
Abstract
Introduction
D
They frequently lead to infection and amputation in the lower extremity due to the absence of circulation in the limb, which causes critical ischemia in the lower extremity. 6 DM is the most common cause of amputation in the lower extremity in the United States and European countries. 7 According to the statistical reports, the annual rate of amputations is ∼82 people per 10,000 in diabetics patients. 8 DM with foot ulcers requires amputation in 14–20% of cases; furthermore, foot ulcer is the precursor of more than 85% amputation in lower extremity. 9,10 Subsequently, chronic DFUs present a clinical challenge for doctors with DM patients. 11
Wound healing generally occurs as the consequence of cellular response to an injury and involves activation of keratinocytes, fibroblasts, endothelial cells, macrophages, and platelets. Numerous growth factors and cytokines released by mentioned cells are needed for coordination and maintaining the healing mechanism in the skin. The biopsies of epidermis by molecular analysis, in which the samples were taken from patients, identified pathogenic markers that correlated with the delayed wound healing process. 12 Subsequently, by the reduction of irregular localized epidermal growth factor receptor (EGFR) and activation of the glucocorticoid pathway, the migration of keratinocytes gets inhibited. It was concluded that keratinocytes presented no existence of migration, proliferation, and deficient differentiation at the edge of nonhealing DFUs (callus). In addition, fibroblasts demonstrated phenotypical changes as well as decrease in migration and proliferation. Although, cells from an adjacent nonulcerated area displayed the appearance of a normal phenotype, they were physiologically nonfunctional. The mentioned cells have the ability to respond to the administration of additional growth factors or cellular therapy. Despite the existence of consistent protocols in standardized care, the physiological impairments can result in DFU complications and delay the healing process. 12,13
It has been postulated that hyperglycemia itself has deleterious effects on wound healing through the formation of advanced glycation end products, which induce production of inflammatory molecules, such as tumor necrosis factor alpha and interleukin-1 (IL-1), and interfere with collagen synthesis. 14 As a result of glycation, impaired biomechanical properties of diabetic skin, 15 impaired proliferation, and migration of dermal fibroblasts occur. 16,17
The application of frequency in low-level laser therapy (LLLT) is growing rapidly. Based on the scientific literature, there are important breakthroughs, which have shown that pulsed wave (PW) LLLT accelerates the healing of human crural 18 and the superficial wounds. 19 According to the previous scientific studies, the positive effect of PWLLLT on healing of open skin wounds and healing burns in healthy and diabetic rats has been reported. The documents demonstrated a significant increase in the number of fibroblasts, blood vessel endothelium, and blood vessel in histological sections and gene expression. 20,21 Furthermore, a significant increase in the rate of wound closure and increase of wound strength have been reported. 22,23
The growth factors and cytokines secreted by mesenchymal stem cells (MSCs; secretomes) could be administered to wounds by either cell transplantation or a safer alternative could be using conditioned medium (CM) from MSCs, which contain the secreted bioactive molecules. 24 MSCs secrete a combination of growth factors and cytokines, which have been shown to accelerate wound healing. This combination of growth factors and cytokines successfully causes angiogenesis, decreases inflammation, and stimulates fibroblast migration and collagen production. 25 To reduce wound closure time, MSC is an ameliorative treatment for chronic wounds. 26 Recently, CM has been applied successfully to treat wounds in nondiabetic and diabetic animals. 25 –27 Ganji et al. divided 24 rats into four groups: normal control, diabetic control, diabetic placebo (culture medium-treated), and diabetic experimental (human bone marrow mesenchymal stem cell-conditioned medium [hBM-MSC-CM]-treated rats). Type I DM was induced in the rats by alloxan. One incision was made on the skin dorsal region of each rat. Twenty-four hours after wounding, diabetic experimental rats received 200 μL of hBM-MSC-CM and diabetic placebo rats received 200 μL of culture medium. Fifteen days after wounding, the wounds were extracted and submitted to tensiometrical testing. 27 Ganji et al. found that maximum force and stress high load of experimental group were significantly higher than those of diabetic control rats, and they concluded that hBM-MSC-CM has significant positive effect on wound strength in diabetic rats. 27
Currently, no solid data have been reported to conclude the effect of combined PWLLLT and hBM-MSC-CM on the healing process of full-thickness skin incisions in streptozotocin (STZ)-induced type I diabetic rats. As suggested by two recent studies, they showed that pulsed infrared laser with 890 nm wavelength, 80 Hz frequency, and 0.2 J/cm2 energy density significantly accelerated the healing process in diabetic rats. 21,23 As a matter of fact, the main objective in this investigation focused on the combined effect of PWLLLT with the wavelength of 890 nm, frequency of 80 Hz, and energy density of 0.2 J/cm2 in addition to the usage of hBM-MSC-CM on the healing process of incisions in type I diabetic rats. The combined use of PWLLLT and BM-MSC-CM could improve severe DFUs in patients.
Materials and Methods
Isolation and expansion of hBM-MSCs
The entire procedure was approved by the Medical Ethics Committee of Shahid Beheshti University of Medical Sciences (Tehran, Iran; Protocol No. 5137). The bone marrow (BM) sample was collected from a 35-year-old healthy female donor from the Cell Bank Center of Royan Institute for Stem Cell Biology and Technology (Tehran, Iran). BM-derived MSCs were isolated and cultured according to the previously reported protocol.
28,29
Briefly, aspirated BM was diluted in phosphate-buffered saline (PBS). The mononuclear cells were isolated by centrifugation in a Ficoll gradient, after which they were washed with PBS and cultured in Dulbecco's modified Eagle's medium (DMEM) supplemented with 15% fetal calf serum, 2 mM
Immunophenotyping of cultured hBM-MSCs by flow cytometry
Passage-4 expanded MSCs were detached by trypsin/EDTA, fixed with 4% paraformaldehyde, and then resuspended in 0.05% PBS-Tween. To detect MSC surface antigens, the samples were incubated in 2% bovine serum albumin blocking solution for 20 min. Afterward, the cells were incubated with fluorescein isothiocyanate (FITC)—or phycoerythrin (PE)—conjugated mouse anti-human antibodies for 45 min at 4°C. The following antibodies were used: anti-CD105-PE (FAB10971p; R&D Systems), anti-CD90-PE (ab95698; Abcam), anti-CD73-PE (BD550257; BD Biosciences), anti-CD45-PE (ab157309), and anti-CD34-FITC (ab18227). Mouse isotype antibodies (IgG1, kappa, ab18443; Abcam) were used as negative controls. The results were analyzed to 104 events against each antibody with a Becton Dickinson flow cytometer and WinMDI software. 28,29
Preparation of hBM-MSC-CM
In this study, CM was prepared by culturing 106 passage-4 hBM-MSCs in a TP75 culture flask. Cells were allowed to grow until a confluence of ∼80% cells was achieved. Eventually, cells were washed twice with PBS. The medium was replaced by a serum-free basal medium and incubated for 48 h. CM was collected and concentrated ∼20-fold by lyophilized drying (Christ Alpha 1-2 LD Plus) according to the manufacturer's instructions; cells were cryopreserved at −20°C up to the use.
