
Abstract
Introduction
T
An alternative approach to chemotherapeutics consists in the use of medical lasers. Various lasers are used in periodontics: Er:YAG laser is used to target bone, dental hard tissues, and calculus, whereas CO2, Nd:YAG and diode lasers are prevailingly used for soft tissue surgery because of their superior ability to induce tissue ablation/vaporization, hemostasis, and sterilization. 7,8 In particular, Nd:YAG and diode lasers have been used in photoablative mode (i.e., with high energy output) for subgingival curettage and periodontal pocket decontamination, although with uneven results. 9 Recently, photodynamic soft laser therapy also entered into use in periodontics. By this technique, low energy lasers at appropriate wavelengths activate photoactive substances, such as methylene blue, to generate oxygen free radicals with potent bactericidal properties. 10,11
On these grounds, we have recently reported that a dual diode laser treatment, termed “photoablative-photodynamic” (PAPD), adjunctive to SRP, can improve the clinical outcome of patients with chronic periodontitis at a 1-year follow-up. 12 The key feature of the PAPD protocol consists in the combination of two different laser modalities in order to exploit their characteristics and achieve synergistic effects. In particular, intra/extra pocket epithelial photoablation with diode laser (λ 810 nm, 1 W) was used to remove the gingival epithelium, the main reservoir of periodontal pathogens, 4,5 whereas photodynamic treatment with a different diode laser (λ 635 nm, 100 mW, and 0.3% methylene blue), performed after SRP and repeated weekly until needed, was used to extend the periodontal antiseptic and antitoxin treatment in the deep root alveolar sites where conventional SRP 13 and photoablation are ineffective.
The aim of the present study was to report the results of PAPD plus SRP versus sham treatment plus SRP alone extended to 4-year follow-up, to evaluate whether PAPD plus SRP can achieve durable amelioration and/or healing, and consolidate the value of this new therapeutic approach to chronic periodontitis.
Materials and Methods
Subjects
