
Abstract
Introduction
T
Three recent, large retrospective studies 3 –5 and a review of 10 cases 6 analyzed the characteristics and treatment of oral pyogenic granulomas. Al-Shamiri et al. 7 reviewed three case reports 8 –10 describing pyogenic granulomas related to a dental implant and one case report of co-development of a pyogenic granuloma and a hemangioma around a dental implant. 11 A recent study by Anitua and Piñas 12 described the clinical and histopathological findings for pyogenic granulomas associated with dental implants in 10 patients. So far, only a single publication has described a pyogenic granuloma adjacent to a dental implant treated with a laser, specifically an Er:YAG laser. 1
Considering the instrument's possible advantages, a CO2 laser was used to remove a pyogenic granuloma associated with dental implants 1 year after implant placement.
Patients and Methods
A male patient (67 years) suffering from a peri-implant gingival hyperplasia in the left lower jaw presented at the Department of Oral Surgery and Orthodontics, University Clinic of Dental Medicine and Oral Health of the Medical University of Graz. One year earlier, his dentist had supplied him prosthodontically with a mandibular total denture that was retained by four interforaminal implants (Ankylos® Dentsply Implants). A ball attachment was integrated in implant 32 and there were three conical attachments (SynCone® abutments) in implants 34, 42, and 44. Following a conventional protocol, the prosthodontic retainments were integrated after about 3 months of submerged healing.
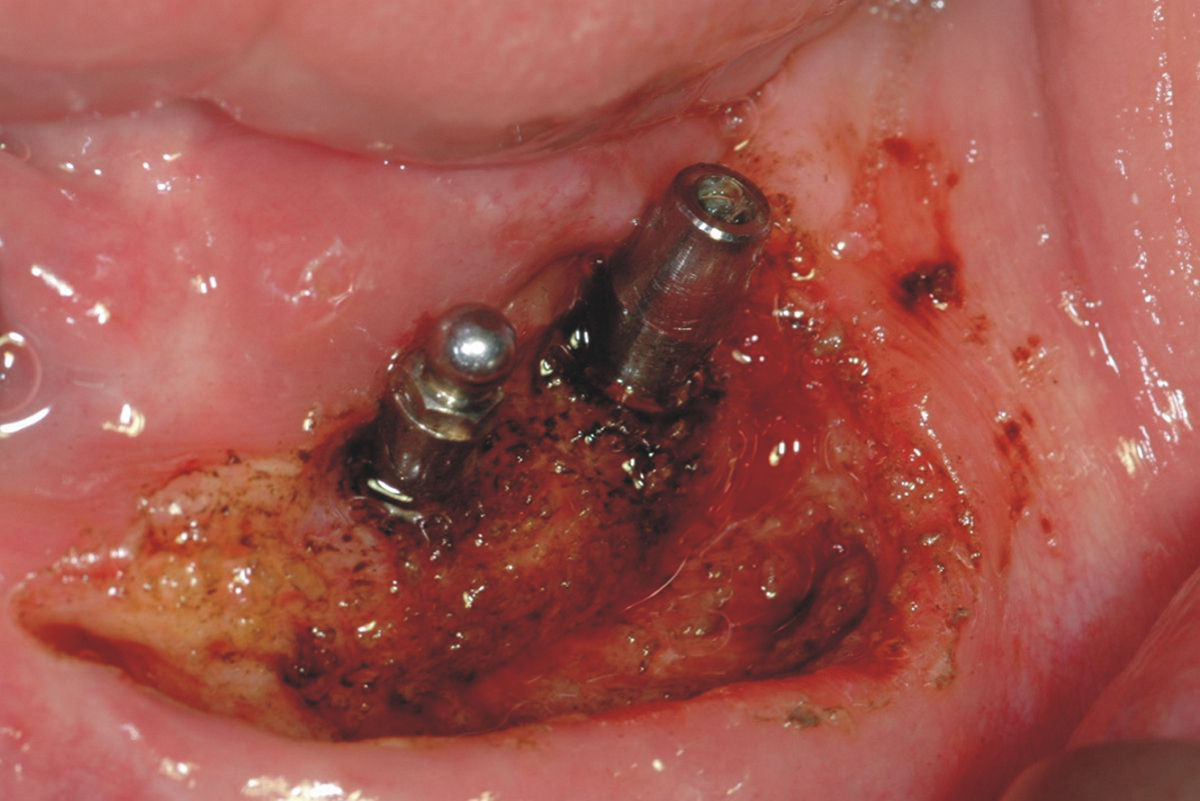
The patient complained of chronic purulent inflammation and painful nodular proliferations around the two implants in the left lower jaw immediately after the prosthetic restoration. His dentist undertook two unsuccessful attempts to remove the inflammatory hyperplastic lesions around the two implants with electrocauterization. At the first examination, the patient presented poor dental hygiene and inflammatory mucosal hyperplasia with profuse bleeding on probing around the implants in the left lower jaw. There was no fixed keratinized mucosa around the abutments of these two implants (Fig. 1).