Animals and study design
Twenty-eight Wistar male adult rats, 4 months old and weighing ∼260 g, were obtained from Pasteur Institute (Tehran, Iran) and used in this study. Rats were housed individually in standard rat cages in a 12-h light/12-h dark environment and provided with water ad libitum. Type I DM was induced in all rats. For all animals, two full-thickness incisions were made on the skin in their backs, one on the thoracic region (proximal) and the other one on the lumbar region (distal). Rats were randomly divided into four groups, and in each group, seven animals were included. The first group was considered as the control group and received vehicle control medium (DMEM). The second group received hBM-MSC-CM; the third group received PWLLLT; and eventually, the fourth group received hBM-MSC-CM+LASER. The proximal wounds in the third and fourth groups were treated by a pulsed laser with energy densities of 0.2 J/cm2.
Induction of type I DM
Type I DM was induced in all rats by an intraperitoneal injection of STZ (Enzo Life Sciences, Inc.), freshly dissolved in sterile distilled water (pH = 7.3), at a single dose of 50 mg/kg body weight. 20 DM was defined as a blood glucose concentration >250 mg/dL by taking a blood sample from the vein in their tails (GM300; Biomince, GMH), 7 days from STZ injection. 23 All diabetic rats were kept for 30 days for making sure that DM was stable in rats. Two full-thickness incisions were made in their skins 30 days after STZ injection. Animals were sacrificed 45 days after STZ injections for biomechanical examination.
Surgery
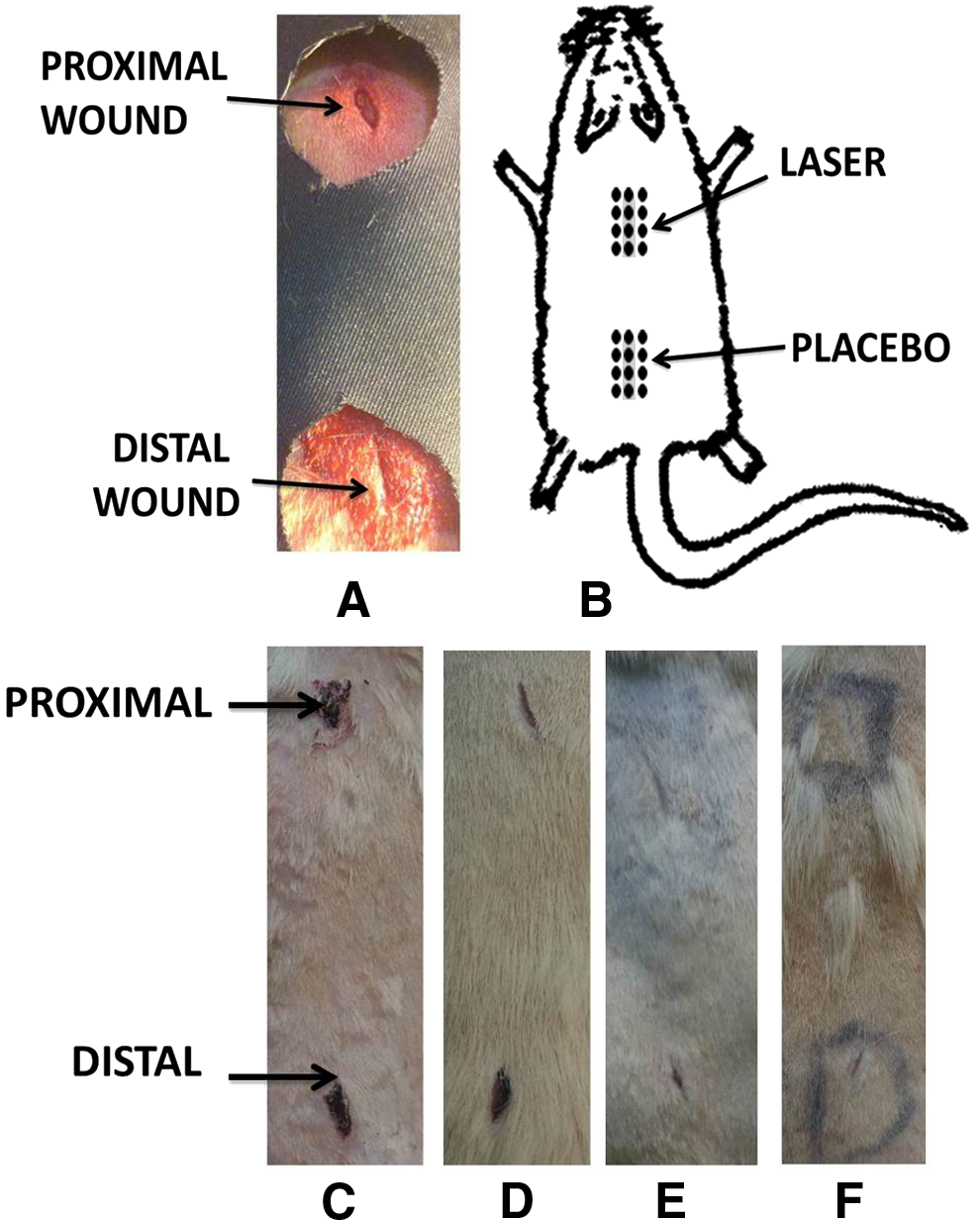
On the 30th day after the injection of STZ in diabetic rats, the animals were anesthetized by ketamine hydrochloride (i.m., 50 mg/kg body weight) intramuscularly (i.m.) along with diazepam (i.m., 5 mg/kg body weight). Subsequently, the fur on the back of rats was shaved and sterilized with alcohol and povidine–iodine. Two longitudinal, full-thickness 12-mm incisions were made on the thoracic and lumbar regions with a No. 15 blade and scalpel, respectively (Fig. 1). The incisions were 4 cm apart.
