
Abstract
Introduction
T
Laser application is a relatively new method to eliminate microorganisms in root canal systems. The antibacterial effects of these lasers are a function of dose-dependent heat generation, which can char dentin, ankylose roots, melt cementum, and cause root resorption and periapical necrosis. 4 These disadvantages may be overcomed by sensitizing bacteria with a photoactive drug or photosensitizer (PS) able to trigger the release of singlet oxygen and free radicals when exposed to light of appropriate wavelength, a method that is called photodynamic therapy (PDT). 5 The antimicrobial PDT is also called photodynamic antimicrobial chemotherapy, photodynamic antimicrobial therapy, photoactivated disinfection, or lethal photosensitization. 5
Although PDT was initially developed as a cancer and premalignant disease treatment, so far its most successful application has been in ophthalmology, for the treatment of age-related macular degeneration. 6 Other nononcological applications at a less developed stage include treatments for psoriasis, acne vulgaris, arthritis, Barrett's esophagus, and atherosclerosis. 6
The cytotoxic effects of PDT have been used to eliminate pathogenic microorganisms, providing bactericidal properties. The transfer of energy from the activated PS to available oxygen triggers the formation of highly reactive oxygen species, such as singlet oxygen and free radicals, which can kill microorganisms by damaging essential cellular molecules, including proteins, membrane lipids, and nucleic acids. 7,8 In vitro, ex vivo, 9 –24 and in vivo 25 –27 PDT studies, using mostly commercial PSs such as methylene blue (MB) and toluidine blue (TBO), showed that this approach has the potential to maximize the root canal disinfection. PDT has also been tested as a promising approach to eradicate oral bacteria and caries, 28 periodontitis, 29 and peri-implantitis. 30
Indocyanine green (ICG), also known as Cardio-Green, (4,5-benzoindotricarbocyanine—C43H47N2NaO6S2) is a negatively charged polymethine dye with 775 kDa molecular weight. The absorption spectrum of ICG is high at wavelengths around 800 nm. ICG is a water-soluble anionic cyanine dye that acts as PS, approved by the US Food and Drug Administration for fluorescence angiography in ophthalmology and, also, in diagnostic assessment of liver function and cardiac output. ICG is of very low toxicity and is rapidly excreted from the body so that any possible damage to host tissues is limited. 31
ICG is activated by light in the near-infrared (NIR) region of the spectrum (between 800 and 810 nm) compared to MB and TBO, which are thiazines and absorb in the red part of the spectrum (660 and 634 nm, respectively). In this spectrum, the electrons of its π-orbital conjugated bonds can be excited resulting in energy transfer to singlet oxygen with a rather high efficiency of photodynamic action. 32 In comparison to the shorter wavelengths of light (<700 nm) used in the majority of current PDT modalities, infrared light (>800 nm) allows for deeper tissue penetration, according to photodynamic periodontal therapy studies. 31,33
The purpose of this ex vivo study was to determine whether the light-activated antimicrobial agent, ICG, could be used to kill E. faecalis biofilms in contaminated root canals when irradiated and activated with near-infrared light doses.
Materials and Methods
Bacterial culture
E. faecalis (ATCC 29212) was the microorganism used in this study, and bacterial cultures were maintained by weekly subculture on Aesculin bile Agar (Oxoid Ltd, UK). For experimental purposes, the microorganism was grown in the presence of 85% N2, 10% H2, and 5% CO2 at 37°C in an anaerobic chamber for 72 h. The bacterial cells were scraped, aseptically suspended in 30 mL of brain–heart infusion (BHI) broth (Oxoid Ltd), and dispersed by vortexing and repeated passages through pipette tips. Then, the bacterial cells were harvested by centrifugation (two cycles of 1000 rpm for 5 min) and were resuspended in phosphate-buffered saline (PBS; Invitrogen, UK). The bacterial cell concentration was measured using a spectrophotometer (Jenway 6305, UK) to obtain an infection inoculum of ∼108 cells/mL [wavelength 600 nm; 0.1 optical density (OD) unit]. This bacterial suspension was considered as the baseline concentration.
