
Abstract
Introduction
P
The Neodymium: Yttrium-Aluminum-Garnet (Nd:YAG) laser is a free-running pulsed wave laser with a wavelength of 1064 nm. Unlike CO2 (10,600 nm) and Er:YAG (2940 nm) lasers, the Nd:YAG laser has low absorption in water, and the energy scatters or penetrates into the biological tissues. Because of the characteristics of penetration and thermogenesis, the Nd:YAG laser produced a relatively thick coagulation layer on the lased soft tissue surface, and thereby showed strong hemostasis. The width of the coagulation layer was demonstrated from 0.27 to 0.62 mm in an incision of bovine oral soft tissue in vitro with 3 and 5 W power outputs of Nd:YAG laser. 10 White et al. 11 also has successfully used the Nd:YAG laser for intraoral soft tissue application without anesthesia, and with minimal bleeding compared with scalpel surgery. Additionally, the United States Food and Drug Administration has approved the application of the Nd:YAG for sulcular debridement or soft tissue curettage since 1997. 12 The Nd:YAG laser with a flexible optical fiber with a contact tip of 200∼400μm is suitable for pocket insertion. Basic research 13,14 and clinical trials 15 –18 have been performed on periodontal pocket curettage and root surface debridement.
A procedure called laser excisional new attachment procedure (ENAP) with Nd:YAG laser has been reported in trade journals with examples of radiographic bone regeneration. 19,20 Referred to as the laser-assisted new attachment procedure (LANAP) in this report, this technique of pocket therapy has recently been approved by the United States Food and Drug Administration. 21 Additionally, in the treatment of moderate to severe periodontal disease using LANAP, Yukna et al. 22 demonstrated that new connective tissue attachment (CTA), and regeneration of root surface (cementum) was achieved in a human histology study using the Nd:YAG laser. However, the American Academy of Periodontology mentioned that not enough randomized blinded controlled longitudinal clinical trials, cohort or longitudinal studies, or case-controlled studies could prove that LANAP or laser curettage offered any advantageous clinical result not achieved by traditional periodontal therapy. 23 Moreover, the mechanism of LANAP and laser curettage, such as morphologic alterations of periodontal pocket epithelium following laser irradiation, is still unclear.
Numerous studies have considered surface alterations of cementum and dentin induced by various laser wavelengths, primarily CO2, Nd:YAG, Er:YAG, and diode laser. 9 Likewise, we consider that alterations in epithelial morphology (i.e., number of cell layers, spatial relationships, overall integrity, or complete removal) following laser irradiation is another important factor that may affect healing of the periodontal pocket. Clinical and morphologic features of human pocket epithelium in periodontitis have been described in detail by scanning and transmission electron microscopy. 24 –28 Additionally, several studies have evaluated the changes in gingival histology following instrumentation by conventional subgingival curettage, 29 or use of the CO2 (8 W), 30 Nd:YAG (1.25 and 1.75 W), 31 or diode lasers (2 and 4 W). 32 However, morphologic alterations in human periodontal pocket epithelium following laser irradiation have not been evaluated clearly. Therefore, the purpose of this in vivo study was to examine the morphologic characteristics of pocket epithelium at different PD and with presence or absence of clinical inflammation [bleeding on probing (BOP)±] following the use of an Nd:YAG laser by scanning electron microscopy (SEM) and histologic finding.
Materials and Methods
Subjects
Twenty patients with chronic periodontitis of moderate severity, planned for extraction of unviable teeth or periodontal surgery, were selected for the study. There were 11 male and 9 female patients ranging in age from 47 to 79 years, with a mean age of 61.5 years (Table 1). Exclusion criteria for patients were systemic diseases related to infectious endocarditis prophylaxis, diabetes mellitus, antibiotic therapy during the previous 6 months, and steroid or radiation therapy. The protocol for this study was approved by the medical ethics committee of Aichi-Gakuin University (No. 17) and informed written consent was obtained from all patients. The laser treatment procedure was explained, and permission to evaluate the specimens was received.
Test group, laser treated.
PD, probing depth; BOP, bleeding on probing.