Pulsed wave low-level laser therapy
The proximal incisions in the third and fourth groups were exposed to a pulsed infrared diode laser [MUSTANG 2000 with LO7 pen (radiating head); Technica Co.] with the following specifications: - Peak power output: 75 W - Average power: 1.08 mW - Power density: 1.08 mW/cm2
- Wavelength: 890 nm - Pulse frequency: 80 Hz - Spot size: 1 cm2
- Pulsed duration: 180 ns - Duration of exposure of each point: 200 s - Energy density: 0.2 J/cm2
The LLLT procedure commenced immediately after the surgery. In the current study, the surface area of the target tissue (including wound in the center and surrounding normal skin, Fig. 1) was larger than the pen's spot size; therefore, we used sequential treatments to ensure that every unit area received similar laser dose. 23 LLLT was performed over 12 distinct regions, which included the wound area and surrounding normal skin, with the laser pen perpendicular to the target tissue, at the distance of <1 cm per region. During laser treatment, irradiated animals were sedated by a half dose of anesthetizing drugs. LLLT was continued once daily, 6 days a week, for the duration of 15 days. The distal wounds in the third and fourth groups were submitted to the pulsed laser with radiating pen without the laser being switched off. This was considered the placebo group. All rats received the same dose of anesthetizing drugs.
Clinical observations
The rats' blood glucose levels and body weights were monitored every 2 weeks throughout the study to determine their hyperglycemic states. The majority of animals developed clinical evidence for DM within a week, following STZ injection. Animals which failed to develop a blood glucose level >250 mg/dL were excluded from the study. The wound site was examined closely every day for monitoring of any apparent exudation. 30 The wounds in rats were observed and photographed on the 15th day (Fig. 1). For our analysis, the complete wound closure in all groups was recorded. 31
Biomechanical examination
Surgery was performed and after 15 days, six rats from each group were randomly selected; rats were sacrificed by injecting an overdose of anesthetized drugs that was followed by cervical dislocation. After careful dissection from underlying deep fascia, standardized rectangular skin specimens (5 × 50 mm strips) were harvested across the wound by using a double-blade cutting instrument. The sample thickness was measured by a digital caliper. During the test, specimens were kept moistened in 0.9% NaCl solution. Specimens were mounted in a material testing machine (Santam, Eng. Design Co., Ltd., Tehran, Iran). Two clamps were used with a rough surface, whereby the wound was placed in the free space. The jaw space, which was the distance between the edges of the clamps, was 30 mm. The deformation rate was kept constant at 10 mm/min. Specimens were loaded uniaxially; therefore, the failure and complete load–deformation curve could be recorded (Fig. 2). From the load–deformation curve, the following biomechanical properties were automatically calculated. Bending stiffness (M·Pa) was calculated by dividing the maximum force by displacement of rupture. The maximum force (N) was measured directly from the load–deformation curve and represented the maximum tensile force applied to rupture the specimen. Stress high load (N/mm2) was calculated at the maximum force divided by the cross-sectional area of the specimen. Energy absorption (J) was the area under the load–deformation curve. 23
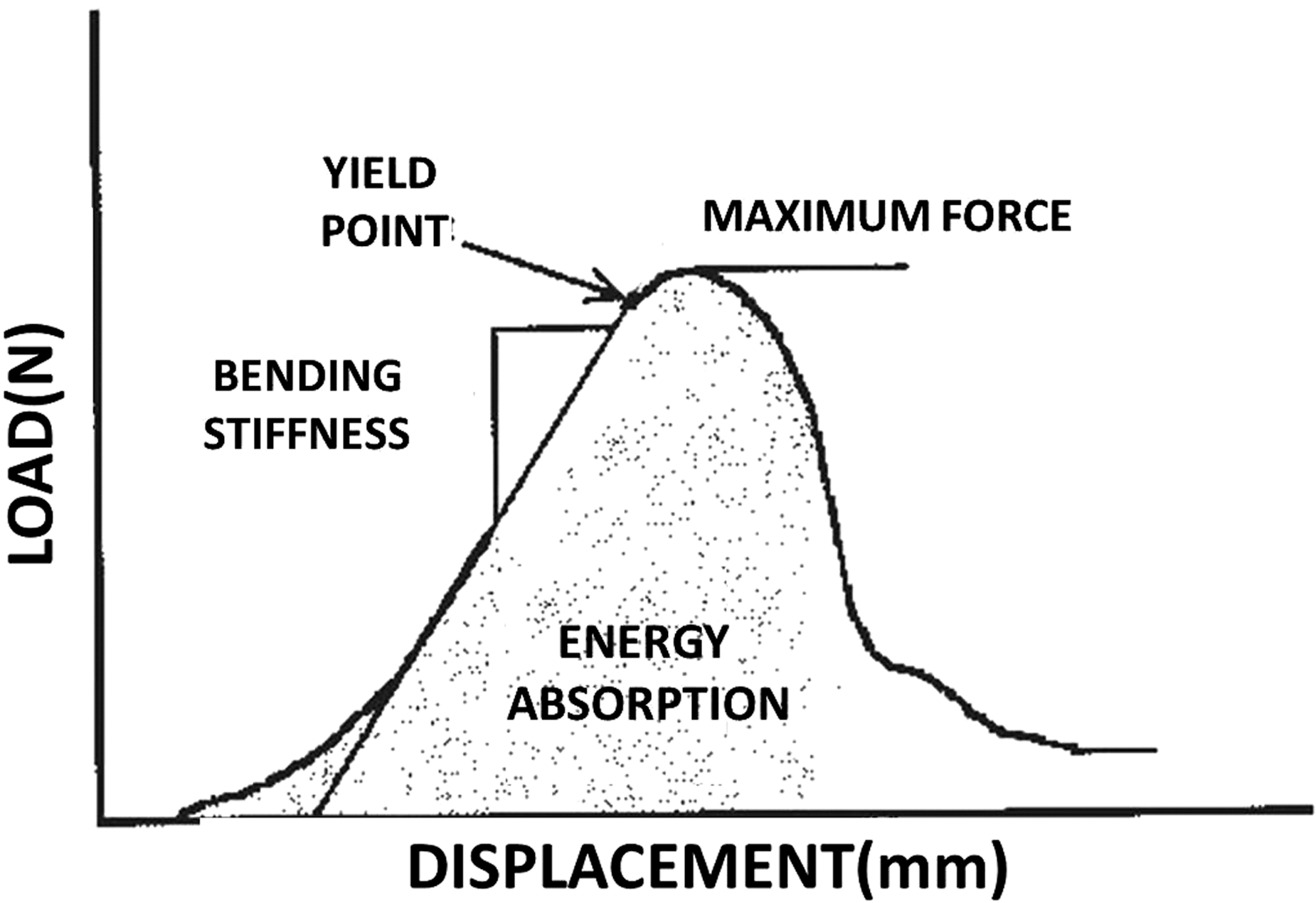
Schematic representation of the load–deformation curve in repairing wound. The graph illustrates various biomechanical characteristics derived from the material testing machine. They are bending stiffness (M·Pa), maximum force (N), and energy absorption (J); proximal (P) and distal (D).