Tooth sample preparation
A total number of 90 freshly extracted single-rooted human teeth were stored in 0.5% NaOCl solution for 2–4 weeks. The study conformed to the ethical guidelines of the World Medical Association Declaration of Helsinki. The presence of a single root canal was determined by radiographs taken from mesiodistal and buccolingual directions and confirmed visually after conventional access preparation.
Specimens were decoronated to a standard root segment length of 12 mm using a cylindrical diamond bur adjusted in a high-speed handpiece under water coolant. The root canal orifices were accessed and working lengths were determined visually by identifying a size 15 K-file (Dentsply Maillefer, Switzerland) at the anatomical apex and subtracting 1 mm coronally. The root canals were cleaned and shaped by using hand K-files (Dentsply Maillefer) and NiTi rotary files (ProTaper® System; Dentsply Maillefer, Sequence: SX, S1, S2, F1, F2, F3), under copious irrigation of 2.5% NaOCl using a 30G Endo-Eze needle (Ultradent, UT). Final apical patency was established with a size 30 K-file (Dentsply Maillefer) and a size F3 NiTi rotary file (ProTaper System; Dentsply Maillefer) to allow for an adequate apical aperture for flushing of microbial aggregates during the microbial analysis process.
After canal preparation, an aliquot of 1 mL of 17% EDTA solution (Eudent Ed-Sol; Intermed S.A., Greece) was left in situ for 3 min and replaced by 1 mL of 2.5% NaOCl for 3 min. Rinsing with 3 mL of saline before and after EDTA solution was part of the irrigation protocol. The tooth specimens were then placed in 1.5-mL sterile microcentrifuge tubes (StarLab GmbH, Germany) containing 1 mL of PBS and autoclaved at 121°C for 20 min. Following autoclave sterilization, PBS was aspirated from the microcentrifuge tubes under sterile conditions. One milliliter (1 mL) of stock solution of BHI broth containing ∼109 cells of E. faecalis (wavelength 600 nm; 1 OD unit equals ∼109 cells/mL) was syringed into each prepared root canal system using a 30G Endo-Eze irrigation needle (Ultradent, UT). After intracanal injection, the entire specimen was fully immersed in the medium. The tubes were kept in an anaerobic chamber (85% N2, 10% H2, and 5% CO2 at 37°C) for 72 h to allow infection to occur.
Testing procedures
Ninety root specimens were prepared and 84 of them were infected as described above. The experimental groups were as follows: (1) 12 specimens treated with PDT (ICG+, light+) in medium-energy fluence (143 J/cm2), (2) 12 specimens treated with PDT (ICG+, light+) in high-energy fluence (286 J/cm2), (3) 12 specimens exposed only to laser irradiation (high-energy fluence, 286 J/cm2, 1 W output power) without ICG (ICG−, light+), (4) 12 specimens exposed only to ICG without irradiation (ICG+, light−), (5) 12 specimens irrigated with 2.5% NaOCl solution, (6) 12 specimens irrigated with 2.5% NaOCl solution and additional PDT in high-energy fluence (286 J/cm2), (7) no irradiation and ICG (ICG−, light−) served as positive control (12 specimens), and (8) no bacterial biofilm growth (PBS solution) served as negative control (six specimens).
