
Abstract
Introduction
E
Hidden (or occult) caries is a term used to describe a carious lesion seen in dentine through a bitewing radiograph in an area of the tooth in which the occlusal enamel appears healthy or slightly demineralized when clinically evaluated. 3 Although these lesions tend to be minimal in size in the enamel, they spread along the dentinoenamel junction as larger, more invasive lesions within the dentin. 4
However, detection of caries lesions on the approximal surfaces of the posterior teeth is difficult, because direct visual examination cannot be applied because of the wide contact area. 2,5 Approximal lesions are usually detected with a visual tactile inspection combined with radiography. 6 Visual inspection is noninvasive and highly specific, but has low sensitivity and reproducibility. 2,7 –9 Another method is separating the teeth temporarily with elastomeric separators, which allows for direct inspection of proximal sites. 10,11 This method is nondestructive, reversible, and inexpensive, and it may be a useful aid in the diagnosis and management of some lesions. However, occasional discomfort provoked by the placement of the rubber rings and the need for two appointments are disadvantages of the method. 12,13 Radiographic examination is commonly used to detect caries, and is a more sensitive diagnostic method than clinical inspection for detecting approximal lesions in dentine. 14 Although radiography usually detects noncavitated approximal lesions earlier than visual inspection alone, 15 the patient is exposed to a relatively high dose of ionizing radiation. 16 Alternative methods for detecting approximal caries are expected to overcome the disadvantages of these conventional methods.
A pen-type laser-fluorescence (LFpen) device (DIAGNOdent pen; KaVo, Biberach, Germany) has been developed to detect occlusal and approximal caries. 17 LF devices are based on the capture, analysis, and quantification of fluorescence emitted from bacterial porphyrins and other chromophores when the tooth surface is illuminated by a diode laser at a 655 nm wavelength. The LFpen has shown good accuracy and reproducibility in detecting approximal caries, and it has shown promising results in vitro on permanent 18 and primary teeth 19 and in vivo on permanent 20 and primary teeth. 2
Recently, an LED-based device was developed [Midwest Caries I.D. (MID); Dentsply Professional, York, PA] to detect occlusal and approximal caries. In the LED device, the reflectance and refraction of the LED off the surface are captured by fiberoptics and converted into an electrical signal for analysis. According to the manufacturer, when demineralization zones are displayed, the emitted green light changes to red, and a signal is audible. 21
Several studies have reported that the LFpen device shows that calculus, plaque, dental materials, toothpastes, prophylaxis pastes, staining, or hypomineralized noncarious teeth could give false-positive readings. 22 –27 Researchers also demonstrated that LF readings from the approximal surface are affected by the adjacent surface. 28 However, no reports on the effects of the adjacent surface on LED readings have been published. The manufacturer does not recommend the use of this device on restorations, sealants, and varnish, on or at the interface of dental restorations, and for residual caries detection. However, there are no restrictions concerning the use of this device for caries detection on approximal surface contacting restored teeth.
The aim of this in vitro study was to investigate how different dental materials in adjacent teeth influence the LFpen and LED device readings of the tooth being examined. The null hypothesis was that the condition of the adjacent surfaces did not affect the LFpen and LED device readings.
Materials and Methods
The study was approved by the local Committee for Ethics in Research (03-2009/78). Eighty-seven permanent molars with 156 approximal surfaces varying from sound, to having different levels of noncavitated caries lesions, were evaluated in this study. The teeth had no cavitations, approximal restorations, or hypoplastic pits, as judged by the naked eye. After the teeth were extracted, they were frozen at −20°C and stored in individual closed containers until use. The teeth had no contact with the soaked roll, which provided 100% humidity. The stored teeth were later defrosted at room temperature (∼24 ± 1°C) for 4 h before the experiment started. 19 The teeth were then cleaned for 15 sec with a toothbrush under running tap water, and then for 15 sec with PROPHYflex (KaVo, Biberach, Germany) and sodium bicarbonate.
To simulate different approximal conditions of neighboring teeth, four molars were selected from the pool of extracted teeth and then prepared and restored through approximal amalgam restoration (Cavex Amalgam; Cavex Holland BV, Haarlem, Netherlands) approximal composite restoration (Filtek Z550; 3M ESPE Dental Products, St. Paul, MN), full ceramic (IPS e.max® Press; Ivoclar Vivadent, Schaan, Liechtenstein), and zirconia (Katana zirconia; Noritake Dental Supply Co. Ltd., Miyoshi, Japan). Restorations were intact and did not contain any gaps or extensions. The teeth were placed in arch models and fixed with melted utility wax. The best contact points possible were achieved, and the presence was confirmed using dental floss.