Statistical analysis
All data are expressed as mean ± standard deviation of mean. Normal distribution of data was analyzed by using the Shapiro test. Data from body weights were analyzed by using the Wilcoxon test. The Mann–Whitney test was used to compare changes among biomechanical parameters in the studied groups. In our experimental groups, the closures of all wounds were recorded. The wound closures in proximal and distal parts in the entire population were analyzed by using the chi-square test. A p-value of <0.05 was considered statistically significant.
Results
Mononuclear cells were isolated from hBM aspirate by a ficole. They showed typical features of MSCs such as morphology and immunophenotyping (Fig. 3A).
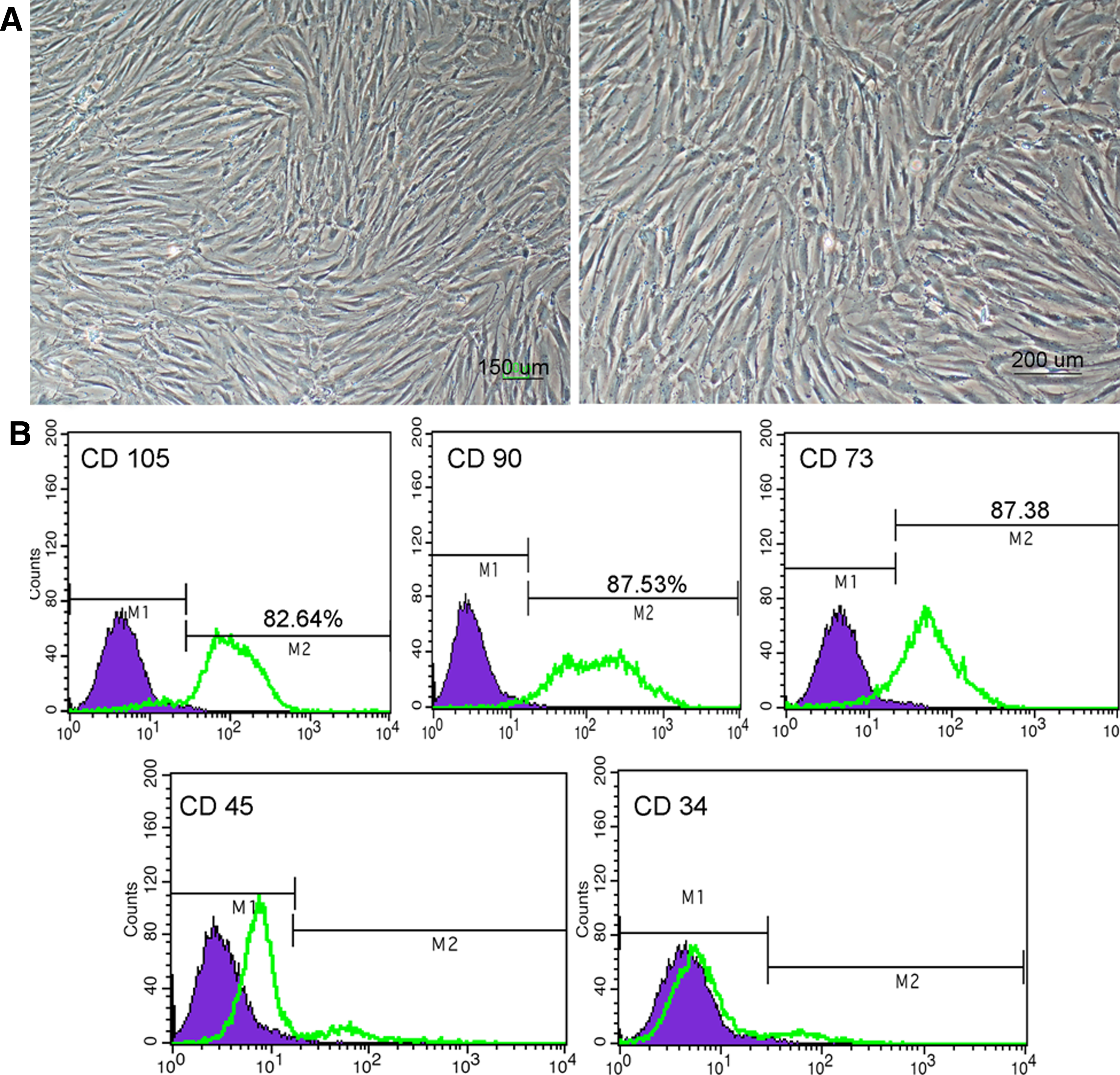
Characterization of cultured hBM-MSCs. Passage-4 MSCs grew as a spindle-shaped, fibroblastic, homogeneous monolayer cell population that had a characteristic nonhematopoietic phenotype
Passage-4 MSCs exhibited fibroblastic appearances with a homogeneous spindle shape (Fig. 3A). According to flow cytometry, the passage-4 cells expressed CD105 (82.64%), CD90 (87.53%), and CD73 (87.38%), but did not express CD34 and CD45 markers (Fig. 3B).