For the root canal irradiation, an NIR diode laser (Doctor-Smile; Lambda Scientifica, Italy) with an output power of 5 W and a wavelength of 810 nm in continuous wave mode was used. The unit was connected to a 300-μm-diameter optical fiber, which was adjusted to the working length of each specimen (Fig. 1). Following the manufacturer's instructions, spiral movements of the optical fiber tip were performed from the apical to cervical direction to uniformly distribute the light inside the root canal. The light was applied in the root canal of the specimens for 60 sec in total, during a set of three light exposures of 20 sec each. A 20-sec break followed each one laser light irradiation dose. The overall power density was measured at 2.38 and 4.7 W/cm2 with an actual power output of 0.5 and 1 W, respectively, corresponding to medium-energy (143 J/cm2) and high-energy (286 J/cm2) fluence. The exact dose of energy fluence rate and power density was calculated based on the equation used in previous studies. 10,14 Before each test, the power output at the tip was measured with an optical power meter (Ando AQ21058, Yokogawa, Japan).
Tooth specimen placed in microcentrifuge tube, filled with photosensitizer ICG, and irradiated with near-infrared diode laser, coupled to a 300-μm-diameter optical fiber. ICG, indocyanine green.
Each specimen in groups 1, 2, 4, and 6 was filled with 1 mL of ICG solution using a 30G Endo-Eze needle (Ultradent, UT). Fresh stock solution was prepared immediately before each experiment by diluting ICG powder (Sigma-Aldrich) in PBS. The final concentration used in this study was 100 μg/mL and it was maintained in the dark for 15 min. After injection, the entire specimen was fully immersed in the ICG solution for 15 min before photoactivation, to be continuously exposed to the PS. In groups 5 and 6, 10 mL of 2.5% NaOCl was irrigated for 2 min in each specimen using a 30G Endo-Eze irrigation needle (Ultradent, UT) adapted to a disposable plastic syringe and placed up to 4 mm short of the apex. The same teeth were irrigated with 1 mL of 17% EDTA (Eudent Ed-Sol; Intermed S.A., Greece), which was left in the canal for 3 min. After a final irrigation with 5 mL of 2.5% NaOCl, 1 mL of 5% sodium thiosulfate (Na2S2O3; Scharlau Chemie, S.A., Spain) was used for 5 min to neutralize the NaOCl. The canal was then rinsed with 1 mL of sterile NaCl solution.
Sampling procedures were as follows: All contents of tested root canals were flushed using an extrusion movement by irrigating 1 mL of PBS solution through a 30G Endo-Eze irrigation needle (Ultradent, UT). The bacterial suspension, derived from the apex, was collected into a sterilized 1.5-mL Eppendorf tube (StarLab GmbH). Sevenfold serial dilutions (neat to 10−7) in Eppendorf tubes containing maximum recovery diluent solution (Scharlau Chemie, S.A., Spain) were prepared and 0.1 mL aliquots were vortexed, spread, and plated on plate count agar (Merck Millipore, Germany) Petri dishes. After incubation for 48 h at 35°C ± 2.0°C, the number of colony-forming units (CFUs) was counted and calculated, using viable count estimation based on dilution factors. All experiments were performed twice in triplicate.
Statistical analysis
Values are expressed as mean log10 CFU levels ± standard deviation. Cell counts were logarithmically transformed to normalize the data before statistical comparison. Comparisons between means of groups were analyzed using Student's t test and one-way analysis of variance. The statistical significance was set at p < 0.05 for all analyses.
Results
The results represent the mean values of log10 CFUs calculated with reference to the nontreated positive control samples (group 7). The application of PDT (group 1 and 2), regardless the overall power and energy fluence, resulted in a significant reduction of the bacterial load to ∼4 and 4.8 log10 in viable counts, respectively, meaning potential disinfection of 99.99% (p < 0.01). The application of laser alone (group 3) and the PS without laser activation (group 4) had no significant effects on the bacterial load, even when a small 0.4 log10 (60%) reduction in viable counts was observed in both groups (p > 0.05). The number of bacteria was significantly reduced (p < 0.001) when 2.5% NaOCl solution was applied (group 5), resulting in 5.1 log10 reduction (99.999%). The highest significant reduction (p < 0.001) of 5.7 log10 in viable counts (99.999%) was observed when 2.5% NaOCl and PDT was added (group 6). Intergroup comparison between PDT groups 1, 2, 5, 6 and 1, 2, 6 revealed no significant differences in bacteria reduction (p > 0.05) in groups 1, 2, 5, 6 and significant differences in groups 3, 4, and 5 (p < 0.001).