The evaluations were performed on the mesial and/or distal surfaces of the molars. All examinations were conducted by one trained examiner. One hundred and fifty-six surfaces were measured with the LFpen and LED devices in contact with the sound surface. The LFpen and LED values from the teeth that were in contact with the sound surface were used as the control values.
The LFpen device attached to probe tip 1 (for approximal surfaces) was utilized according to the manufacturer's instructions. Before each measurement, the device was calibrated against a ceramic reference (standard calibration), and the teeth were air dried for 3 sec with a 3-in-1 syringe before the examination using the LFpen. The detection side of the LFpen device tip was introduced underneath the contact area and moved until the peak value was reached. One measurement on the facial space and one measurement on the lingual interproximal space were taken, and the highest value from both measurements was recorded. The cutoff values for the LFpen readings were as follows: D0, 0–9; D1,9.1–15; and D2, >15. 18
The same measurements were obtained with the LED-based device after calibration with the ceramic standard. Red LED radiation was transported to the occlusal or approximal area using the tip of the probe in contact with the occlusal surfaces. The teeth were then scored as follows. The emission of red light (with an audible tone) indicated the presence of decay or decalcification of the tooth structure, and the emission of green light without an audible tone indicated that the test site was sound. Three types of audible tones that accompanied the emission of the red light clarified the extent of the decay. The cutoff limits suggested by the manufacturer were used to assess the performance of the device: 0 (no signal/green light, sound); 1 (slow or medium signal/red light, caries in the enamel); and 2 (rapid or continuous signal/red light, caries in the dentin).
After the assessments, the teeth were longitudinally cut to the suspected mesiodistal caries sites using an Isomet (Buehler, Lake Bluff, IL) for histological validation, which is the gold standard. Once calibrated, a blinded examiner evaluated the teeth slices using a stereomicroscope at a magnification of ×15 under reflected light. The extent of the caries in the teeth was assessed using Braga et al.'s 8 criteria, modified for histological evaluation as follows: caries free (0), caries in the enamel (1), and caries in the dentin (2) (Fig 1). The depth of the enamel demineralization was assessed in the area that showed the greatest opacity along the direction of the rods. The depth of the dentin demineralization was measured in the area where the color changed from brownish/yellowish to gray along a line at a right angle to the enamel–dentin junction toward the pulp. 29
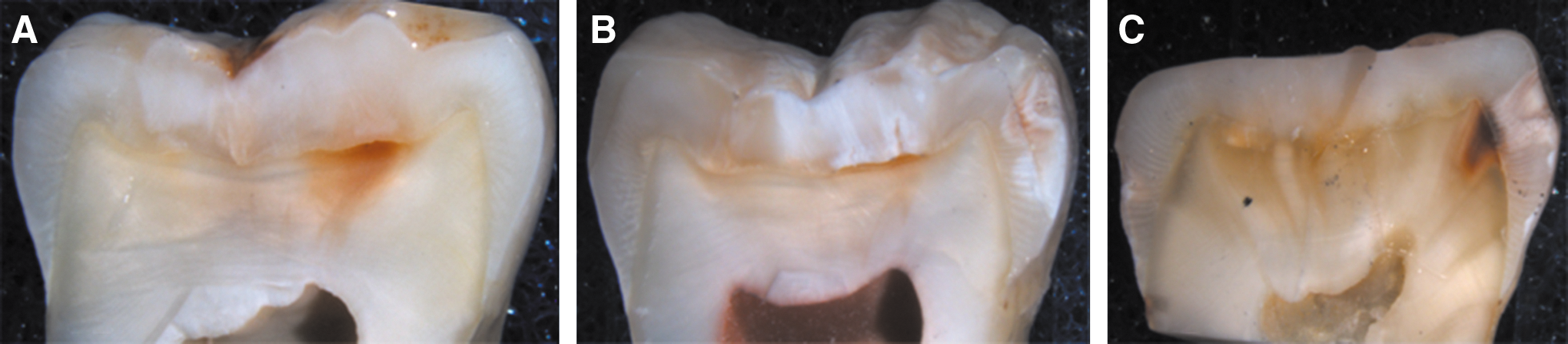
Histological examination.
Statistical analysis
The sensitivity, specificity, accuracy, and area under the receiver operating characteristic (ROC) curve in detecting approximal caries adjacent to four different dental restorative materials using two methods (LFpen, LED-based device) were calculated according to appropriate cutoff scores. For the assessment of validity, values of sensitivity, specificity, accuracy and the area under the ROC curve (Az) at the T1 (sound and enamel caries) and T2 (dentin caries) thresholds were compared by means of a McNemar test. A p value of < 0.05 was considered statistically significant. Spearman's rank correlation was used to evaluate the correlation between the two methods (LFpen, LED-based device) and histological examination. The analyses were performed using the SPSS statistics program for Windows, version 11.5.