Exophytic lesions around the implants in the left lower jaw.
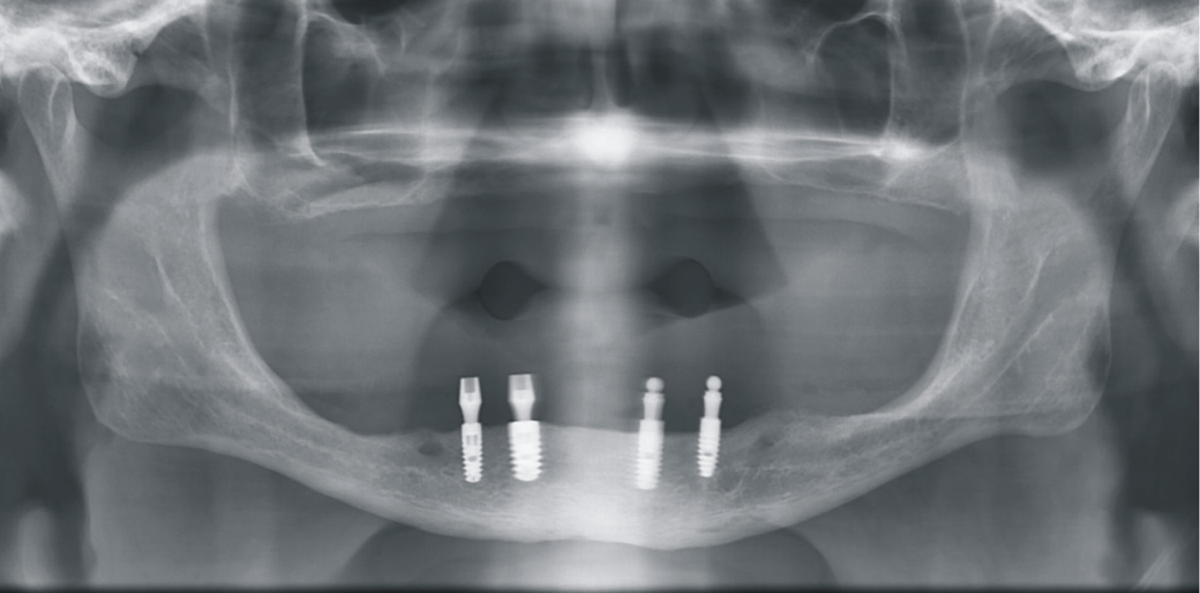
The panoramic X-ray showed mild to moderate vertical peri-implant bone loss at implant 3, whereas the other implants were unremarkable (Fig. 2).