None of the experimental groups resulted in entire elimination of the bacterial load. The negative controls yielded no cultivable cells, ruling out contamination of the samples. The results of the viable counts for all tested groups after log transformation (log10 CFU/mL) are given (Fig. 2). In Table 1, the reductions in the number of viable E. faecalis cells after the various treatments are listed.
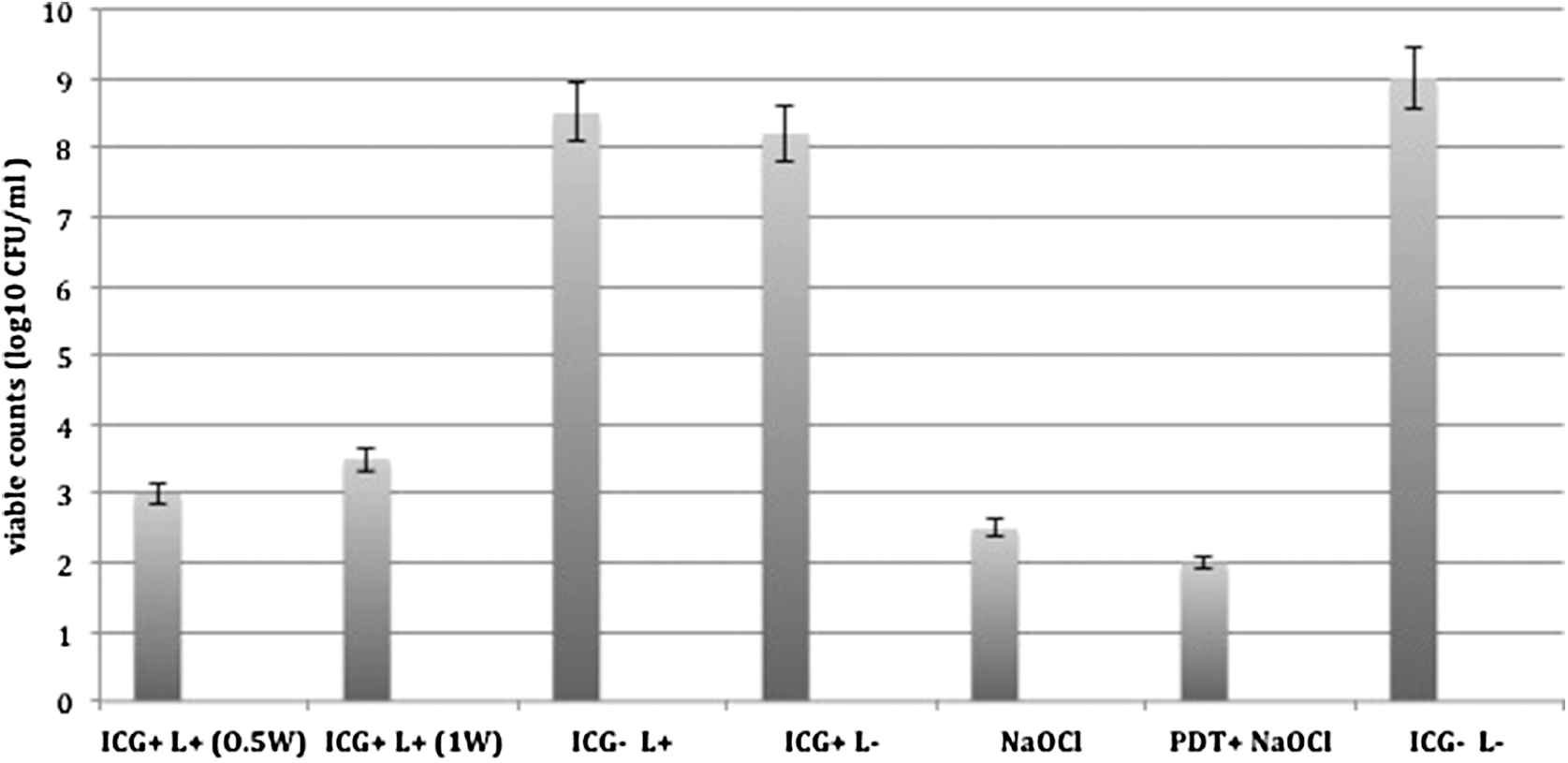
Effect of PDT using ICG in elimination of Enterococcus faecalis. The application of PDT (ICG+, L+) regardless the power was significantly lower than control (ICG−, L−), ICG (ICG+, L−), or laser-alone (ICG−, L+) group. The combination of PDT and NaOCl (PDT+, NaOCl+) was significantly lower than all tested groups. Values are expressed as ±mean standard deviation of triplicate assays. ICG, indocyanine green; L, laser; NaOCl, sodium hypochlorite; PDT, photodynamic therapy.