Results
The specificity, sensitivity, accuracy, and areas under the ROC curves (Az values) for all conditions in this study are shown in Table 1.
Within columns, significant differences are represented by different superscript letters (McNemar test, p = 0.05 for specificity, sensitivity, and accuracy; nonparametric statistical test for Az).
ROC, receiver operating characteristics; LED, light-emitting diode; LF, laser fluorescence.
The histological examination revealed that 57 of the 156 approximal surfaces were caries free (score 0), 44 had caries in the enamel (score 1), and 55 had caries in the dentin (score 2). The distribution and number of teeth according to the diagnostic methods and the caries classification for the four different adjacent materials are shown in Table 2.
LED, light-emitting diode; LF, laser fluorescence.
For the LFpen device, the specificity was higher when the adjacent tooth had a full ceramic (80.70) or zirconia restoration (77.19), but this is not significant when compared with the specificity achieved with adjacent amalgam restorations at the T1 threshold. The specificity was higher when the adjacent tooth had a full ceramic restoration (90.10), and this is significant when compared with the specificity achieved with an adjacent sound surface and zirconia for the T2 threshold. Higher sensitivity at the T1 threshold was found when the adjacent surface was smooth (92.93). At the T2 threshold, sensitivity was highest when teeth were contacting sound tooth surfaces (74.55) and composite restorations (72.73), but this is not significant compared with the sensitivity achieved with adjacent zirconia restorations. The accuracy of the LF-based device was higher when the adjacent surface was sound (80.76) at the T1 threshold, and no significant differences were found at the T2 threshold.
ROC curves (Az values) at the T1 and T2 thresholds were 0.68–0.76 and 0.70–0.78, respectively. The area under the ROC curves demonstrated that there were no significant differences between LF-based device performance when the adjacent surface had a restoration, and LF-based device performance when the adjacent surface was sound at the T1 and the T2 thresholds.
For the LED-based device, the specificity was higher when the adjacent tooth had a composite restoration (78.95), and this is significant compared with the specificity achieved when the adjacent tooth had a full ceramic restoration or a sound surface at the T1 threshold. At the T2 threshold, specificity was higher when the adjacent tooth had a zirconia restoration (87.88). No significant differences were found between sensitivities at the T1 threshold. The sensitivity was higher when the adjacent tooth had a composite (70.91) or amalgam restoration, (76.36); however, this was not significant compared with the sensitivity achieved when the adjacent tooth had a full ceramic or zirconia restoration at the T2 threshold. There were no significant differences found between accuracy values at the T2 threshold.
The areas under the ROC curve at the T1 and T2 thresholds were 0.68–0.80 and 0.68–0.74, respectively. The area under the ROC curves showed that LED-based devices performed better when the adjacent surface was a composite restoration at the T1 threshold, and there were no significant differences at the T2 threshold.
The highest correlation coefficient between histological examination and the LFpen was found when the teeth were in contact with a sound surface. The highest correlation coefficient between histological examination and the LED device was found when the teeth were in contact with a composite restoration (Table 3).
LF, laser fluorescence; LED, light-emitting diode.
Discussion
The present study investigated the influence of different dental materials on LFpen- and LED-based device readings adjacent to the tooth being measured. The null hypothesis that the condition of the adjacent surface does not affect LFpen and LED device readings must be rejected. The specificity and sensitivity changed when the adjacent teeth had restorations.
Virajsilp et al. 30 compared LF reading values when teeth were and were not in contact with another smooth tooth surface, and found a high correlation. However, there are no data in the literature on the effect of contacting teeth on LED readings. Generally, diagnosing approximal caries is more difficult when adjacent teeth are present. Therefore, to reflect actual clinical practice, LFpen and LED values for teeth that were in contact with a smooth surface were used as the control values.
The first LF-based caries detection device was introduced to clinicians and designed for occlusal surfaces. The tips of this device were unable to penetrate far enough into the approximal space or deflect the light laterally. The LFpen is designed for occlusal and approximal surfaces. LFpen has a new optical system for the probe so that the user can access the contact area closely enough to capture fluorescence emerging from a carious approximal surface. The prismatic shape of the probe tip has the advantage of allowing access to the approximal contact and allowing the ability to direct the excitation light laterally to the long axis of the tip. The approximal probe is designed with a prism that deflects the laser beam 100 degrees, making it possible to access the approximal surfaces. 17,18 Several in vitro and in vivo studies related to the performance of LF-based devices have been reported in the literature. The results have shown that the LFpen is accurate and reproducible in detecting caries on permanent 5,18,20 and primary teeth. 2,19,31
In the present study, specificity values of the LFpen device tended to increase compared with sound surface, but this increase was significant only when an adjacent surface had a zirconia or full ceramic restoration at the T1 threshold and a ceramic restoration at the T2 threshold. The sensitivity of the LFpen decreased when the adjacent surface had a restoration at the T1 threshold, and no significant change was found when the adjacent surface was sound at the T2 threshold.