Thirty-two investigation sites were selected and randomly divided into control (no treatment) and test groups (laser treated). Two clinical periodontal parameters, PD and BOP, were recorded for all sites to establish a relative degree of inflammation. The untreated control group consisted of 18 sites, 4 sites with a PD of ≤3 mm, all being BOP (−); and 14 sites with a PD of ≥4 mm, 9 being BOP (−) and 5 BOP (+). The laser-treated test group consisted of 14 sites, 3 sites with a PD of ≤3 mm, all being BOP (−); and 11 sites with a PD of ≥4 mm, 4 sites being BOP (−) and 7 being BOP (+) (Tables 1 and 2).
PD, probing depth; BOP, bleeding on probing.
Clinical trial
A pulsed Nd:YAG laser (SPL 7200, Sokkia Co., Ltd. Tokyo, Japan) with a wavelength of 1064 nm was used to effect subgingival irradiation in test sites. A quartz silica contact tip of 400 μm diameter (core diameter: 320 μm) was used to deliver laser energy at 2 W of power, 200 mJ/pulse, and 10 pps. The energy beam was delivered in the presence of a surface cooling air spray. The optical fiber was passed through a contra-angled cannula. During pocket irradiation, the fiber was moved along the root surface in a coronal-apical direction for a period of 1–2 min per pocket.
Immediately following laser treatment, both control and test specimens were obtained by incisive dissection using a scalpel. Two vertical incisions and one connecting horizontal incision were placed, creating a rectangular tissue block that included the bottom of the soft tissue pocket wall. The resulting biopsy specimen was carefully removed so not as injure the pocket epithelial surface.
SEM procedure
Upon removal, specimens were gently rinsed in cold saline solution to remove blood and debris loosely adhering to the pocket epithelial surface. Specimens were then fixed by immersion in 2% glutaraldehyde (Kanto Chemical Co., Tokyo, Japan) in phosphate buffered saline (PBS) for 3–4 h at room temperature. Specimens were then post-fixed by immersion in 1% osmium tetroxide (Wako, Osaka, Japan) for 2 h. After being rinsed several times in a phosphate buffer, specimens were dehydrated with a graded series of aqueous ethanol (50%, 70%, 80%, 90%, 95%, and 100%) for 30 min at each concentration, and finally dried with a critical point CO2 drying apparatus (HCP-2, Hitachi, Tokyo, Japan). The pocket epithelial surface of all control and test specimens was sputter-coated with 10 nm of gold using an ion coater (JFC-1500, JEOL Ltd., Tokyo, Japan). Subsequently, specimens were examined by SEM (S2150, Hitachi, Tokyo, Japan) at 15 or 20 kV.