Twenty-six patients (Caucasian, 14 males and 12 females, age range 25–65, mean 46.1) affected by chronic periodontitis, as defined by Armitage, 14 were selected from January 2009 to April 2010. The patients were informed about the nature, timing, and potential risks and benefits of their participation in the trial and then signed a written informed consent. Of them, 24 (13 males and 11 females, ages 25–65) completed the study, whereas 2 patients discontinued the treatment and were lost to the follow-up. The clinical protocol complied with the Declaration of Helsinki, as amended in Edinburgh 2008, and the Consolidated Standards of Reporting Trials (CONSORT) statement (Fig. 1). The study was approved by the Medical Ethics Committee of the Florence University, Italy (SPE 14.126-ASF). Inclusion and exclusion criteria are reported in Table 1.
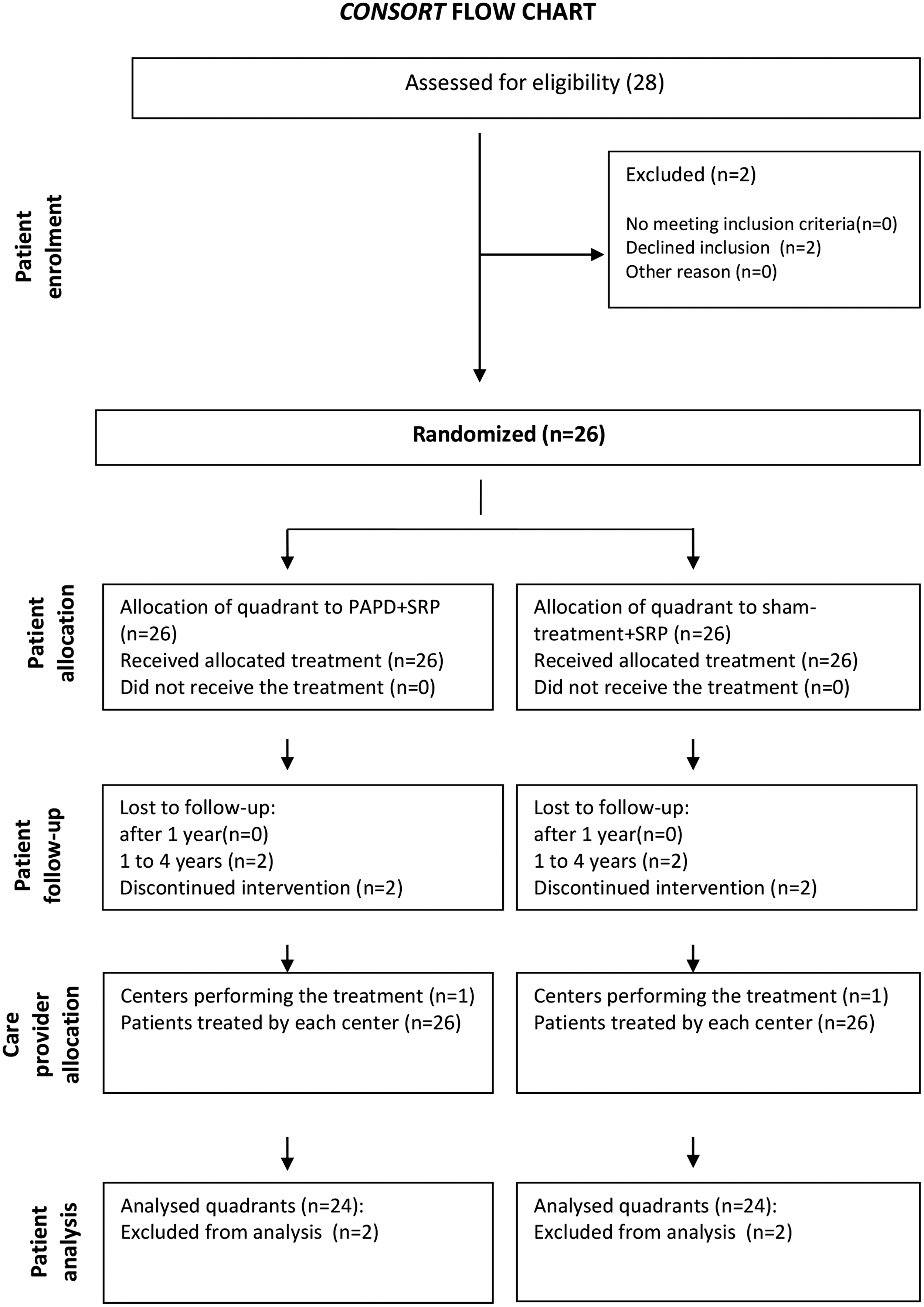
Consolidated Standards of Reporting Trials (CONSORT) flow chart of the clinical study.
Periodontal treatment randomization and allocation
Each patient underwent two parallel treatments (split-mouth): the teeth on the test maxillary quadrant received PAPD plus SRP, whereas those of the contralateral control quadrant received sham treatment plus SRP, consisting of the same manual operations and methylene blue applications performed with a switched-off laser. Allocation concealment of the patients' upper quadrants to PAPD plus SRP or sham treatment plus SRP was performed by sequentially numbered opaque sealed envelopes (SNOSE), opened and registered by a non-clinical investigator (L.F.) immediately before the beginning of the treatment, and kept concealed from the clinical operator in charge of follow-up analyses until completion of the study.
Examiner/operator features and blinding
Periodontal clinical assessment at admission was performed by a periodontologist (L.L.) who was not involved in the patients' subsequent treatment and data analysis. Eight periodontopathic subjects not included in the study were preliminarily recruited and used as standard reference by the examiner. The examiner recorded full-mouth probing depth (PD) and recessions at six sites per tooth (with the exclusion of the third molars), using a conventional manual periodontal probe (PCP15, Hu-Friedy, Chicago, IL). The examiner was deemed reliable when repeated measures (twice after an interval of 1 h) were in a range of ±2 mm. This procedure was repeated periodically during the 4-year study period. This investigator also collected follow-up data at 1 and 4 years in a blinded fashion, being unaware of the treatments applied. The operator who performed the treatments (M.G.) was not involved in any evaluation before or after his intervention. Except for the periodontal pocket chart needed for the treatment, he was unaware of the previously recorded data.