CFU, colony-forming unit; ICG, indocyanine green; NaOCl, sodium hypochlorite; SD, standard deviation.
Discussion
E. faecalis was chosen as the test organism since it is one of the most common species associated with persistent endodontic infections, also found in primary root canal infections. 2 Studies reporting on antimicrobial therapies against E. faecalis have been published before. 10 However, in the existing literature there is no consensus about the length of time to perform such bacterial growth experiments, with reported time periods ranging from 24 h to 50 days. 34 In the present study, the 72-h model of bacterial growth was adopted. The bacterial total growth was estimated before and after the colonization, using a spectrophotometer and measuring the OD, which is the amount of light passing through a suspension of cells (determination of turbidity). Several disinfection methods alternative to current standard endodontic methodologies have been explored to achieve complete disinfection of the root canal, including laser of different wavelengths and types. 35 PDT is one of the most recent methods in the field of disinfection protocols in endodontics, principally tested against periodontal pathogens. 29
Most of the PDT studies were performed with visible light and common phenothiazine dyes, such as MB and TBO, which have a maximum wavelength absorption of 665 and 625 nm, respectively. 19 Gutknecht et al. used NIR diode laser for disinfection of contaminated root canals by E. faecalis in different dentin thicknesses and achieved penetration to a depth of 500 μm in dentin. 36 In this spectrum, ICG acts as PS and is activated, providing antineoplastic and antibacterial effects. There are two PDT studies reporting lethal photosensitization of ICG on Streptococcus aureus, Streptococcus pyogenes, and Pseudomonas aeruginosa. 32,37
To the best of our knowledge, so far, there has been only one report about the PDT bactericidal effect for the treatment of infectious oral diseases. Nagahara et al. investigated PDT using a nanoparticle formulation of ICG against Porphyromonas gingivalis, which is detected at a high frequency in periodontal pockets of patients with advanced periodontitis, and found a positive PDT-like effect. 33 The present ex vivo study is the first in the field of endodontic research, assessing the effect of ICG and PDT against E. faecalis in experimentally infected human teeth models.
