
Abstract
Introduction
W
Many attempts to alter the surface characteristics of the porcelain and to develop better techniques for bonding have been reported. 3 –5 Generally, mechanical (roughening the surface with a diamond bur or micro-etching with aluminum oxide particles), 6 chemical (orthophosphoric acid, hydrofluoric acid, and acidulated phosphate fluoride), or combination methods have been suggested. 7,8 Clinical applications of these methods have various advantages and disadvantages. 9
With advances in science and technology, the applications of lasers in dentistry have increased. Different types of laser, such as carbon dioxide (CO2) laser, neodymium-doped yttrium aluminium garnet (Nd:YAG) laser, erbium-doped yttrium aluminium garnet (Er:YAG) laser, and erbium, chromium: yttrium-scandium-gallium-garnet (Er:Cr;YSGG) laser, have been used in orthodontics for conditioning enamel before bonding brackets, and all have shown acceptable results. 3,10 However, only one study of the bond strength of brackets using a femtosecond laser to treat human enamel has been reported. 10 Few studies of porcelain surface treatment by different laser techniques have been performed. An and Sohn and Akova et al. showed that 2W/20 sec super pulse CO2 laser irradiation provided acceptable bond strength of metal brackets to porcelain surfaces. 5,11 Poosti et al. reported that Nd:YAG laser irradiation was an acceptable substitute for hydrofluoric acid but that the Er:YAG laser was not. 12 A literature search yielded no reports of the performance of femtosecond (FS) lasers in comparison with other conventional techniques for improving the bond strength of orthodontic brackets to porcelain surfaces.
Therefore, the purpose of this study was to investigate the effects of FS laser treatment on the shear bond strength (SBS) of a metal bracket to prepared porcelain surface and to compare it with other surface treatment techniques [50 μm Al2O3 sandblasting (SB), 9.6% hydrofluoric acid gel (HF), and Nd:YAG (NY) laser]. The null hypothesis was that no difference would be found among the effects of the porcelain surface treatment techniques used in the study.
Materials and Methods
Eighty feldspathic porcelain specimens (Ceramco, Dentsply, York, PA; Heraus Kulzer, Hanau, Germany) were fabricated and then trimmed to 10×10×4 mm in size. The samples were embedded in a 20 mm height and 25 mm diameter PVC ring using an autopolymerizing acrylic resin block. The area (4.5×4 mm) in the center of the specimens was roughened with a yellow-label diamond bur to remove the glaze layer. Prior to the bonding of the brackets, the specimens were randomly assigned into four groups (n=20) (Fig. 1).
A computer-controlled femtosecond laser micromachining system (Quantronix, QMark system).
The surface treatment procedures were as follows.
Group SB
In this group, 50 μm grain-sized Al2O3 was used during sandblasting for 3 sec at 2 bar (BEGO Easyblast, Bremen, Germany). The distance between the tip of handpiece and the porcelain surface was adjusted to 10 mm using a special holder attached to the handpiece. The handpiece was kept perpendicular to the porcelain surface.
Group HF
In this group, the specimens were conditioned with 9.6% HF gel (Porcelain Etch Gel, Pulpdent Corp., Watertown, MA) for 4 min, rinsed with distilled water for 1.5 min, and finally air dried.
Group NY
The surfaces were painted in an area of 4.5×4 mm with a black acetate pen, to increase laser absorption, to prevent transmission of the laser beam, and to determine the laser irradiation borders. The laser beam (λ=1064 nm; Fotona Lightwalker, Slovenia, EU) from the Nd:YAG laser was delivered using a 300 μm diameter optical fiber perpendicular to the porcelain surface. The output settings were 4 W and medium-short pulse (MSP) mode, and the pulse repetition rate was 40 Hz. The pulse duration was 100 μs, and the energy density was 0.354 J/cm2. Nd:YAG laser irradiation was performed in a water-filled plastic cup for cooling. The tip was moved across the surface in a scan at 1 mm/sec for 20 sec with 1 mm from the surface.