When the teeth were in contact with zirconia and full ceramic restorations, the true-negative LF readings increased, but the true-positive readings decreased in all conditions compared with sound surface for sound approximal surface and enamel caries (T1 threshold). When teeth were in contact with full ceramic, the true-negative LF readings increased for dentin caries. When teeth were in contact with amalgam and full ceramic, the true-positive readings decreased for dentin caries.
Lussi et al. 28 evaluated the effect of the adjacent tooth surface condition on LF readings, and used teeth with composite, ceramic, and ZnO-eugenol restorations to simulate neighboring teeth. An adjacent surface with a ZnO-eugenol restoration increased the LF readings from sound surface, enamel, and dentin caries, but this increase was not significant for dentin caries. A composite restoration increased LF readings, but this increase was significant only for the smooth surface. When the adjacent teeth had a ceramic restoration, the LF values increased, but this was not significant. Additionally, ceramic restorations decreased the LF readings for surfaces with enamel and dentin caries. In the present study, the T1 threshold included smooth surfaces and enamel caries. However, in the Lussi et al. 28 study, smooth and carious tooth surfaces were evaluated separately. The difference in the results of the two studies may be for this reason.
The LED-based device was developed to detect occlusal and approximal caries. In contrast to the LFpen, the LED device manufacturer claims that detection for both occlusal and approximal lesions can be performed occlusally. One probe detects interproximal and occlusal caries while providing clinical access and enhanced visibility, and the visual and audible caries detection signals provide an ideal end-user interface. For occlusal lesions, this device gave contradictory results. The specificity and sensitivity were 0.56–0.94 and 0.31–0.88, respectively, at the enamel threshold and 0.48–0.90 and 0.70–0.84, respectively, at the dentin threshold. 21,32,33 The differences in specificity and sensitivity values may result from differences between the cutoff values and thresholds. For approximal caries, the specificity and sensitivity were 0.87 and 0.32, respectively, at the enamel threshold and 0.89 and 0.39, respectively, at the dentine threshold. 6
In the present study, at the T1 threshold, the specificity of the LED device tended to increase in all conditions, but this increase was significant only for composite restorations. At the T2 thresholds, the specificity of the LED device significantly increased only in the teeth that had contact with zirconia. There were no significant differences between the sensitivity achieved when the tooth being examined was in contact with various restoration materials and that achieved when it was in contact with a sound surface at the T1 and T2 thresholds. When the teeth had contact with composite, the true-negative readings for the LED device increased on smooth surfaces and enamel caries. When the teeth were in contact with zirconia, the true-negative readings increased on the dentin caries.
Virajsilp et al. 30 reported that LF devices generally showed lower sensitivity but higher specificity when the tooth had contact with adjacent teeth. They explained that most extrinsic stains or intrinsic stains at the lesion remained, and that these stains might produce a fluorescent signal that increased LF values. However, contact with teeth could prevent false-positive readings from the stain and, therefore, increase the specificity. At the same time, the neighboring teeth also prevented true-positive readings for the carious lesions, which led to decreased sensitivity. In the present study, all teeth restored with different materials showed a similar effect to that of the unrestored neighboring teeth, and thus increased specificity and decreased sensitivity. The differences in the decrease and increase in the LFpen and LED values may be the result of the different optical properties of the dental materials.
One of the most important requirements for the ideal diagnostic method for caries detection is good intra- and interexaminer agreement about the method. It must be noted that only one examiner performed one assessment to evaluate the performance of devices. This may be considered one of the limitations of the current study.
Conclusions
Within the limitations of this study, the following conclusions can be drawn: 1. Although LFpen readings may be influenced by the adjacent restored surfaces for approximal enamel caries detection, LED readings may not be influenced by the adjacent surfaces. 2. When LFpen is used to detect approximal caries on teeth that are in contact with amalgam and full ceramic restorations, some dentin caries may not be diagnosed. 3. When adjacent tooth was restored with ceramic materials, LFpen readings for evaluating sound surfaces yielded more accurate results than other materials for both thresholds. 4. For evaluating sound surfaces with LED-based devices, adjacent composite restorations at T1 and for zirnconium at T2 yielded more accurate results than other materials.
Therefore, both devices could be used effectively for evaluating approximal surfaces with adjacent restored teeth, regardless of the different kinds of restorative materials.
Footnotes
Author Disclosure Statement
No competing financial interests exist.