ICG is a rather weak PS because the yields of the triplet state appear low when compared to other PSs used in PDT, such as MB and TBO. 38 Nevertheless, the data obtained in this study have shown that a significant decrease of pathogen numbers can be achieved using both ICG in a concentration of 100 μg/mL and medium to high light dose of 143 and 286 J/cm2, respectively. These findings are in agreement with two other studies using similar ICG concentrations and energy fluencies tested in both gram-positive and gram-negative bacteria. 32,37 A reduction, but not elimination of E. faecalis, was found when diode laser (810 nm) was combined with 0.5% NaOCl and 17% EDTA irrigants. 5 In our study, there was a minimum reduction in mean Log10 CFU units in the experimental group exposed to high-energy fluence rate of irradiation without ICG. The antibacterial effects of these lasers alone are a function of dose-dependent heat generation (photothermic effect), which can cause irreversible pathology to soft and hard oral tissues, if the overall power is not standardized. When a PS is added, the photodynamic effect, rather than the photothermic alone, induces more efficient disinfection, which is less aggressive for the dental and periradicular tissues. 14,18
Several concentrations of different PSs and the antimicrobial effect of PDT have been tested for endodontic disinfection at concentrations ranging from 6.25 to 25 μg/mL for MB and from 10 to 12.5 mg/mL for TBO. 19 The ICG concentration (100 μg/mL) used in our study was based on a pilot study (data not shown) and on the results of previous studies reporting the same concentration of ICG-mediated PDT in planktonic cultures. 32,37 The used concentration of ICG is low compared with the concentrations reported in a case study using ICG (1 mg/mL) and PDT as an adjunctive to periodontal therapy 39 and in an in vitro study investigating the bactericidal effect of ICG-mediated PDT (12.5 mg/mL). 21
PDT has the advantage of the absence of thermal side effects in the periradicular tissues. 31 –33 The lethal photosensitization of PDT is based on photochemical reactions and not thermal effects, as opposed to many high-power laser therapy techniques. 35 The minimization of a thermal effect of PDT makes it potent in eradicating oral bacteria, such as periodontal and endodontic pathogens, without causing overheating of the adjacent tissues. 5
In our study, the bactericidal effect was not heat mediated as the temperature of the bacterial suspensions did not exceed 34°C during irradiation with both output power 0.5 and 1 W, and energy fluence of 143 and 286 J/cm2, respectively. The final temperature rise of <1–3°C from body temperature after the end of irradiation is excluding the hyperthermic effect in the current study. These findings are supported by the results of previous studies using ICG-mediated PDT with medium- and high-power density and fluence rate reporting significant inhibition of bacterial growth. 33
Common setbacks of the PDT studies are the differences in methodology and laser parameters (e.g., energy fluencies, power densities, laser type, optical fiber diameter, duration of emission) leading to difficulty of method standardization. 5 Soukos et al. 10 and Schlafer et al. 40 reported that PDT kills significantly more E. faecalis cells compared to conventional chemomechanical preparation, but in their studies, the wavelengths (635 and 628 nm), fiber diameter (500 μm and 0.4 cm, respectively), power output (1 and 5 W), and PS used (MB and TBO, respectively) were not fixed. Rios et al. 23 used a 30-sec. irradiation, while other researchers 11,18 irradiated the root canals for 5 and 10 min.
Also, the use of an optical fiber that distributes light at 360° in the entire length of the root canal is an important prerequisite for successful targeting of microorganisms in the root canals by PDT. 11 In the current study, the light was emitted from the end of the fiber and a continuous spiral movement was necessary, to provide a better light distribution throughout the dentinal walls. Another researcher 21 using ICG and NIR diode laser reported findings similar to ours, but the study design was different and no data about the power density and the energy fluence were provided.
In our study, flushing with PBS was preferred to collect the bacterial suspension from the root canal. Comparing this method with other methods, such as using paper points, collecting the dentine chips and debris from the root canal walls, or pulverizing the root samples in liquid nitrogen, it proved to be more effective. In conclusion, according to our findings, ICG activated by a diode laser emitting NIR light (810 nm) is bactericidal to E. faecalis in root canals, but is less effective when compared with 2.5% NaOCl. Further ex vivo and in vivo studies comparing other PSs and lasers should be performed to assess accurately the use of NIR diode laser and ICG in endodontic therapy.
Footnotes
Acknowledgments
The authors thank SinaDent Dental Company and AnthosHellas Dental Company, Greece, for providing the diode laser. The authors deny any conflicts of interest related to this study.
Author Disclosure Statement
No competing financial interests exist.