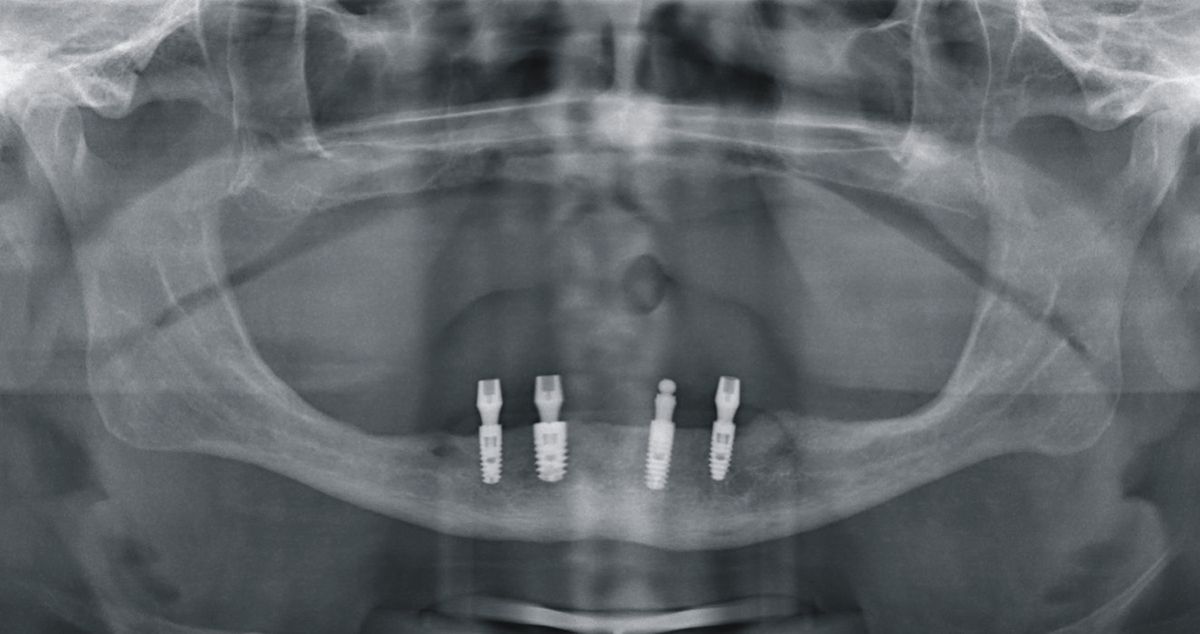
Panoramic X-ray on first visit (ball attachment 32).
Pre-treatment of the inflammatory lesions at the two left implants consisted of mechanical and chemical decontamination, including rinsing with 3% hydroperoxide solution until the acute inflammation subsided.
The hyperplastic tissue was removed down to the periosteum under local anesthesia with a surgical CO2 laser (Lasram, Budapest, Hungary; model OPAL 25, 25 W continuous wave, 10.600 nm, gas laser). This gas laser emitting laser light with a wavelength of 10,600 nm was set to an output power of 3 W in a continuous-wave mode. A non-contact handpiece with a focal length of 127 mm was used to focus the beam to a spot with a diameter of 0.25 mm. For work close to the implant, an additional applicator tip with a ceramic tube was attached to the handpiece (Fig. 3). This ceramic tube had an inner diameter of 0.5 mm; the diverging laser beam had a spot diameter of 0.7 mm on the tissue (Table 1).
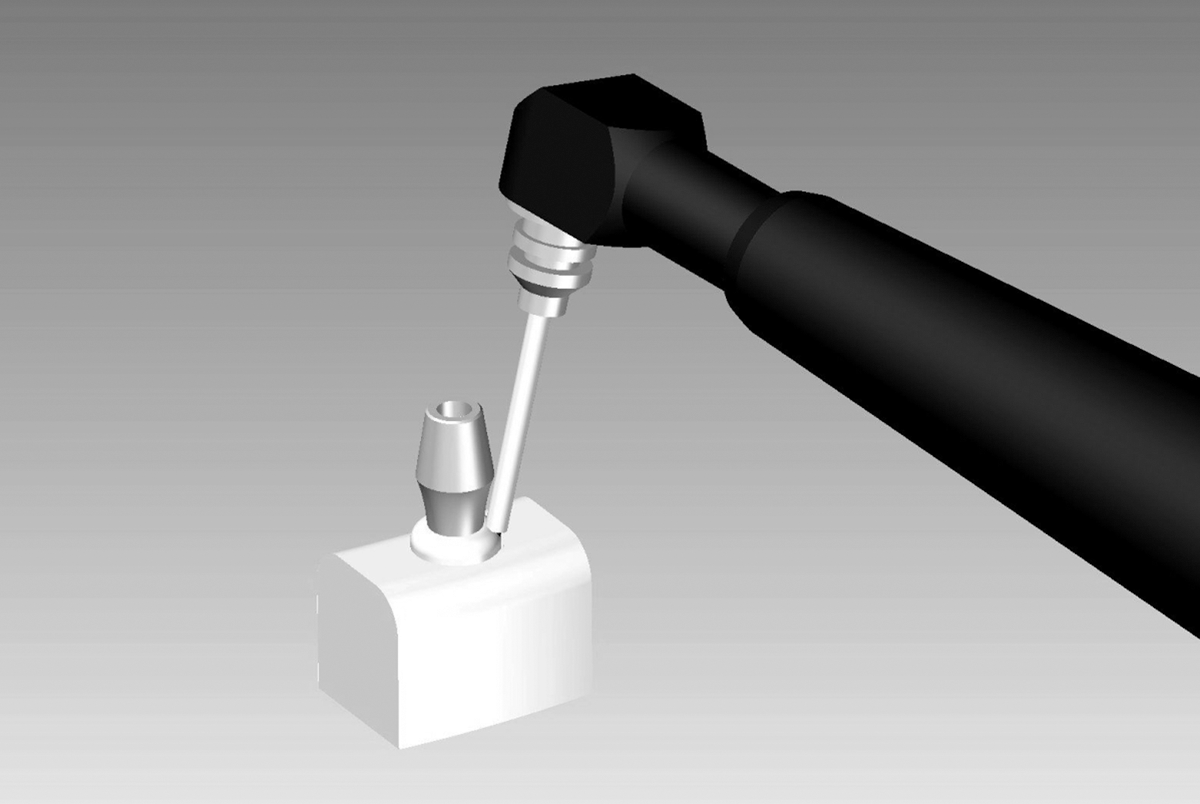
Schematic showing the handpiece with ceramic tube and guidance of the laser beam tangentially to the implant surface.
Dose and cumulative dose have no meaning when moving the handpiece in cutting mode.