General and clinical observations
There was no evidence of exudate in the wounds during our experiments. All diabetic rats developed clinical evidence of DM a week after STZ injection. The entire population of diabetic rats showed metabolic abnormalities, which characterized with uncontrolled DM; furthermore, a significant decrease in body weight was observed. The statistical analysis was performed by Wilcoxon test, in which the results showed a significant decrease of body weight at the day of surgery compared with the beginning of our experiment (266.3 ± 41.8 vs. 241 ± 30.3 g; p = 0.000). Blood glucose level at the beginning of the experiment was measured and it was 95.7 ± 12.6 mg/dL. Blood glucose level increased significantly to 389.3 ± 86.8 mg/dL at the time of biomechanical testing. Table 1 shows wound closure in the studied groups. There were no significant differences in wound closure between proximal and distal wounds in each group. The number of wound closures was significantly higher in proximal wounds in the laser and LASER+CM groups compared with the control ones (chi-square test, p = 0.002 and p = 0.015, respectively).
There were no significant differences in wound closure between proximal and distal wounds in each group. Chi-square test showed that the number of wound closures was significantly higher in proximal wound in the third (LASER) and fourth groups (LASER+CM) compared with the control ones (p = 0.002 and p = 0.015, respectively).
CM, conditioned medium.
Biomechanical examination
The results of biomechanical examination are shown in Figs. 4 –7.

Mean ± SD of bending stiffness in the study groups, compared by using the Mann–Whitney test. There was a significant difference in bending stiffness between third (LASER), fourth (LASER+CM), and second (CM) groups and the control group (p = 0.004, p = 0.006, and p = 0.032, respectively). There was also a significant difference in bending stiffness between laser-treated rats in second and fourth groups (p = 0.007, p = 0.012, respectively). *<0.05, **<0.01. CM, conditioned medium; SD, standard deviation.
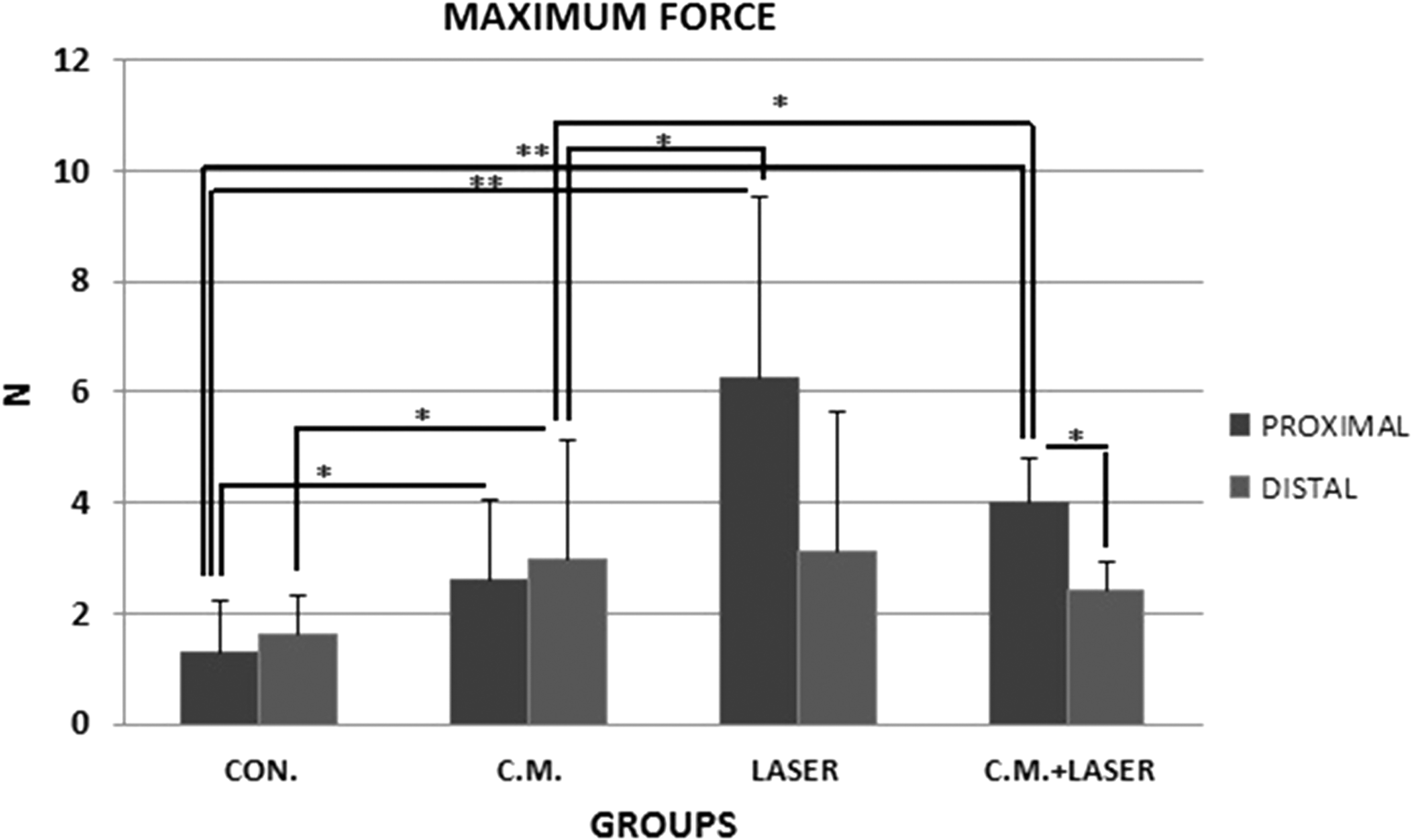
Mean ± SD of maximum force in the study groups compared by using the Mann–Whitney test. There was a significant difference in maximum force between third, fourth, and second groups and the control group (p = 0.004, p = 0.008, and p = 0.044, respectively). There was also a significant difference in maximum force between CM-treated rats in third and fourth groups (p = 0.014, p = 0.042, respectively). *<0.05, **<0.01.