Histologic procedure
After SEM examination, controls and laser-treated test specimens were immersed in distilled water and prepared for routine paraffin embedding. All blocks were facial-lingually sectioned in a step-serial manner at 3 μm by a sledge microtome (Large Sledge Microtome, ERMA, Tokyo, Japan). The sections were stained with hematoxylin and eosin (H&E) and examined using a transmitted light microscopy at magnifications of ×20, ×40, and ×100. The histologic assay was performed by two examiners who were blinded to the control and laser-treated test groups.
Results
SEM observation
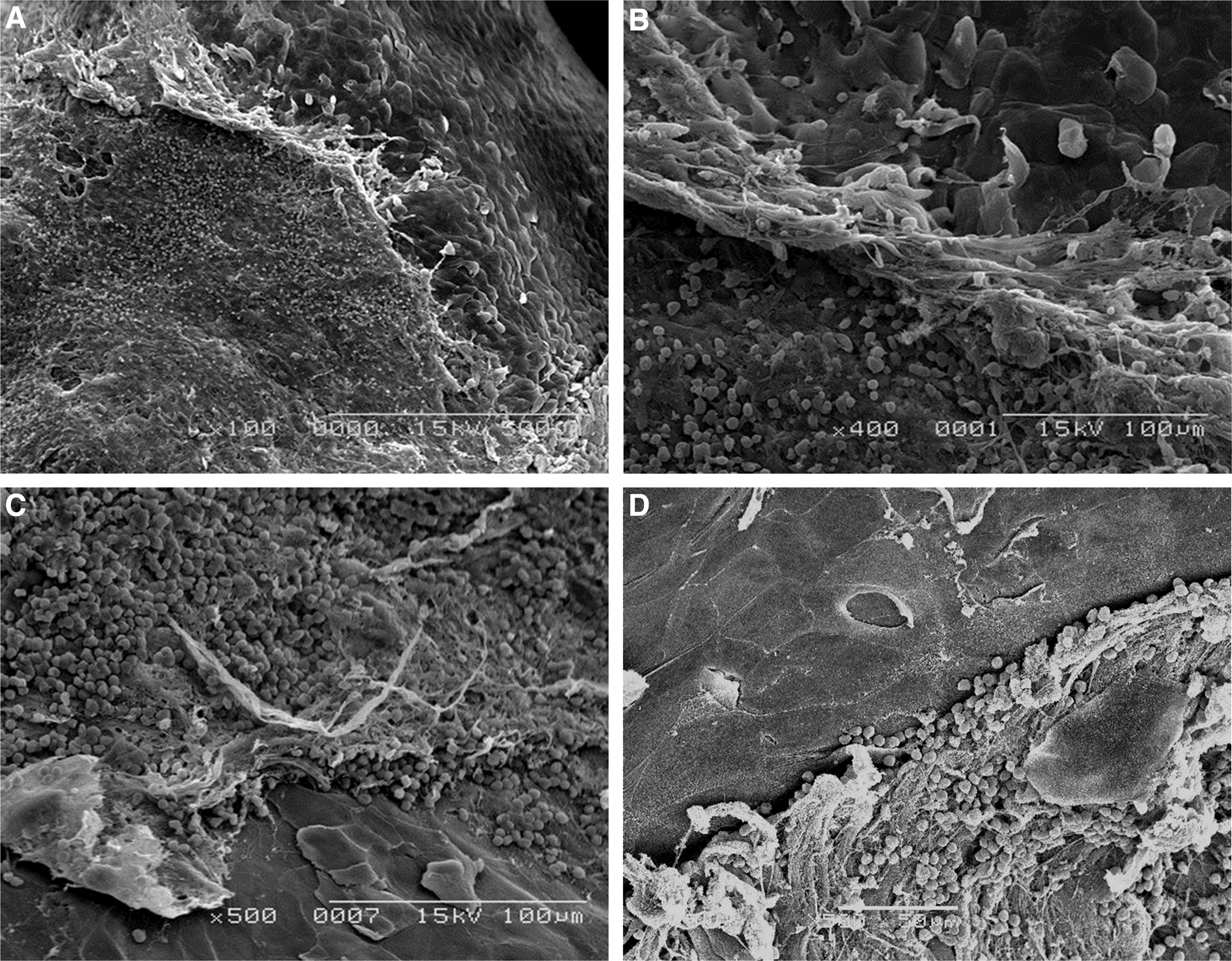
The pocket wall epithelium of untreated control specimens with PD of ≤3 mm and negative BOP exhibited a smooth layer of cells with no apparent loss of integrity or evidence of an inflammatory cell infiltrate (Fig. 1A). In contrast, differing morphologic features of pocket epithelium at different probing depths and relative degrees of inflammation were noted in specimens with PD ≥4 mm (Fig. 1B). At the greatest depth of untreated periodontal pockets, evidence of microbial penetration of the epithelial barrier was observed to occur, following intercellular spaces (Fig. 1C and D). This latter observation was particularly true of specimens that were BOP (+).

Scanning electron microscopic (SEM) images of untreated control group.
Examination of laser-treated test specimens revealed varying degrees of epithelial cell ablation and/or removal of pocket epithelia. In specimens with a PD of ≤3 mm and BOP (−), two cellular changes were noted; for example, either no obvious alterations or disruptions of the epithelial barrier or a localized area of heat-damaged and/or ablated cells (Fig. 2). On the other hand, specimens with PD of ≥4 mm exhibited a conspicuous ablation and/or removal of epithelia. Moreover, these specimens, especially with BOP (+), had a response that featured an erythrocytic and lymphocytic infiltrate covering laser-treated areas (Fig. 3). In some specimens with a PD of ≥4 mm, a peeling and accumulation of epithelium at the interface between laser-exposed and adjacent unexposed surfaces was observed. In all laser-treated test specimens, there was a complete absence of microorganisms.

Scanning electron microscopic (SEM) images of laser-treated test specimens with a probing depth (PD) ≤3 mm and no bleeding on probing (BOP-) showed narrow range and thin layer of evaporated epithelia (marked by arrow) (original magnification: ×500).