During the excision of the lesions, the laser beam was applied intermittently and guided tangentially to the implant surface to avoid thermal damage to the peri-implant tissues. A vestibuloplasty—also by CO2 laser—was subsequently performed on the buccal side with the same power setting but without the applicator tip (Fig. 4).
Appearance directly after laser surgery.
Both tissue specimens, examined at the Institute of Pathology of the Medical University of Graz by one of the authors (A.B.), were diagnosed as pyogenic granulomas (Fig. 5).

Histopathologically, the pyogenic granuloma features a dome-shaped, superficially ulcerated proliferation of capillary-rich tissue.
One day after surgery, the surface of the wound was covered by a thick fibrinous layer with no bleeding or swelling; the patient did not report any pain. Healing was uncomplicated, and re-epithelialization was completed after 1 month. There was excessive keratinized fixed peri-implant mucosa and a deepened vestibulum but persistent inflammation around the peri-implant mucosa (Fig. 6). Therefore, the decision was taken to replace the conical abutment of implant 34 with a ball attachment, and so prevent mechanical irritation to the adjacent peri-implant tissue. Two weeks later, that is, 6 weeks after surgery, the peri-implant mucositis in region 34 had subsided (Fig. 7).

Inflamed mucosa around the implant in region 34 with the conical abutment 1 month after laser surgery.