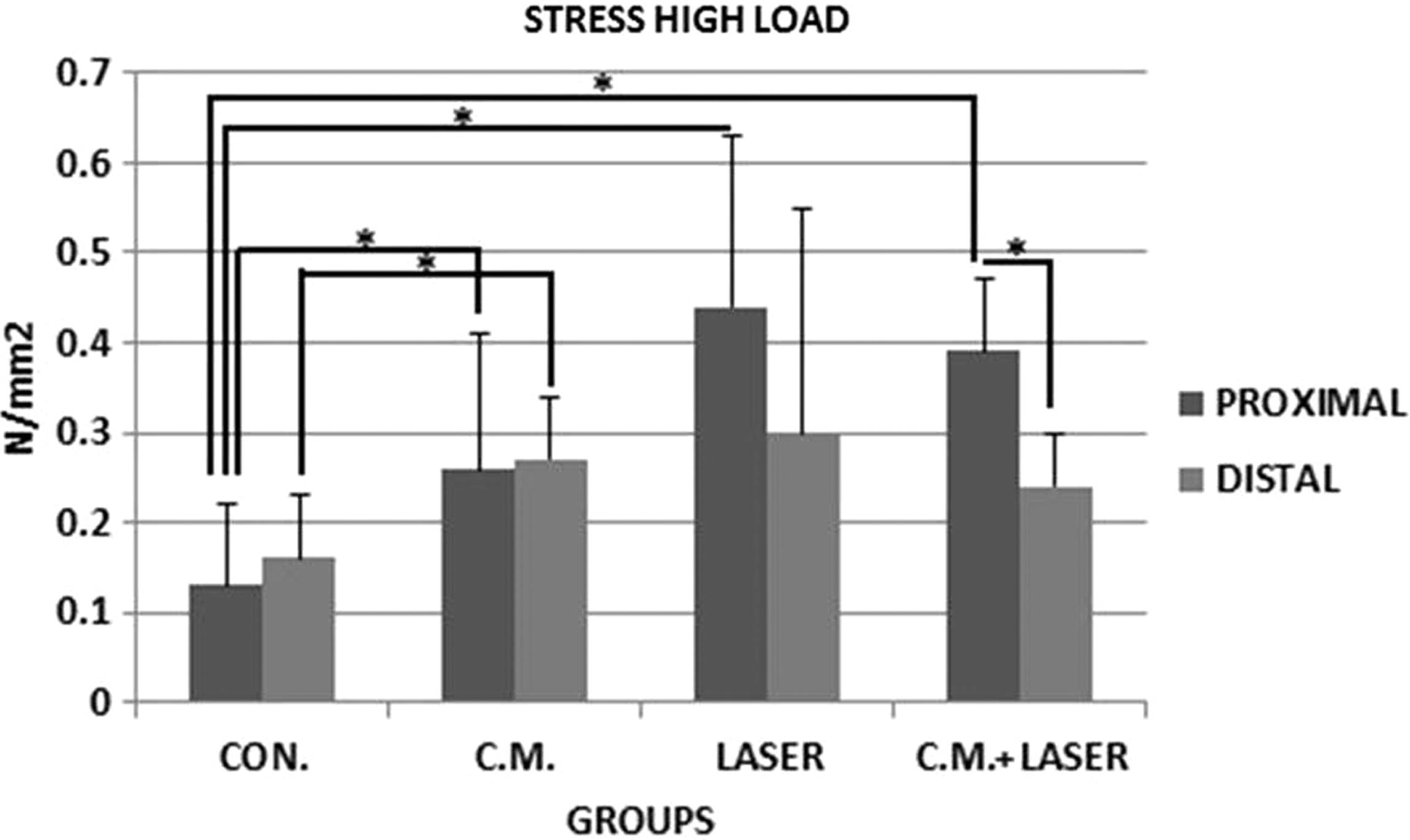
Mean ± SD of stress high load in the study groups was compared by using the Mann–Whitney test. There was a significant difference in stress high load between fourth, third, and second groups and the control group (p = 0.011, p = 0.016, and p = 0.044, respectively). *<0.05, **<0.01.
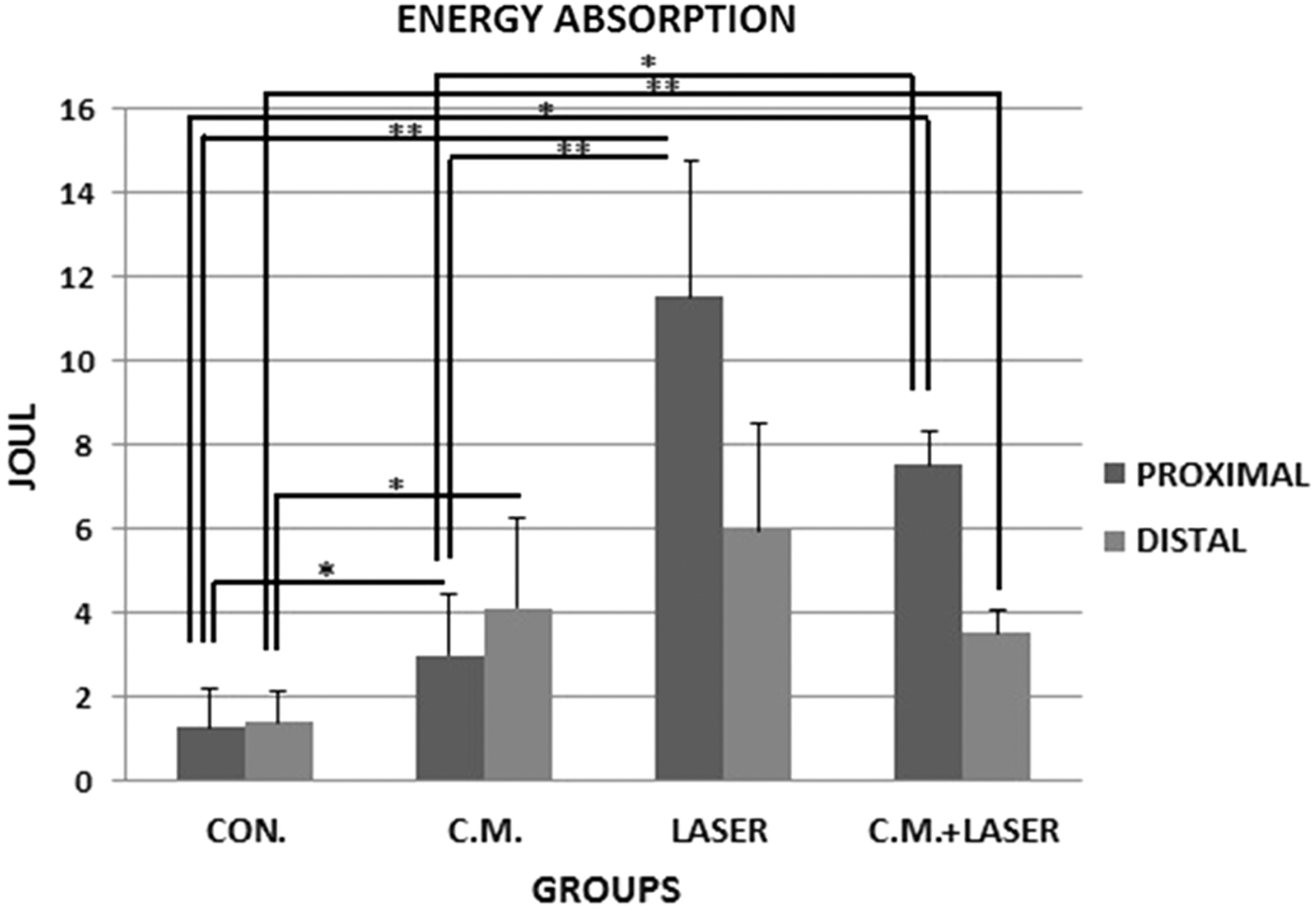
Mean ± SD of energy absorption in the study groups was compared by using the Mann–Whitney test. There was a significant difference in energy absorption between third, fourth, and second groups compared with the control group (p = 0.004, p = 0.011, and p = 0.046, respectively). There was also a significant difference in energy absorption of CM-treated rats compared with the third and fourth groups (p = 0.007, p = 0.028, respectively). *<0.05, **<0.01.
