulinum toxin 31 and myotomy. 15 Polo 31 treated 30 patients for gummy smile with botulinum toxin type A and performed followed-up evaluations at 2, 4, 8, 12, 16, 20, and 24 weeks postinjection. Although the baseline gingival display decreased significantly at 2 weeks, gingival display gradually increased after 2 weeks and the author predicted a return to baseline values at 30–32 weeks postinjection 31 ; no other clinical parameters were assessed in that study. Patients always prefer these injections because of postoperative complications and the difficulty of the surgery. In our treatment group, using laser for incisions eliminated the postoperative complications, which were reported in previous studies. 16 –18
Ishida et al. 15 described a combined approach of myotomy of the levator labii superioris muscle, subperiosteal dissection of the gingiva, subcutaneous dissection of the lip, and frenectomy for correction of gummy smile in 14 female patients. And the authors reported good results at 6 months. It appears that the three treatment modalities (botulinum toxin, myotomy, and modified lip repositioning surgery) provided similar benefits in terms of gingival display reduction, at least at the early time points. However, EGD treatment with botulinum toxin requires frequent repeat injections to maintain the desired outcome.
Rosenblatt and Simon, 17 and Simon et al. 18 used an elliptical-shaped incision at the mucogingival junction and the alveolar mucosa, reflected a partial-thickness flap, and excised 10–12 mm of epithelium. The authors described good results and one study 17 reported an 8-month follow-up. But lip-repositioning surgery is accompanied by limited morbidity, with mucocele formation. 17,18
Between the two surgical approaches, myotomy is the much more aggressive procedure, with irreversible outcomes and greater potential postoperative morbidity, such as paresthesia. 14 In contrast, lip repositioning is a less aggressive surgery. The most common complications of lip repositioning surgery reported in the literature were postoperative bruising, pain, discomfort, and swelling of the upper lip, 32 but in this study, none of the patients had similar complaints, probably because of the advantages of lasers. However, possible damaging thermal effects to the underlying tissues should be kept in mind when using lasers deep in the tissues. It is well documented that the scattering of laser energy within the surrounding tissues is low, and that the layer of heat-altered tissue that remains after vaporization is relatively shallow. 33
As diode lasers have an excellent soft tissue ablation capacity, the laser used in the surgery reported here performed a precise and nontraumatic de-epithelization. In addition, the laser-assisted technique used here may shorten the duration of early healing. Other advantages of the use of a diode laser include a relatively bloodless operative and postoperative field, a less traumatic operation, greater accuracy in making incisions, sterilization of the surgical field, minimal swelling and scarring, vaporization, and cutting with much less postoperative pain. This could provide potential advantages for the surgery, the healing process, and the patients' perceptions of the procedure. Silva et al. treated 13 patients for gummy smile with lip repositioning technique, and 92% of the subjects said that they would likely choose to undergo the procedure again. 34 But in our study, considering the overall experience (the procedure, the postoperative course and the outcome), all of the subjects said that they would likely choose to undergo the procedure again. The surgery can be less invasive, take less time, and be less demanding, and patients could benefit from a procedure with potentially reduced intra- and postoperative morbidity. Lasers have also been known to stimulate growth factors, which enhances the activation of human gingival fibroblasts to proliferate and release growth factors in tissues; therefore, this may have also had an impact on our positive findings for the laser therapy. 35
Conclusions
The current study indicates that after a 12-month follow-up, the LALR procedure can produce stable results. This can be considered to be short-term evidence of its usefulness. A proper diagnosis and case selection are essential before considering this procedure. For patients desiring a less invasive alternative to orthognathic surgery and lip repositioning surgery, LALR is a viable alternative. Long-term follow-up studies are needed to evaluate the stability and effectiveness of LALR as a treatment modality. This technique has an edge over other techniques because it is simple and effective, requires minimal instrumentation, is less time consuming and less invasive (compared with other techniques), and is cost effective and easy to perform with excellent postoperative results, faster healing, and patient satisfaction.
Footnotes
Author Disclosure Statement
No competing financial interests exist.