Group FS
FS laser pulses (λ=800 nm) from an amplifier (Quantronix Integra-C-3.5, NY) were applied to a deglazed surface. The FS laser parameters were as follows. The laser delivered pulses at 3.5 mJ per pulse and a beam splitter was used to split the beam into two arms, one of which had 750 mW per pulse and was directed at the sample surface. The wavelength of the laser beam was 800 nm, with pulses at 90 fs, and a 1 kHz repetition rate. The pulse duration was 90 fs, and the energy density was 2033 J/cm2. The laser beam was delivered to the porcelain surface using a laser marker (Q-Mark, Quantronix, NY) system that had a back focal length of 11 cm (the distance between the cover glass of the F-theta lens of the marking system and the paraxial focal point) and could scan the work plane at various scanning speeds, controlled by the software.
Bonding procedure
After surface conditioning, all specimens were cleaned for 380 sec in an ultrasonic cleaner, and were air dried in air stream before bonding. After all sample-surface-conditioning steps were completed, one sample from each group was selected randomly, and the porcelain surface was examined by scanning electron microscopy (SEM) (Jeol JMS-6390LV, Jeol Ltd., Tokyo) (Fig. 2).
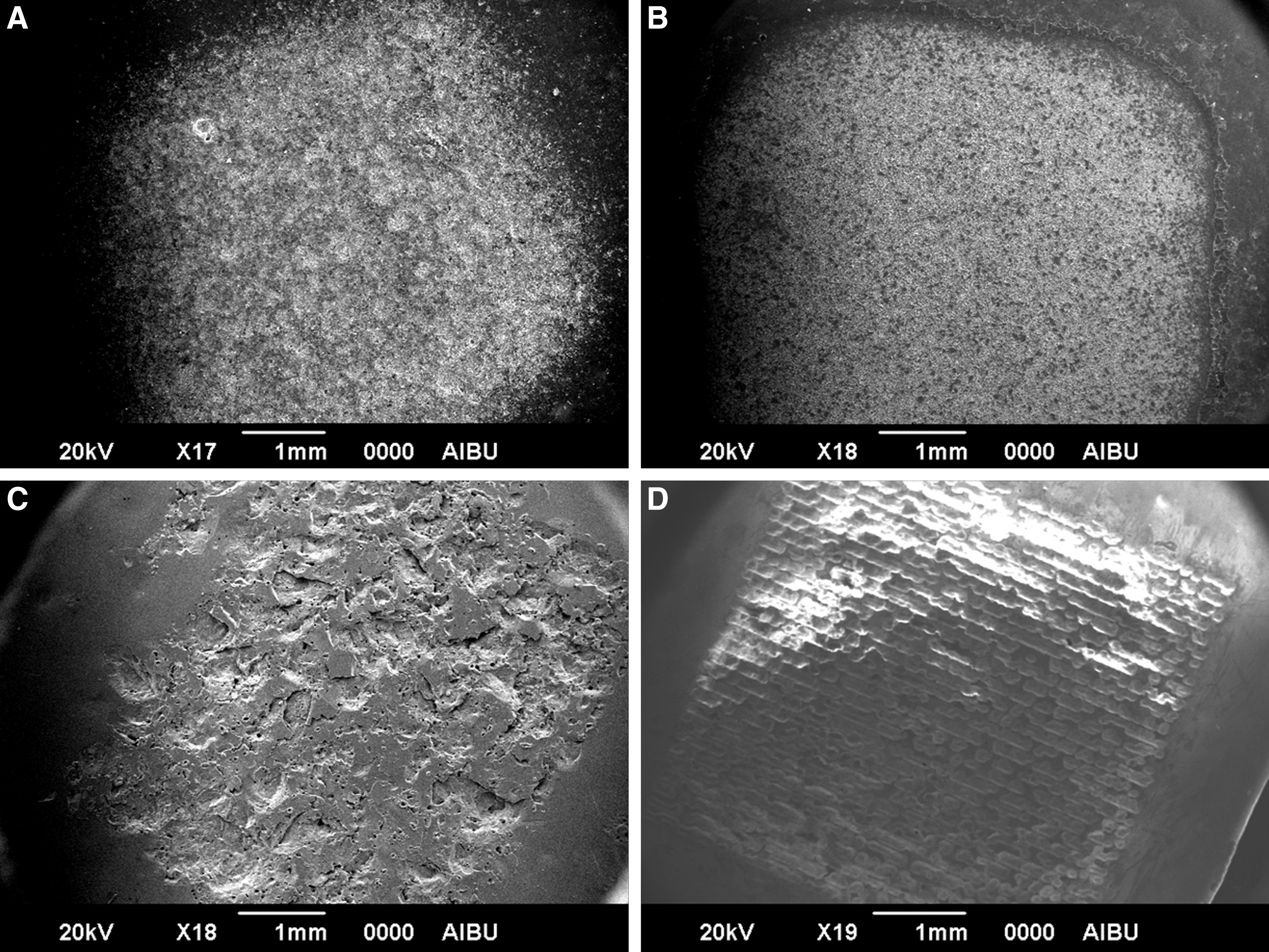
Before the shear bond strength (SBS) testing, scanning electron micrographic (SEM) images of treated specimens from each group. (