We classified the results of biomechanical examination into (1) results of proximal wounds versus distal wounds, (2) comparing the proximal wounds in the groups, and (3) comparing the distal wounds in the groups.
Proximal wounds versus distal wounds
There was a significant increase in bending stiffness, maximum force, and stress high load in the proximal wounds in the fourth group (LASER+CM) compared with the distal wounds in the same group (Mann–Whitney test, p = 0.04, p = 0.016, p = 0.047, respectively).
Comparing the proximal wounds of the groups
Bending stiffness
There was a significant increase in bending stiffness in the third (LASER), fourth (LASER+CM), and second (CM) groups compared with the control group (p = 0.004, p = 0.006, and p = 0.032, respectively). In addition, there was a significant increase in bending stiffness in laser-treated rats compared with the second and fourth groups (p = 0.007, p = 0.012, respectively).
Maximum force
There was a significant increase in maximum force in the third, fourth, and second groups compared with the control group (p = 0.004, p = 0.008, and p = 0.044, respectively. Furthermore, there was a significant decrease in maximum force in CM-treated rats compared with the third and fourth groups (p = 0.014, p = 0.042, respectively).
Stress high load
There was a significant increase in stress high load in the fourth, third, and second groups compared with the control group (p = 0.011, p = 0.016, and p = 0.044, respectively).
Energy absorption
There was a significant increase in energy absorption in the third, fourth, and second groups compared with the control group (p = 0.004, p = 0.011, and p = 0.046, respectively). There was also a significant decrease in energy absorption of CM-treated rats compared with the third and fourth groups (p = 0.007, p = 0.028, respectively).
Comparing the distal wounds of the groups
Bending stiffness
There was a significant increase in bending stiffness in the second and fourth groups compared with the control group (p = 0.025, p = 0.028, respectively).
Maximum force and stress high load
There was a significant increase in maximum force and stress high load in CM-treated rats compared with the control group (both p = 0.037).
Energy absorption
There was a significant increase in energy absorption in the second and fourth groups compared with the control group (p = 0.025, p = 0.028, respectively).
Discussion
The biostimulatory effect of PWLLLT in our study is demonstrated by a significant increase in bending stiffness, maximum force, and stress high load compared with the control group.
The wounds on the skin in DM exhibited impaired healing, including delayed acute wounds and chronic wounds, whereby they generally have failed to progress through the normal stages of healing. Such wounds frequently enter the state of pathological inflammation due to the delayed, incomplete, or uncoordinated healing process. 32 The amount of type I collagen and the ratio of type I to III collagen dramatically decrease in the skin in diabetic rats. Therefore, predisposition of diabetics to wounds may result in the impairment of tissue integrity at baseline; in addition, it can cause a defect in the regulation of synthesis in collagen proteins. 13 According to the statistical reports, animals with diabetes presented 30% less load of collagen in their skin compared with the control group. 33 The animals with DM, which did not attain the treatment, had less strength in their wounds than the treated ones. 34
In our laser-treated rats, the healing in wounds significantly increased the maximum force, stress high load, and bending stiffness on the 15th day postinjury compared with the control group. According to our data, the biomechanical analysis indicated that the repairing system in wounds in the laser-treated ones was significantly stronger (maximum force) than the control wounds, even by the time strength was normalized for minor variation in the sample size (stress high load). The ability of stretch in the skin is quite an essential function in healthy people, especially where skin crosses the joints. Apparently, the usage of laser as the treatment of choice caused the wound healing process to be much faster and stronger. It is a revealing fact that in the situation of stretch, the strain value is higher than the control group. 35 Based on the results, it has been indicated that PWLLLT can facilitate joint movements in the involved limb. The function of this mechanism is increasing the elasticity of the repaired wound that overlies joints. During the mechanical testing, resistance to tension by straightening, uncoiling, or unfolding of fibrils and molecules results in the linear region of the load–deformation curve. These moduli are often defined as the bending stiffness. 36 In the current study, the wounds in laser-treated rats showed a significant increase in bending stiffness compared with the control wounds. A higher bending stiffness was shown because of the following effects: increased fibrillar molecules per unit area, increased fibril diameter, or increased cross-linking of fibrillar molecules. 36
In this study, we sought to explore the combined effect of PWLLLT and the hBM-MSC-CM-enhanced wound healing procedure in type I diabetic rats compared with PWLLLT or hBM-MSC-CM solo.