Scanning electron microscopic (SEM) images of laser treated test specimens with a probing depth (PD) ≥4 mm showed a conspicuous ablation and/or removal of epithelia. Note the erythrocyte and lymphocyte infiltration covered on laser-treated area (original magnification:
Histologic observation
The epithelium of untreated control specimens at the gingival crest of a periodontal pocket showed intact and thickened, with prominent rete pegs. The thin, nonkeratinized stratified squamous epithelium was observed at a large depth of pocket epithelium. Leukocytic infiltration was usually present near the base of the pocket (Fig. 4).
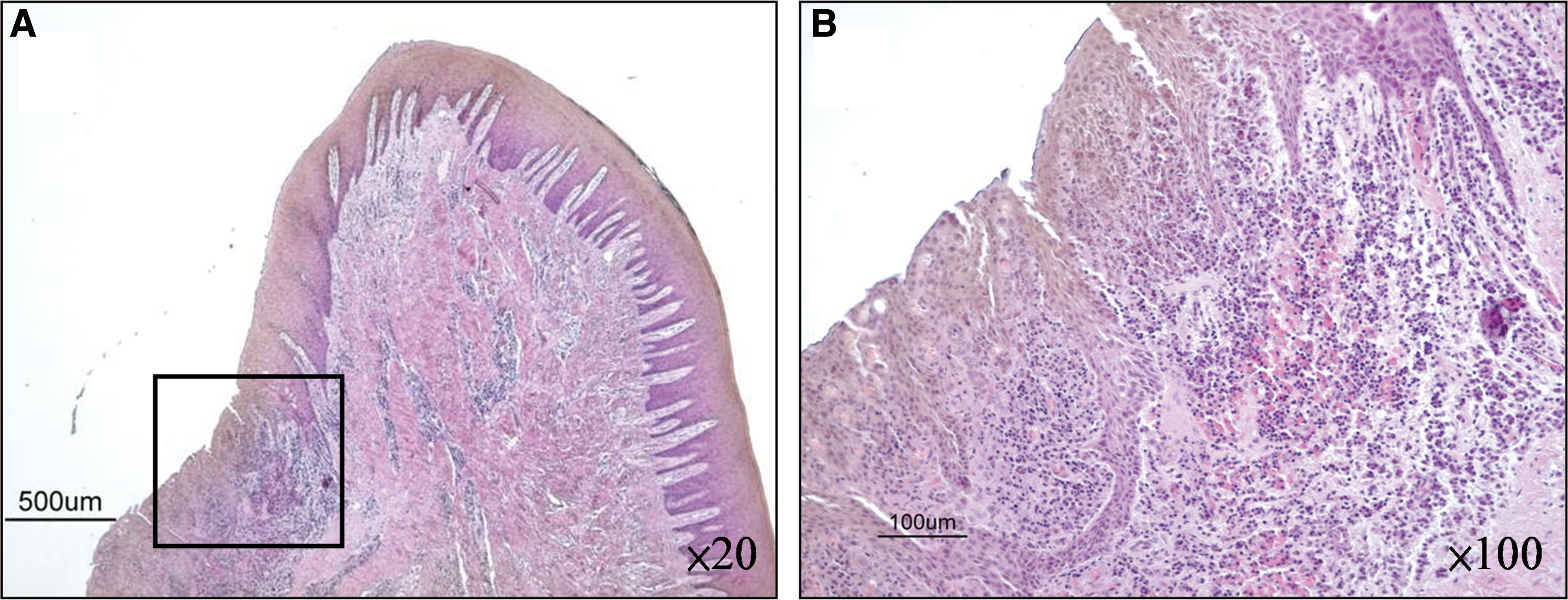
Histologic images of untreated control group.
In laser-treated test specimens, varying degrees of epithelial cell ablation and/or removal of pocket epithelia were observed. No prominence alterations or only thin layers of evaporated epithelia were observed in specimens with a PD of ≤3 mm and BOP (−) (Fig. 5). In contract, the specimens with PD of ≥4 mm exhibited a conspicuous ablation and/or complete removal of epithelia in inflamed portion, whereas epithelium remains were observed in the uninflamed portion. No significant damage on the connective tissues was observed (Fig. 6).