Stainless steel standard edgewise maxillary central incisor brackets with a 0.55 mm slot (Dentaurum, Ispringen, Germany) were used. During the bonding procedure, a silane-coating agent (Monobond S, Ivoclar Vivadent, Schaan, Liechtenstein) was applied to the porcelain surface according to the manufacturer's instructions. Opal Bond MV adhesive (Opal Orthodontics, South Jordan, UT) was applied to the base, and the bracket was bonded to the center of the porcelain specimens. Excess adhesive material was removed from the borderline of the bracket with an explorer, and the specimen was light cured with a 3 sec exposure directly over the labial face of the bracket, followed later by a second exposure, for a total of 6 sec, using a LED curing unit (Valo Ortho Cordless, Ultradent Products, Inc., South Jordan, UT)
After the brackets were bonded to the porcelain surfaces, the specimens were stored in distilled water at 37°C and then thermocycled for 500 cycles between 5° and 55°C, using a dwell time of 30 and 3 sec expected time.
The SBS of the brackets were tested with a universal testing machine (Shimadzu AGS-X, Shimadzu Corp., Tokyo, Japan) at a crosshead speed of 1 mm/min until bonding failure occurred (Fig. 3). A fractured specimen from each group was examined by SEM (Fig. 4).

Shear bond strength test.
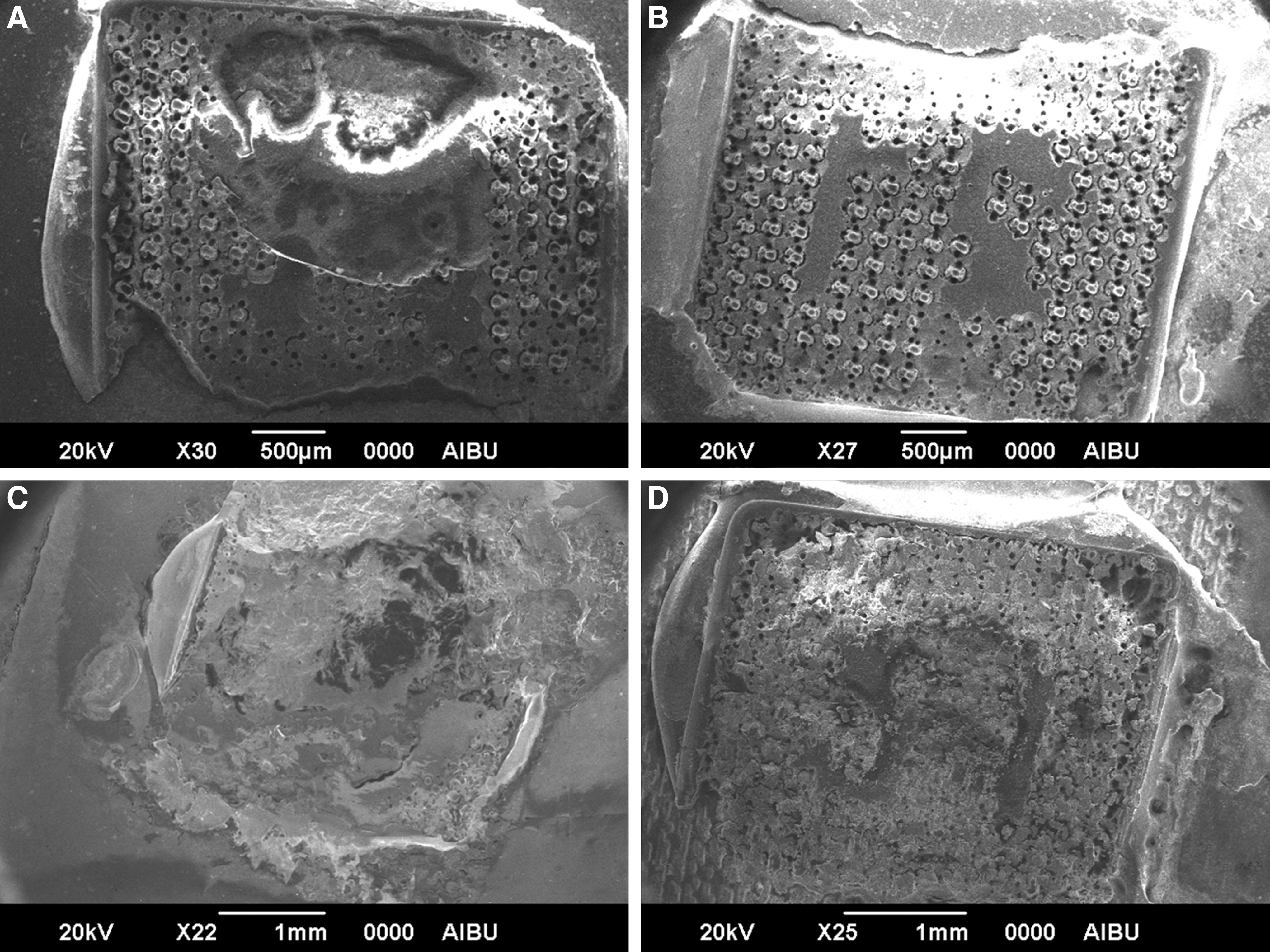
After the shear bond strength (SBS) testing, scanning electron micrographic (SEM) images of fractured specimens from each group. (
After the specimens were tested and removed from the testing apparatus, the fracture sites were observed using a stereomicroscope (SZTP; Olympus, Tokyo, Japan) at 40×magnifications, to identify the mode of failure. The fractured surface was classified as one of four types: 13
Type 1: Adhesive failure, between the adhesive layer and the porcelain surface
Type 2: Mixed failure, failure in the resin layer