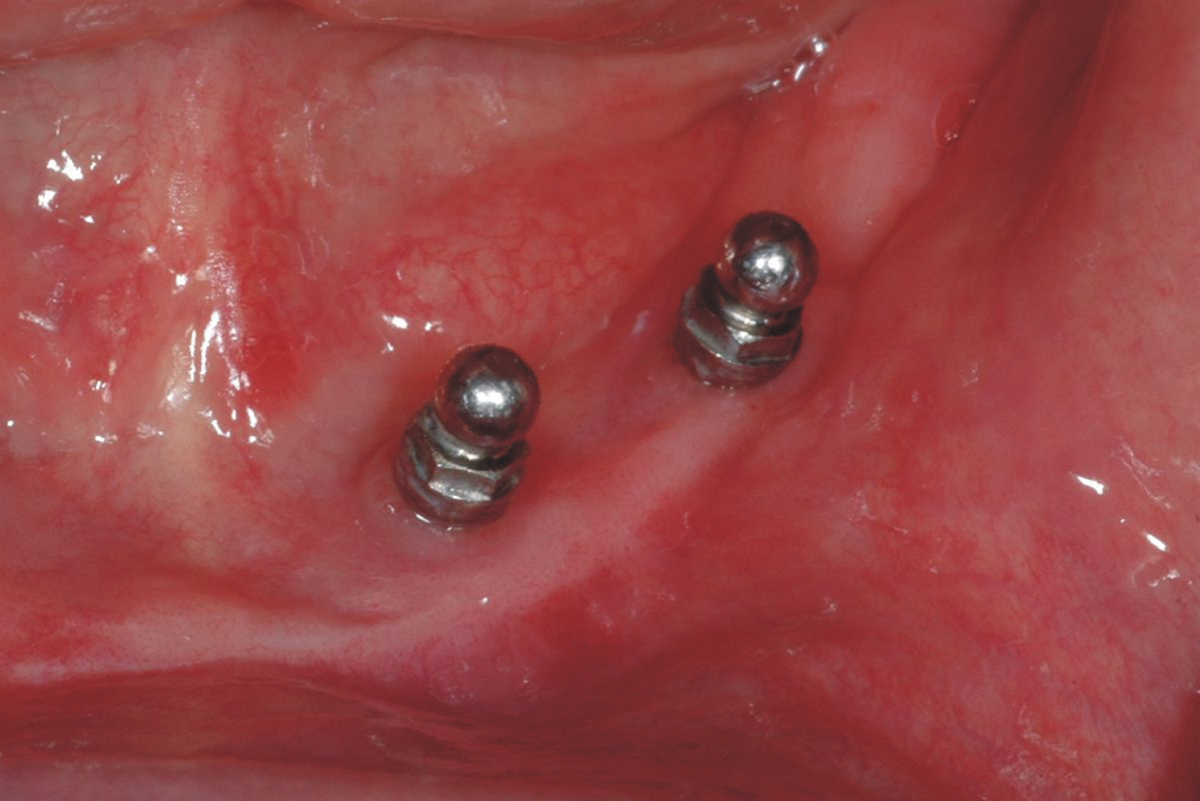
Uninflamed mucosa around both implants 2 weeks after replacement of the conical abutment of implant 34 with a ball attachment.
Further follow-ups after 6 months and 1 year showed a stable result without any inflammation, no recurrence of the hyperplastic tissues, and steady keratinized fixed peri-implant mucosa. The panoramic X-ray taken at the follow-up 1 year after laser surgery showed neither a vertical peri-implant defect nor impairment of osseointegration (Fig. 8).
Panoramic X-ray taken 1 year after laser surgery.
Discussion
A thorough review of the relevant literature indicates that this is the first article of successful removal of an oral peri-implant pyogenic granuloma using the CO2 laser technique.
Among the many methods of removing an oral pyogenic granuloma, the most common is excision with the scalpel and electrocautery. The literature describes a number of other methods, such as cryosurgery, 13 sclerosing agents, 14 injection of absolute ethanol, 15 and treatment with corticosteroids. 16 Laser excision has also emerged as an established option for pyogenic granulomas, and the following laser types have been used: Nd:YAG laser, 17 –19 CO2 laser, 18,20 diode laser, 21,22 and Er: YAG laser. 23
Complete excision of pyogenic granuloma in conjunction with a dental implant has been described by Dojcinovic et al., 8 Olmedo et al., 9 Etöz et al., 10 Kaya et al., 1 and Kang et al. 11 Specific circumstances sometimes required additional measures: Dojcinovic et al. 8 curetted the surrounding tissues and replaced the oversized healing cap of the implant. Olmedo et al. 9 curetted the bone surface. Etöz et al. 10 removed the failed implant, curetted the empty socket and around the other implants, covered the implants with platelet rich fibrin (PRF) membranes, and finally closed the mucoperiosteal flap with sutures. Kang et al. 11 completely coagulated the wound area with electrocautery after the excision. Most recently, Anitua and Piñas 12 described clinical and histopathological findings for pyogenic granulomas associated with dental implants in 10 patients. The lesions were conventionally excised, and the defects were covered with an autologous fibrin membrane.