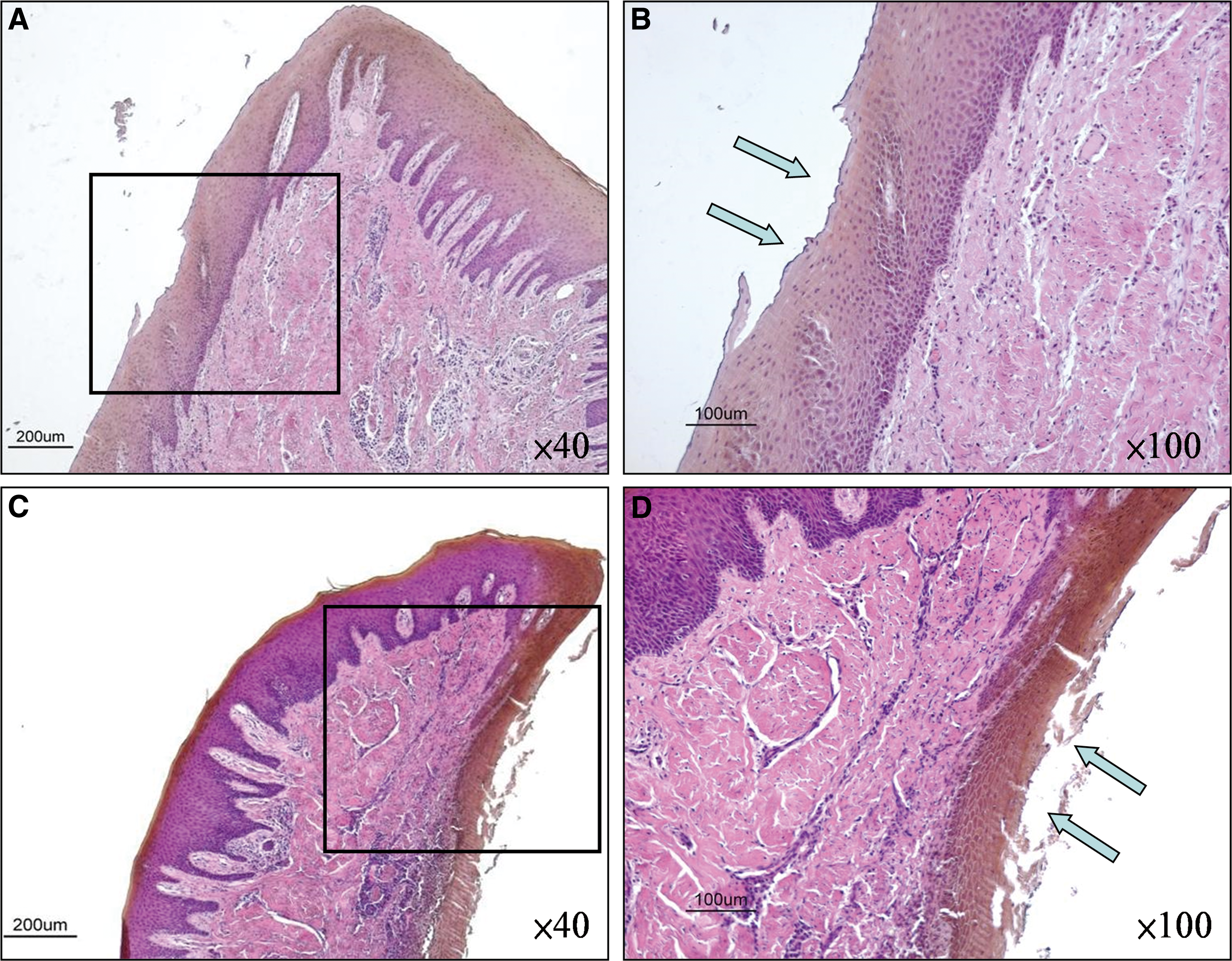
Histologic images of laser-treated test specimens with a probing depth (PD) ≤3 mm and mp bleeding on probing (BOP-). No prominence alterations or only thin layer of evaporated epithelia (marked by arrow) were observed.