Treatment phase I: Oral hygiene
After admission, all patients were seen by a dental hygienist for: (1) supragingival scaling by ultrasonic and/or hand instrumentation and tooth polishing with dental paste (Nutro Dentsply, Philadelphia, PA) applied with a rotary rubber cup and (2) instruction and motivation to maintain oral hygiene.
Periodontal clinical assessment
One week after the oral hygiene treatment, the subjects were recalled to collect baseline clinical data. The blinded examiner (L.L.) evaluated PD, clinical attachment level (CAL) and bleeding-on-probing (BOP). CAL was PD plus recession (assumed as 0 whenever the cement–enamel junction was covered). BOP was assessed during PD assay as presence or absence of bleeding; then, BOP scoring was calculated for each quadrant as the percentage of sites (six per tooth) showing bleeding within 30 sec. after probing. The PD measurements were also used to calculate the percentages of shallow (<4 mm), moderate (4–6 mm) or deep (>6 mm) periodontal pockets at the different treatments and time points. The test and control quadrants comprised teeth 1–8 and 9–16 without furcation involvement. The test time points were 0 (baseline, before any therapy), 1, and 4 years. Windent software (QuadernoElettronico Ltd., Montevarchi, Italy) was used for measurement collection.
Periodontal cytodiagnostic assessment
Samples containing cells shed from gingival epithelium, blood cells, and bacteria were taken with a sterile microcurette at the free gingival margin of the teeth to be treated at day 0 (before therapy), and 1 and 4 years after therapy. They were smeared on glass coverslips, fixed in 90% ethanol, stained with the fluorescent dye LIVE/DEAD BacLight™ (Invitrogen/Molecular Probes, Milan, Italy), and observed under a fluorescent microscope (Leica 4000 B Microsystems, Milan, Italy). This cytofluorescent method, extensively described elsewhere, 12,15 allows the detection of the amount and viability of bacteria (cocci, bacilli, and spirochetes), erythrocytes (RBC), damaged epithelial cells (DEC), and inflammatory polymorphonuclear leukocytes (PMN), and represents a sensitive method to assess the severity and progression of periodontal disease. 12,15,16 These parameters were semiquantitatively scored by a specifically trained dental assistant on a 0–3 scale (0, normal; 3, severe changes) according to Giannelli et al. 12,15
Treatment phase II: Photoablative laser treatment and SRP
Each patient underwent two parallel treatments: the teeth on the test maxillary quadrant were subjected to PAPD plus SRP, and those of the contralateral control quadrant were subjected to sham treatment plus SRP. The gingival mucosa underwent photoablation with a λ 810 nm diode laser (4×4 Dental Laser System, General Project Ltd., Montespertoli, Florence, Italy) set as reported in Table 2. This laser was used because of its low tissue penetration, allowing complete removal of the contaminated gingival epithelium with minimal injury to the lamina propria. 17 Irradiation was performed in contact mode (the fiber tip touching the gingiva) to remove the junctional, sulcular, and outer gingival epithelium (∼5 mm from the gingival margin) all around the teeth, under airflow cooling. Irradiation was performed under thermographic feedback, which activated an alarm if tissue temperature approached the damage threshold, and stopped laser emission if the temperature exceeded 80°C. Laser treatment was usually painless. Local anesthesia was given on demand to a single patient during laser photoablation, and to 15 patients during SRP on the control quadrants. At the end of the laser or sham treatments, conventional SRP was performed using Gracey curettes (Hu-Friedy) until the root surfaces were clean and smooth.
