
Abstract
Introduction
T
It is generally believed that roughened surfaces influence microbial colonization by enhancing microbial retention within surface irregularities. Microroughness (Ra: 1 μm) has been suggested to be appropriate for dental implants. 5,6 However, the characteristics of titanium implant surface can be altered by the chemical and mechanical treatments, which in turn change the adhesion patterns of microorganisms. Several studies investigated the effects of different mechanical treatments, such as metal and plastic curettage, air-powder abrasive systems, and lasers on titanium surfaces on texture changes, cleaning efficacy, and fibroblast attachment. 7,8 The surface profile and roughness produced by different instruments could have an important impact on the newly formed biofilm and, consequently, can be an important factor in peri-implant health maintenance. 9 For mechanical debridement, instruments made from plastic and other nonmetals have been applied to avoid damaging titanium surfaces during instrumentation. However, these nonmetallic instruments are ineffective for removing bacterial plaque and calcium depositions. 10 Air-powder abrasive system can effectively achieve surface decontamination; however, the system produced microscopically visible alteration and its application in the narrow vertical bone defect is limited. 6 The effects of the Er:YAG laser on the morphologic characteristics of implant surfaces, effectiveness for removing biofilm, and biocompatibility of osteoblastic and fibroblastic cells were investigated. 6,11,12
There is limited information about the influence of the titanium surface conditions on bacterial adherence, in particular, for surface roughness ranging from 0.2 to 2.7 μm. This study is to identify the relationships between surface conditions of titanium implants and bacterial adhesion, and then to evaluate the effectiveness of three different decontamination methods, including the plastic curettage, air-powder abrasion, and laser irradiation for bacteria-infected titanium implants.
Materials and Methods
Roughening
Commercially available 3-mm-thick Ti-6Al-4V alloys (ASTM F136-84; Titanium Industries, Parsippany, NJ) of 10 × 10 mm2 were selected as the substrate materials. All samples were wet ground with a 1200-grit SiC abrasive paper (3M Wetordry TriMite 734, St. Paul, MN), followed by sandblasting with Al2O3 particles with 50, 100, and 250 μm (Korox, Bego, Bremen, Germany) for 10 sec to produce three different rough surfaces, as listed in Table 1. The air pressure was 3.5 bar using a Taicrown P-002B machine (Taichung, Taiwan) and the distance between the orifice and the metal surface was ∼10 mm. as listed in Table 1. The surface preparation of the sandblasting, large-grit, and acid-etching (SLA) disks was produced by sandblasting titanium with 100 μm Al2O3, followed by acid etching in HCl/H2SO4/H2O (1:1:100) at 100°C for 30 min. All roughened discs are then ultrasonically cleaned in acetone and ethanol for 20 min at each step, rinsed in deionized water, and then dried in an oven at 60°C.
SLA, sandblasting, large grit, and acid etching.
Surface roughness measurement
The Surfcorder SE-40G profilometer (Kosaka Laboratory, Tokyo, Japan) was used to measure the surface roughness (Ra; arithmetic mean roughness) with a cutoff value of 0.25 mm, a measurement length of 1 mm, and a drive speed of 0.1 mm/sec. The Ra data provided for each group were the mean of 11 independent measurements.
Estimation of contact angle
The static water contact angles were determined by the sessile drop method at room temperature (25°C, 65% relative humidity). Using a micropipette, a droplet (5 μL) of water was placed on the sample surface. The water contact angle, expressed as the mean ± standard deviation, was calculated from 11 measurements.
Surface morphology
A scanning electron microscope (SEM, JSM-6700F; JEOL, Tokyo, Japan) was used to characterize the surface morphology of the roughened specimens. Three specimens per group were coated with gold using a JFC-1600 (JEOL) coater and examined by SEM operating in the lower secondary electron image mode (LEI) at 3 kV accelerating voltage.