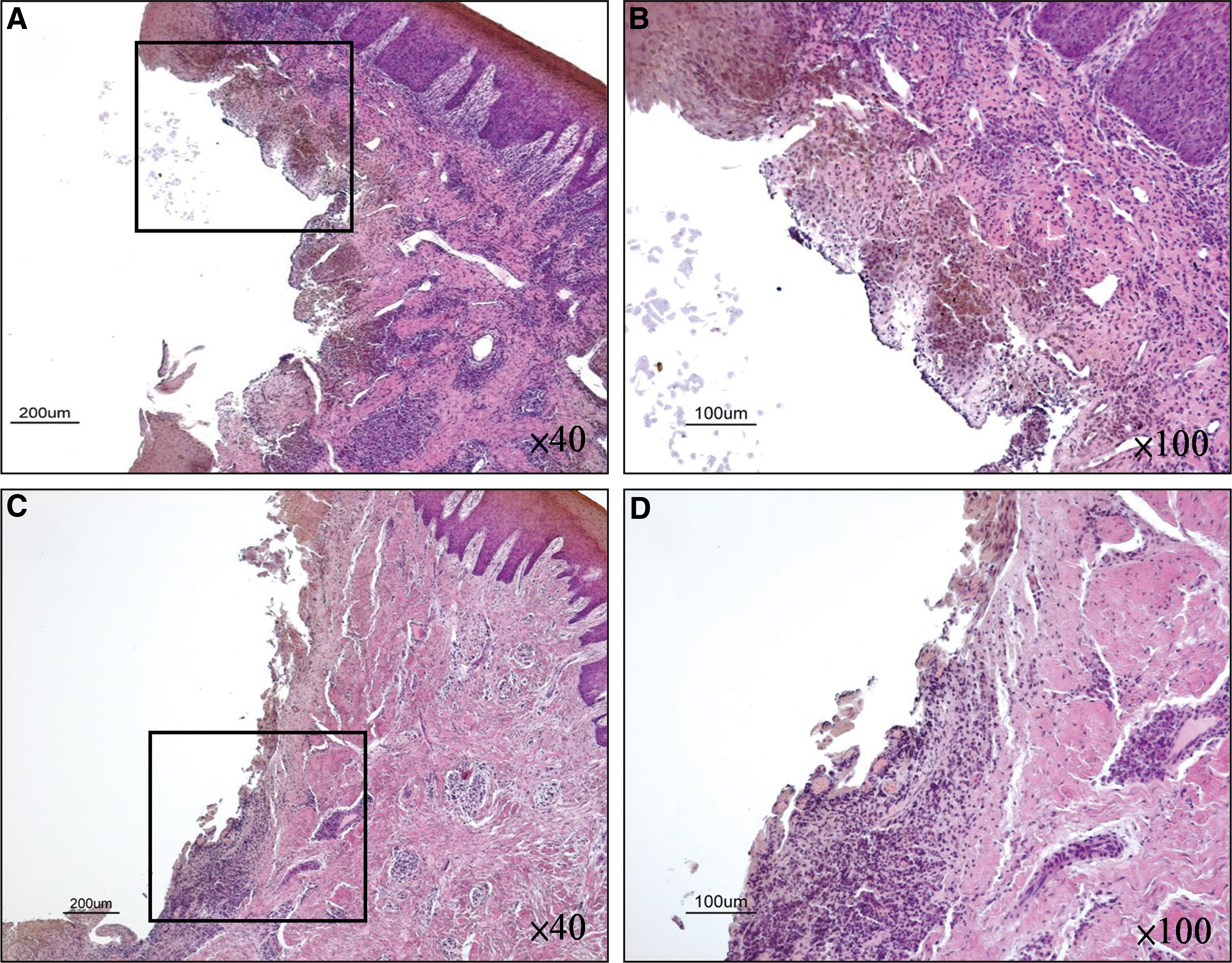
Histologic images of laser-treated test specimens with a probing depth (PD) ≥4 mm. A conspicuous ablation and/or complete removal of epithelia in inflamed portion were observed. Note that the epithelia still remained in the uninflamed portion. (
Discussion
The morphologic features observed using SEM in untreated control specimens in the present study were similar to those reported in previous studies. 26 –28,33 Collectively, these investigations reported surface changes involving pocket epithelium that appeared associated with the presence of subgingival biofilm, but were independent of the clinical presentation of inflammation. In this study, control specimens exhibited a healthy epithelial morphology at shallow PD, and the thin, nonkeratinized stratified squamous epithelium were observed at deep PD. These findings corresponded with earlier studies that examined the healthy crevicular epithelia of monkeys 26 and pocket epithelium from human periodontitis subjects. 33
The laser-treated test specimens with a PD of ≤3 mm and BOP (−) showed no significant alteration or only a thin layer of evaporation. The specimens with a PD of ≥4 mm showed extensive evaporation and complete removal of pocket epithelia in the inflamed portion, whereas epithelium remains were observed in the uninflamed portion. Gold et al. 31 demonstrated a different degree of removal of pocket epithelia (83.3% complete removal and 16.6% partial removal) by examining the morphologic alterations of pocket epithelium histologically following use of a pulsed Nd:YAG laser (1.25 and 1.75 W). We considered that these findings indicated that the structure of healthy, uninflamed pocket epithelia seemed fairly resistant under 2 W (200 mJ, 10 pps) energy output of Nd:YAG laser irradiation without obvious alteration. Consequently, Nd:YAG laser irradiation in the periodontal pocket might easily evaporate and remove the inflamed, weak epithelial tissues.