Type 3: Cohesive failure, fracture in the porcelain
Type 4: Adhesive failure, between the adhesive layer and the bracket
The ultimate stress (MPa) of the bracket–adhesive cement–porcelain bonds were calculated as follows
14
:
The SBS values were analyzed using the SPSS software (ver. 11.5; SPSS, Chicago, IL). One way analysis of variance (ANOVA) was used to assess the data for differences. The Tamhane test was used to perform multiple comparisons among results at a significance level of p<0.05.
Results
The mean SBS values, their standard deviations, and the distribution of bond strengths of all surface treatment groups are shown in Table 1. The results obtained using one way ANOVA indicated that the SBS values varied according to the surface treatment method (p<0.001; Table 2).
Group SB, sandblasting; Group HF, hydrofluoric acid; Group NY, Nd:YAG laser; Group FS, femtosecond laser.
Groups with different letters are statistically significantly different.
Results of the Tamhane post-hoc tests indicated that the bond strength in Group NY was significantly lower than in the other groups (p<0.05). There were no statistically significant differences among Groups SB, HF, and FS (p=0.28).
Bond failure modes are presented in Table 3. There was a high frequency of fracture of adhesive between the bracket and resin cement (Type 4), particularly in group FS (80%). Mixed failure was the most prevalent type in Group NY, ∼65%. Group SB showed 40% cohesive failure (in the ceramic) and 30% adhesive failure between the bracket and resin cement. These were also the most common failure modes in Group HF; adhesive (40%) and cohesive (45%).