Treatment phase III: Photodynamic laser treatment
At the next clinical sessions, 1 week after the previous treatments, the photoablated mucosa was subjected to photodynamic treatment. The periodontal tissues, including the pocket, the surrounding mucosa, and the dental root, were rinsed with methylene blue (0.3% w/v in water). After 5 min, the treated areas were irradiated with a λ 635 nm diode laser set as reported in Table 2. The absorption curve of methylene blue in water ranges from λ 609 to 668 nm, and peaks at λ 665 nm. In a biological environment, binding of methylene blue to bacteria and their byproducts, such as lipopolysaccharide, shifts its absorption spectrum to lower wavelengths, 18 thereby approaching the λ 636 nm emission of the used diode laser. The optical fiber was gently introduced into the pocket and moved circularly in a deep-to-cervical direction, or smoothly a few millimeters over the outer gingiva (average time per tooth: 1 min inside and 1 min outside the pocket). This procedure did not require any local anesthesia. The photodynamic treatment was repeated once weekly until normalization of the cytodiagnostic parameters, especially PMN (range: 4–10 applications). Sham treatment consisted of methylene blue rinsing with no laser photoactivation. The whole photoablative and photodynamic laser treatment protocol is referred to as “PAPD therapy.” The affected teeth of the lower mandibular quadrants were also treated, but not evaluated for this study.
Post-treatment supportive periodontal therapy
After the phase III treatment, the patients were seen by a dental hygienist every 3 months during the 1st year and then every 6 months until the end of the study for professional mechanical plaque removal, reinforcement of oral hygiene instruction, and motivation. The treatment included: (1) supragingival plaque removal and tooth polishing, and (2) subgingival plaque removal using ultrasonic and/or hand instrumentation aimed at minimal debridement into the gingival sulcus. No mouthwashes or toothpastes containing triclosan, chlorhexidine, or other antimicrobial agents were prescribed.
Statistical analysis
The subject's quadrant was assumed as test unit for statistical comparison. For the clinical parameters, each test unit resulted from the average of six measurements per tooth, and a minimum of five teeth per quadrant. For the cytodiagnostic parameters, each test unit was the average of five sampling sites per quadrant for a total of 360 exfoliative samples. The clinical and cytodiagnostic parameters taken at baseline, 1 year, and 4 years after the treatments were first checked for normal distribution with D'Agostino–Pearson omnibus normality test. The clinical values, which were normally distributed, were compared by within-subject, repeated-measures ANOVA and Newman–Keuls multiple comparison test, whereas the cytodiagnostic values, not normally distributed, were compared by Kruskal–Wallis test followed by Dunn's multiple comparison test. A p value≤0.05 was considered significant. The aim of statistical comparison was to detect whether significant differences exist in the outcome variables for periodontal disease assessment, in terms of clinical parameters (primary outcome) and cytodiagnostic parameters to evaluate antimicrobial/anti-inflammatory effects (secondary outcome), between PAPD plus SRP and sham treatment plus SRP after a 4-year follow-up.
Results
Of the 26 patients enrolled, 24 successfully completed the study. The remaining two subjects left the study because of exacerbation of periodontitis in the control quadrant, requiring the shift to SRP plus PAPD treatment. A total of 138 teeth per experimental group was evaluated and compared. The values of the clinical parameters (PD, CAL, BOP) assayed before the treatments and at 1- and 4-year follow-up are reported in Tables 3 and 4. As previously reported, 12 at 1-year follow-up, both sham treatment plus SRP and PAPD plus SRP improved the clinical parameters in comparison with the pretreatment levels, with greater improvement with PAPD plus SRP. At the 4-year follow-up, the control quadrants subjected to sham treatment plus SRP showed a slight to moderate worsening of the clinical parameters at the 1-year follow-up. Conversely, PAPD plus SRP therapy caused a further, statistically significant reduction of PD and CAL, and maintained the striking improvement of BOP already observed at the 1-year follow-up. Accordingly, PAPD plus SRP therapy significantly and time dependently increased the percentage of shallow pockets, while reducing that of moderate and deep pockets compared with SRP alone (Table 4). Moreover, after 4 years, PAPD plus SRP therapy induced the disappearance of clinical signs of gingival inflammation accompanied by tight epithelial reattachment of the free gingiva to the dental root, with reduction or disappearance of gingival pockets in most of the patients examined (Fig. 2). It is of note that the patients perceived very little or no pain and discomfort during PAPD laser treatment, requiring no local anesthesia, and did not undergo adverse events during the 4-year follow-up. The patients showed a mean full-mouth plaque index of 0.90±0.20 at baseline that was reduced to 0.85±0.17 after 1 year and to 0.81±0.25 after 4 years (p<0.05).