According to the recent studies in vivo and in vitro, positive effects of CM on enhancement of wound healing in healthy subjects and diabetic animals were reported. 24 –27 Zhou et al. evaluated the effect of conditioned medium in adipose-derived stem cells (ADSC-CM) in wound healing, after fractional carbon dioxide laser resurfacing (FxCR) in the human skin. The population of 19 people was irradiated by FxCR in both arms. ADSC-CM was applied in the laser-treated site. They found that the index for erythema, melanin, and transepidermal water loss in ADSC-CM-treated skin was significantly lower than the side that was counted as the control. The mRNA expression for type III procollagen in the ADSC-CM-treated group was 2.6 times more compared with the control group. Zhou et al. concluded that application of allograft ADSC-CM is an effective method for enhancing wound healing after FxCR. 37 In other scientific reports, it has been indicated that BM-MSCs secrete certain cytokines, which include vascular endothelial growth factor (VEGF), basic fibroblast growth factor (bFGF), IL-6, and monocyte chemoattractant protein-1 (MCP-1). 38 –40 Much of the wound healing afforded by MSCs can be achieved by treatment with cell-free MSC-CM. Thus, it is expected that MSC-CM sustains advantages by containing stem cell paracrine factors without the risk of immunological side effects in MSCs. 41
In the ongoing study, according to the our previous study, 27 we observed that the alternative for using hBM-MSC-CM twice during the treatment was more effective than the placebo group; as a matter of fact, we used hBM-MSC-CM twice during the treatment. Our results showed that the biomechanical parameters of hBM-MSC-CM-treated rats were significantly higher than the control ones; at the same time, some biomechanical values were significantly lower than ones in the laser-treated group. The results may be attributed to few drawbacks; for example, low concentration of many cytokines and growth factors should be into the normal range before therapeutic utilization of MSC-CM42; otherwise, tremendous volume of CM should repeatedly be injected into the damaged tissues 43 to attain a positive outcome. However, it seems that administration of hBM-MSC-CM more than twice could increase the biomechanical parameters of hBM-MSC-CM-treated diabetic wounds.
Several studies have indicated that LLLT is effective for the enhancement of the viability and proliferation of stem cells with appropriate energy density and wavelengths. 44 In addition, LLLT increases the gene expression and release of several growth factors. 45 However, our results showed that biomechanical values for laser-treated rats were higher than ones in the fourth group. It was observed that the combined effects of PWLLLT and hBM-MSC-CM, which were used in our experiment, neither had a synergistic effect on hBM-MSC-CM activity nor increased the biomechanical results. Furthermore, Santuzzi et al. evaluated the isolated and combined effects of LLLT (632 nm, 12 s, spot size: 1.5 cm, 4 J/cm2, during 3 consecutive days); in addition, they evaluated ICOX2 (50 mg/kg, for 10 days before the surgery) in the reepithelialization of incisional wounds in mice. Mice were divided into four groups: the control group, the group treated with LLLT, the group treated with ICOX2, and the group with combined therapy (LLLT+ICOX2). They found that the LLLT group and the celecoxib group showed an increase in skin reepithelialization compared with the control group; however, the therapy in combination showed no differences. As for keratinization, the group with combined therapy showed a reduction in keratinocytes compared with the control group. 46
The following hypothesis explains lack of sufficient combined biostimulatory effect of PW (LLLT+hBM-MSC-CM) in the treatment of diabetic rats: 1. The combination of hBM-MSC-CM and PWLLLT treatments caused a reduction in the biomechanical parameters of the wounds. It could be associated with the effect of the PWLLLT in regulating, expression, and synthesis of cytokines and growth factors, which were involved in wound bed containing hBM-MSC-CM. 2. The PWLLLT protocol, which was used in the current work, was not accurate enough in the stimulation of fibroblasts that received hBM-MSC-CM. 3. These results may be attributed to few drawbacks; for example, the low concentration of some cytokines and growth factors should be reconsidered before therapeutic utilization of MSC-CM.
42
Otherwise, a large volume of CM should be repeatedly injected into the damaged tissues
43
to get positive results. 4. The fibroblasts and other cells in wound bed in the fourth group were under several external strains, such as type I DM, surgery, enforcing PWLLLT for 13 days, and injecting 500 μL of hBM-MSC-CM twice in the experiment for the mentioned groups. The above stressors could cause an inverse effect on the wound healing process as well. 5. Similarly, Fekrazad et al. evaluated the combined effect of LLLT and MSCs on bone regeneration. They made bone defects in the calvaria of rabbits. The rabbits were randomly divided into four groups: a control group that received no treatment; laser-treated rabbits (810 nm, 4 J/cm2); MSC-treated rabbits; and combination treatment of LLLT and MSCs. The histological examination revealed a statistically significant increase in the new bone formation in the LLLT group compared with the control and the other two experiment groups. There was no significant difference in bone formation of the control group compared with the experimental groups filled with MSCs. In addition, inflammation was significantly increased in MSC-treated groups compared with the control defects and the laser group. Fekrazad et al. concluded that LLLT could be effective in bone regeneration; however, there was no evidence to support the synergistic effect when applied in conjunction with MSCs. Fekrazad et al. reported that high amount of inflammation in MSC-treated groups could be a contributing factor to reduced bone formation.
47
It appears that in the present study, hBM-MSC-CM could be a quite important factor to reduce biomechanical properties of hBM-MSC-CM-treated wounds by increasing the inflammatory reaction.
Conclusions
It was ultimately concluded that PWLLLT with 890 nm wavelength, 80 Hz frequency, and 0.2 J/cm2 energy density significantly accelerated the wound healing process in the experimental model for STZ-induced type I DM. Definitely, the PWLLLT was statistically more effective compared with the hBM-MSC-CM. With the emergence of this approach, we described the benefit of using this therapy as a noble and promising alternative for treatment of DFUs in type I diabetic patients. The cellular and molecular mechanisms regarding the effect of PWLLLT on healing of diabetic rats should be elucidated by further researches. Moreover, further studies using the PWLLLT on the experimental model in type II DM are suggested.
Footnotes
Acknowledgment
The authors would like to thank the Vice Chancellor of Research at Shahid Beheshti University of Medical Sciences (Tehran, Iran) for financial support (Grant No. 5137).
Author Disclosure Statement
No competing financial interests exist.