One pyogenic granuloma adjacent to a dental implant was excised by Kaya et al. 1 with an Er:YAG laser. The authors then elevated a mucoperiostal flap, decontaminated the implant surfaces with the laser in a non-contact mode, and sutured the flap.
Many authors have documented the advantages of the CO2 laser for soft tissue excisions 24 –29 : Not only does the excellent hemostatic effect allow a good view of the surgical field, but also the surrounding tissues are not injured, sutures are not needed, there is less risk of infection as well as less pain and swelling, and there is only minimal scarring.
Both shallow penetration and good hemostasis with the instrument allow accurate preparation, especially around implants. As the optical penetration depth is only 17 μm in soft tissues, 30 the resultant necrotic zone is quite small. The good hemostatic effect of the CO2 laser is due to a combination of a low-power setting in continuous-wave mode and slow application to provide sufficient time for heat diffusion.
Basically, the Er:YAG laser could also be used but its hemostatic effect is inferior to the CO2 laser. The very small optical penetration depth of 3 μm in soft tissues 30 in conjunction with the short pulse length of several hundred microseconds greatly limits heat diffusion into the adjacent tissue. Even when the pulse length is extended into the millisecond range, hemostasis is poorer than with a CO2 laser. Further, an Nd:YAG laser or various diode lasers show penetration depths of more than 2 mm in soft tissue, 30 leading to a perfect hemostatic effect. However, these lasers create a thick zone of necrosis.
Ganz, 31 Oyster et al., 32 Swift et al., 33 Barak et al., 34 Mouhyi et al., 35 Kreisler et al., 36 and Lambrecht et al. 37 described temperature changes in metal implant surfaces when soft tissue adjacent to implants is removed with a CO2 laser. The instrument can only be used safely when a low-power setting is chosen and the laser beam is applied intermittently. 31,33,34,37 Addressing the risk of overheating, in an in vitro study, Leja et al. 38 compared four different lasers applied on implants inserted in bovine ribs and found the highest and fastest temperature increase with the CO2 laser.
Besides the risk of overheating of implants adjacent to laser application, possible direct laser damage to the bone also has to be considered. In 1970, Goldman et al. 39 had already studied the effects of CO2 laser on bone. Subsequent investigations showed that the thermal laser damage to bone structures leads to delayed and sometimes incomplete healing of bone defects produced by the laser. 40,41 Krause et al. 42 undertook a more detailed study of the adverse effects of CO2 laser irradiation to the bone with different power settings. In 1991, however, Hibst and Keller 43 demonstrated that the Er:YAG laser is very useful for preparing bony tissue, and it is especially effective with osteotomies.
In the presented case, a soft tissue pathology adjacent to osseointegrated implants was removed by a CO2 laser. Possible adverse thermal side effects of the CO2 laser on implants were avoided by reducing the power setting to 3 W, choosing a pulsatile interruption mode for the continuous-wave laser light, and guiding the beam tangentially to the implant surface. Finally, a special ceramic tube applicator reduced the risk of overheating close to the implant surface (Fig. 3). As mentioned in the Patients and Methods section, though the pyogenic granuloma was removed down to the periosteum, care was taken not to penetrate it and not to damage the underlying bone. An X-ray taken 1 year later supports the conclusion that CO2 laser did not cause thermal damage to the surrounding bony tissue; there was also no sign of either a vertical peri-implant defect or impairment of osseointegration.
To avoid re-inflammation, an increased extent of keratinized fixed peri-implant mucosa was created by performing a vestibuloplasty with the CO2 laser. In contrast to Etöz et al. 10 and Kaya et al., 6 the wound area was not closed with a flap but was left uncovered for secondary epithelization. As described by Dojcinovic et al., 8 efforts were made postoperatively to eliminate the persistent mechanical irritation to the mucosa surrounding the implant. This entailed removal of the conical abutment of implant 34 with insufficient gingival height and its successful replacement with a ball attachment.
Conclusions
With correct application and careful choice of parameters, the CO2 laser can both safely and effectively remove soft tissue pathology, even adjacent to dental implants.
Footnotes
Author Disclosure Statement
No competing financial interests exist.