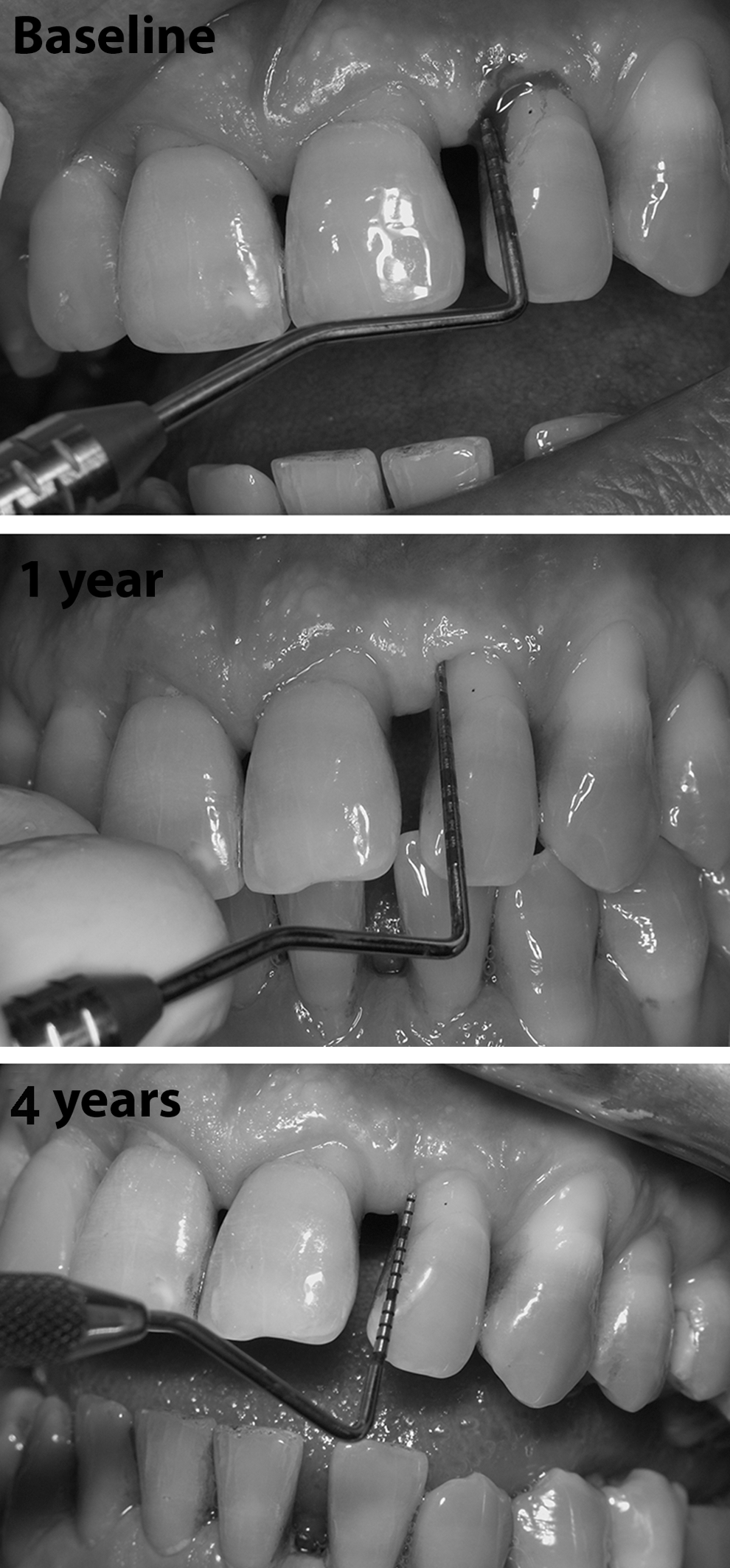
Representative images of a typical periodontopathic patient taken at admission (upper panel) and at 1- and 4-year follow-up (center and lower panels). The patient's left quadrant has been subjected to photoablative and photodynamic therapy (PAPD) plus scaling and root planing (SRP). Before the treatment, the probe reveals a deep pocket associated with bleeding-on-probing. At the 1-year follow-up, tight epithelial root reattachment impedes the probing. No signs of bleeding or inflammation of the periodontal tissues can be seen. A similar condition can be seen at the 4-year follow-up.