Type 1: adhesive failure, between the adhesive layer and the porcelain surface; Type 2: mixed failure, failure in the resin layer; Type 3: cohesive failure, fracture in the porcelain; Type 4: adhesive failure, between the adhesive layer and the bracket.
Group SB, sandblasting; Group HF, hydrofluoric acid; Group NY, Nd:YAG laser; Group FS, femtosecond laser.
Discussion
In the current study, the effects of FS laser treatment on the SBS of a bracket to prepared porcelain surface with different surface treatment techniques (50 μm Al2O3 sand, 9.6% hydrofluoric acid gel, Nd:YAG laser, FS laser) were evaluated. The FS laser treatment played an important role in the bond strength of the bracket to porcelain. However, the SBS of porcelain treated with a Nd:YAG laser (5.11 MPa) was found to be lower than the acceptable value (6–10 MPa). 15
In patients undergoing porcelain restorations, adhesion of the bracket to the porcelain surface is of great importance, because orthodontic forces are transmitted to the tooth via the brackets. A porcelain surface having a glaze layer does not provide for proper adhesion of bracket to the feldspathic porcelain surface. 1 The subject of whether and how to deglaze porcelain to achieve adequate bond strength with the bracket has been debated for many years. Several in vitro studies have shown that glazed porcelain treated with silane does result in adequate bond strength. 16 In contrast, Zachrisson et al. stated that the bond strength to glazed and deglazed porcelain surface showed no significant difference. 17 Also, destruction of the glaze layer leads to irreversible damage, such as water and other liquid absorption, bacterial plaque accommodation, and porcelain fractures during debonding. 18,19 Smith et al. 2 stated that glazed porcelain surfaces disallow resin penetration to the bonding surface. In our study, before surface treatment, deglazing was performed with yellow-label burs on the porcelain surface (4.5×4 mm center area). Before the bonding procedure, application of silane is required for a chemical link between the porcelain surface and composite resin. 20 Kocadereli et al. 21 stated that using silane improved the bond strength of bracket to porcelain surface. For this reason, in this study, a silane-coating agent was applied beforehand, for bracket bonding.
To increase the mechanical interlock with the composite resin, the porcelain surface can be etched. 22 HF etching has been used to improve the bond strength of feldspathic porcelain. 23,24 The most widely used etching agent is 9.6% HF acid (gel form) for 2–4 min. 25 Therefore, in this study, 9.6% HF acid gel was used for 4 min. The results showed that HF treatment did provide sufficient bond strength (9.09 MPa). A study conducted by Huang and Kao, 26 who was used 9.6% HF acid gel on porcelain surface, reported that SBS value of bracket to porcelain surface was 10.49 MPa. This finding is similar to that of the current study. However, these results were not consistent with a previous report that the SBS of an SB porcelain surface was higher than that after HF treatment. 27 Using HF may also lead to damage to soft tissue. Therefore, the orthodontist must be careful during HF application. 17 Aluminum oxide sandblasting has been widely used to promote micromechanical retention of ceramics (madani 2000). Many studies 27,28 have shown that Al2O3 sandblasting, combined with silane, significantly increased the bond strength of bracket-to-porcelain surface. Girish et al. 27 showed that 50 μm Al2O3 SB for 10 sec without thermocycling enhanced to SBS value (15.18 MPa). This finding is concurrent with results from the current study, because thermocycle can decrease the SBS value. However, Abdelnaby 28 reported that 50 μm Al2O3 SB porcelain surface with thermocycling provided a 6.95 MPa SBS value. In the current study, the SBS values of the HF and SB groups showed no significant difference, and similar bond failure modes. Therefore, given the similar results and the possibility of harmful and irritating effects of HF, some authors have suggested that sandblasting combined with silane application is preferable. 29
Laser technology has been used in dentistry since 1988 for a variety of techniques. 30 Fornaini et al. 31 stated that dental lasers of several wavelengths can be used for different applications, such as intra-oral welding, frenectomy, enamel conditioning, and bracket bonding and debonding. Numerous studies have shown that NY laser use is an effective technique for bracket adhesion. 32,33 In a recent study, an NY with a 4 W output power, 40 Hz repetition rate, and 300 μm diameter optical fiber was used for surface treatment. In the current study, the SBS value of the NY group (5.11 MPa) was the lowest among the groups, which was not adequate for clinical application (6–10 MPa). 15 This finding is consistent with the results of Hosseini et al. 33 It has been reported that a gradual increase in the output power of NY lasers improved the SBS of the bracket-to-porcelain surface. In contrast, Poosti et al. 12 reported the SBS of bracket-to-porcelain surface to be 6.9 MPa, using a 0.8 W NY laser. This result can arise from ceramics that effectively absorb the 1064 nm wavelength energy emitted by an NY laser. Considering other studies, in the current study, the porcelain surface was painted to restrict laser beam transmission to within the porcelain, and to reduce the temperature increase, laser treatment was performed in a cup of water.