In the periodontal pocket, the root surfaces and pocket epithelia are contaminated with an accumulation of plaque and calculus, as well as by infiltration of bacteria and endotoxins into the cementum. 34 Complete removal of these harmful substances is essential for the healing of periodontal tissue. Like subgingival curettage to remove pocket epithelium, another technique, ENAP, was first described in 1976, 35 and showed results in “a long, thin epithelial attachment and a minimal amount of connective tissue attachment.” 36 The previous animal study 37 reported that pocket epithelia proliferating apically along the root surface interfered with the establishment of a new connective tissue attachment. They suggested that removal of the inflamed epithelial lining of the periodontal pocket was necessary to obtain new attachment. Additionally, the previous human histologic report 22 that used a specific patented technique of the laser-assisted new attachment procedure (LANAP) with the free-running pulsed Nd:YAG laser, has demonstrated favorable histologic healing. Although the protocol of laser irradiation in this study that used laser curettage is different from ENAP or LANAP, completely removed inflamed epithelium could be observed in the inflamed portion of laser-treated specimens. Short-term and long-term studies 38,39 have revealed that Nd:YAG laser as an adjunct to scaling and root planing could significant reduce the severity of periodontal inflammation. Although they did not provide an absolute explanation for the improvement of periodontal status, we considered that the removal of inflamed pocket epithelium might be an important contributing factor.
In this present study, we observed that the Nd:YAG laser irradiation into the periodontal pocket with 2 W energy output evaporated and removed the inflamed pocket epithelium at large PDs without damage to healthy, uninflamed pocket epithelium. In the histologic findings of this study, additionally, the complete removal of pocket epithelium in the inflamed portion of laser treated specimens was observed. However, different ranges of completely removed epithelium were observed in different parts of specimens. The widest range of removed epithelium was observed in the parts where laser irradiation was performed directly, and the range became narrow far from this part. In clinical performance for completely removed inflamed pocket epithelium, the laser tip of Nd:YAG laser should carefully reach every part of a deep pocket during clinical treatment.
Bacteremia is well known to be associated with scaling as well as with various invasive dental procedures. 7,40 –47 When the tip of the ultrasonic scaler is inserted between the tooth and gingiva, the junctional epithelium and periodontal ligaments are ruptured; bacteria in the sulcus may enter the bloodstream, causing transient bacteremia. Prophylactic management is now indicated for patients who are at risk before such dental procedures. Although antibiotics remain the most accepted prophylactic regimen, they have drawbacks, such as increased bacterial resistance, hypersensitivity, and interactions with other drugs. 48,49
In the laser-treated test specimens of this study, the bacteria aggregation at the lased surface could not be observed either on the laser-evaporated areas or on the unaffected areas. The bacteria attached to the pocket epithelium or invaded into connective tissue should also be evaporated or removed with inflamed pocket epithelia by laser irradiation. Although more randomized blinded controlled longitudinal clinical trials or case-controlled studies are necessary to support the effect of subgingival laser irradiation on bacteremia, several articles 15,50,51 have reported reductions in putative periodontal pathogenic microbes following Nd:YAG laser treatment in vivo.
Conclusions
Given the limited number of treated sites and resulting specimens, the study demonstrated the feasibility of ablating pocket epithelium with an Nd:YAG laser using parameters of 2 W of power, 200 mJ of power per pulse, and a pulse repetition rate of 10 pps via SEM and histologic examination. It was also noted that the presence or absence of clinical inflammation appeared to have an impact on the degree of laser- mediated epithelial ablation. Further clinical studies are necessary to better define the effect of Nd:YAG laser irradiation on the soft tissue wall of periodontal pockets.
Footnotes
Acknowledgments
This work was supported by Strategic Research Aichi-Gakuin University (AGU)–Platform Formation (2008–2012) from The Ministry of Education, Science, Sport and Culture of Japan.
Author Disclosure Statement
No competing financial interests exist.