SEM, standard error of the mean; PD, pocket probing depth; SPR, scaling and root planing; PAPD, photoablative-photodynamic therapy; CAL, clinical attachment level; BOP, bleeding on probing.
SEM, standard error of the mean; PD, pocket probing depth; SPR, scaling and root planing; PAPD, photoablative-photodynamic therapy.
In parallel with the classical clinical parameters, we used a cytodiagnostic assay to achieve a semiquantitative evaluation of periodontal inflammation, bleeding, and bacterial contamination. The results are shown in Table 5. In comparison with the control quadrants, PAPD plus SRP therapy was more efficient in reducing the amount of PMN, an index of periodontal inflammation, at the 1- and 4-year follow-up, yielding a stable, statistically significant reduction (fewer than five PMN per microscopic field) or normalization (no PMN per microscopic field) of this parameter. Conversely, in the sham treatment plus SRP quadrants, PMN tended to progressively re-grow at both follow-up time points. In two patients, exacerbation of periodontal inflammation in the sham treatment plus SRP quadrants required them to be shifted to PAPD plus SRP therapy, and therefore they exited the study. Evaluation of RBC, a microbleeding index, indicated that PAPD plus SRP therapy induced a greater reduction of this parameter at the 1- and 4-year follow-up compared with the sham treatment plus SRP quadrants. A similar trend, albeit less evident and only reaching statistical significance at the 4-year follow-up, was observed by the measurement of DEC, an index of gingival epithelial injury. Evaluation of microbial contamination showed that PAPD plus SRP therapy induced a significant reduction of the bacterial species most commonly associated with periodontitis; namely, spirochetes and bacilli, at the 1- and 4-year follow-up compared with the sham treatment plus SRP quadrants. In particular, spirochetes, which include the most aggressive periodontopathogens, 19,20 tended to persist in the sham treatment plus SRP quadrants at both time points, whereas they remained undetectable in the PAPD plus SRP group (p<0.001). Cocci, which encompass both pathogenic species and the normal oral microbial flora, showed no substantial changes in the sham laser treatment plus SRP quadrants, whereas they were reduced by PAPD plus SRP at the 4-year follow-up.
SEM, standard error of the mean; PMN, polymorpholuclear leukocytes; SRP, scaling and root planing; PAPD, photoablative-photodynamic therapy; RBC, red blood cells; DEC, damaged epithelial cells.