The use of FS laser pulses in dentistry is increasing gradually. 10,34 The current study is the first reported study to examine the SBS of the bracket-to-feldspathic porcelain surface using a FS laser treatment in comparison with other conventional surface treatment methods. According to results of the study, the FS laser treatment showed high SBS value (11.6 MPa), and can be considered as a reliable and effective technique in orthodontic treatment.
In contrast to the other groups, the FS surface treatment produced extensive surface fissuring, which was more homogenous and had more regular surface characteristics. Although ceramic surface treatments using conventional methods can produce undesired results, such as crack propagation and surface heating, recent studies have shown that FS laser pulses promise a gentler, more precise, and clear surface machining without heating effect. 35,36 This technique is also able to ablate material in thin layers at the surface without changing the properties of the material. 37 The depth and shape of the surface can be readily formed using appropriate software. Use of different speeds, numbers of repetitions (passes through the same point), laser repetition rates (kHz), and laser pulse powers affect the depth and width of the craters. The high standard deviation value achieved in SBS test, ∼35% of the mean value, may be dependent upon these craters on the surface. Although many more craters and fissures could be formed in this study, cohesive bond failure was observed in 5% of cases. However, in 80% of cases, adhesive failure between bracket base and resin cement were observed as result the high bond strength of the resin layer to porcelain surface. This is consistent with the results obtained in the bond failure mode, which showed that the strength of the resin layer to porcelain surface bond with FS treatment was higher than in the other groups.
Under clinical conditions, type 2 and 4 failures result in the least damage for porcelain surface, because the remaining resin can be polished. When viewed from this angle, Group FS (n=16) can be more tolerant of porcelain repair after the post-orthodontic treatment. In scanning electron micrographs, Groups SB and HF exhibited similar surface roughness; however, Group NY showed irregular craters. When compared with the other groups, Group FS exhibited several symmetrical cavities on the surface (Fig. 2). After the SBS test, cohesive fracture in the porcelain surface was observed in Group NY. On the other hand, Groups HF and FS exhibited adhesive fracture failures (Fig. 4).
If FS lasers will be used under clinical conditions in the future, they might be the clinician's preference, because of their precise and effective properties. However, further studies are required to bring about their clinical use.
Conclusions
FS laser treatment is a new method for bonding a bracket to a prepared porcelain surface. The results of this study showed that FS laser treatment produced high SBS of the processes assessed; therefore, it appears to be an effective method for bonding orthodontic metal brackets to prepared porcelain surfaces. In future studies, the effects of different surface treatments on porcelain system strength should be investigated more thoroughly.
Footnotes
Acknowledgments
The authors acknowledge the Abant İzzet Baysal University, Art and Science Faculty-Physics Department for preparing SEM images of the samples; Dr Tugrul Sari, Bezmialem Vakif University, Faculty of Dentistry for the Fotona Laser and thermocycle devices; Advanced Technology Research and Application Center (İL-TEK) for FS laser facilities, and the staff at the Department of Physics, Faculty of Science, Selçuk University, for their assistance.
Author Disclosure Statement
No competing financial interests exist.