Discussion
The present 4-year follow-up study on 24 patients with chronic periodontitis treated with SRP and diode laser in sequential photoablative-photodynamic modes (PAPD therapy) confirms the efficacy of this innovative therapeutic approach over conventional SRP and offers evidence for its capability to achieve durable clinical improvement and healing potential. In the long term, as compared with the quadrants undergoing sham treatment plus SRP, those subjected to PAPD plus SRP showed a significant, stable improvement of PD, CAL, and BOP, thus meeting the primary outcome objective. The clinical findings were paralleled by the cytodiagnostic data, which also met the secondary outcome objectives. In the PAPD plus SRP-treated quadrants, the patients consistently showed the absence of the most aggressive periodontal bacteria, such as spirochetes, 19,20 and a marked abatement of the amount of PMN and RBC, which are related to the severity of periodontal inflammation and bleeding. 12,15,16,21 Because infiltrating leukocytes can produce harmful substances, such as reactive oxygen species, inflammatory mediators, and matrix-degrading enzymes, capable of back-feeding the inflammatory process and promoting progressive reabsorption of alveolar bone and soft tissues, their removal is crucial for periodontal healing and repair. 22,23 The finding that PAPD plus SRP therapy results in long-lasting decontamination of the treated quadrants is particularly relevant, as it predisposes to periodontal healing. Periodontopathogenic bacteria can evade host immunity and conventional antibiotics by penetrating and persisting into epithelial cells of the periodontal pockets and outer gingiva. 4,5 This bacterial reservoir can account for re-colonization of periodontal tissues after conventional treatments, disease relapses, and chronicization. 6,24 Laser-aided de-epithelization can thus remove most periodontopathogens, whereas repeated photodynamic therapy cycles hamper periodontal reinfection. It is of note that in most patients, the quadrants subjected to PAPD plus SRP therapy did not undergo disease relapses, despite that the sham treatment plus SRP control quadrants still showed various degrees of bacterial contamination and residual periodontitis. SRP itself has been reported to favor bacterial invasion of the connective tissue underneath the sulcular/junctional epithelium. 23 In our study, bacterial re-colonization of the test quadrants is likely prevented by the tight adhesion of the free gingiva to the dental root often observed with PAPD plus SRP therapy.
Another remarkable effect of the PAPD plus SRP treatment consisted of long-term stabilization of gingival tissues, as judged by the marked improvement of CAL at the 4-year follow-up. This phenomenon may depend on the absence of appreciable fibrotic retraction and scarring of the gingiva. We have previously shown that photoablation with the 810 nm diode laser causes a nearly selective removal of the gingival epithelium without substantial thermal injury to the lamina propria. 17 This is an important point considering that, in mammals, the regenerative ability of mature organs is limited to superficial epithelial wounds not substantially involving the underlying connective tissue, whereas the stroma is nonregenerative and responds to injury by scarring. 25
The clinical and microbiological responses to conventional SRP in the treatment of chronic periodontitis are well documented. 2 A comprehensive meta-analysis of nonsurgical treatment reported that, following SRP at sites with probing depths ≥4–7 mm, clinicians should expect a mean reduction in PD of ∼1–2 mm, and a gain of CAL of ∼0.5–1 mm. When patients were followed up over ≥3 years, these differences were reduced to <0.4 mm. 26 Adjunctive antibiotic therapy may slightly improve the clinical parameters over SRP alone, but there is general consensus that the use of antibiotics in chronic periodontitis should be restricted to selected cases irresponsive to conventional treatment. 27,28 The current findings of a marked and long-lasting improvement of the clinical and microbiological parameters after PAPD laser therapy combined with conventional SRP allow this protocol to be regarded as a valuable resource for the treatment of chronic periodontitis. Moreover, most of our patients felt no pain or discomfort during PAPD treatment, which could be performed without local anesthesia, and had an overall preference for the laser modality, in keeping with recent reports. 29 This indicates that the PAPD plus SRP protocol is safe and well tolerated.
Conclusions
In the current clinical literature, the efficacy of lasers in the treatment of chronic periodontitis in adjunct to SRP is matter of debate. 8,9 Limited evidence supports the view that diode lasers in photoablative 30,31 or photodynamic mode 32,33 can yield appreciable advantages over SRP alone. On these grounds, with the PAPD therapy, we have combined the photoablative and photodynamic laser treatment modalities to take advantage of their different functional mechanisms. Photoablation can achieve selective and harmless sterilization of the bacterial intraepithelial reservoir, whereas photodynamic activation of methylene blue can achieve effective antiseptic and antitoxin action useful to shift the parasite–host balance in favor of the latter, thereby counteracting disease relapses and facilitating periodontal healing. Further studies are needed to compare the efficacy of PAPD therapy with other laser-aided protocols adjunctive to SRP, as well as to elucidate whether photoablative and photodynamic laser treatments have additive or synergistic effects.
Footnotes
Acknowledgments
The authors gratefully acknowledge Tiziana Fossi for skillful technical help in oral hygiene and cytodiagnostic assay.
Author Disclosure Statement
No competing financial interests exist.