Bacterial adhesion
The bacterial adhesion of the specimens against Escherichia coli (ACTT, DH5α) was investigated as a model for gram-negative bacteria. Specimens were placed in 24-well culture plates and 1 mL of bacteria was seeded on the specimens at a density of 2 × 106 CFU/mL in Bacto Tryptic Soy Broth (Becton Dickinson, Sparks, MD) for 2, 4, 8, and 12 h. 13 Afterward, the adhesion of bacteria on specimens was assessed by alamarBlue (Invitrogen, Grand Island, NY, USA) assay that was used for real-time and repeated monitoring of bacterial viability. 14 At the end of the culture time, specimens were transferred to new plates and then washed twice with phosphate-buffered solution (PBS, pH 7.4). A total of 600 μL of the solution at a ratio of 1:100 of alamarBlue to fresh medium was added and incubated at 37°C for 20 min. The solution in each well was transferred to a new 96-well tissue culture plate. Plates were read in a Sunrise Microtiter reader (Tecan Austria Gesellschaft, Salzburg, Austria) at 570 nm with a reference wavelength of 600 nm. The absorbance results were obtained in 15 independent measurements.
To observe bacterial morphology on the specimen surface, three specimens per group were washed three times with PBS and fixed in 2% glutaraldehyde (Sigma, St. Louis, MO) for 1 h after 4 and 12 h of seeding. The specimens were then dehydrated using a graded ethanol series for 20 min at each concentration. The dried specimens were mounted on stubs, coated with gold layer, and viewed using SEM.
Cleaning processing
After 8 h of bacterial culture on the Grit, SB100, and SLA specimen surfaces, plastic curettage, air-powder abrasive system, Er:YAG laser debridement, as stated below, were further used to evaluate the cleaning effect. Fifteen replicates were carried out for each group. After the cleaning treatment, SEM observation (n = 3) and alamarBlue assay (n = 9), as previously stated, were used to evaluate the residue quantity of E. coli on the surfaces. In addition, the treated surfaces were also examined by SEM (n = 3) to understand whether the cleaning processing altered on the morphology of implant surfaces or not.
Plastic curettage
Samples were scaled from bottom to top with the plastic curette (Implacare™; Hu-Friedy, Chicago, IL), in which the tip was placed at a contact angle of 70. No attempt was made to standardize the application of the scaling force because the operator applied the curettes freely.
Air-powder abrasive system
The bacterial-adherent sample surfaces were treated with an air-powder abrasive system (AIR-FLOW Master®; EMS, Nyon, Switzerland). The device was used at a pressure of 5 bar. The insertion tip was perpendicularly applied to the surfaces and worked by directing fine particles of glycine (25 μm) that were propelled by compressed air at a distance of 10 mm from the surface for 1 min.
Er:YAG laser
Samples were irradiated with the Er:YAG (erbium-doped: yttrium, aluminum, and garnet) laser (KEY3; KaVo, Biberach, Germany) working at 2940 nm. A periodontal handpiece (No. 2056) was used with a prismatically cut glass tip. The fluency and repetition rate used for the laser irradiation was 100 mJ/pulse (12.7 J/cm2) and 10 Hz, respectively, and the pulse energy at the tip was ∼85 mJ/pulse. The tip was used at an incidence angle of 90. The application tip was moved from bottom to top and maintained in 2 mm with the disk surface for about 1 min per sample.
Statistical analysis
All the results are expressed as mean ± standard derivation for the numbers of experiments indicated, unless otherwise stated. One-way analysis of variance (ANOVA) was used to evaluate the significance of differences between the means. Scheffe's multiple comparison testing was used to determine the significance of the standard deviations between the measurements. Results were considered statistically significant when the p-value was less than 0.05.
Results
Roughness
When subjected to different pretreatments, the surface roughness (Ra) became 0.21 ± 0.03, 0.72 ± 0.05, 1.28 ± 0.09, and 2.68 ± 0.09 μm for No. 1200 grit polishing (Grit), 50 μm Al2O3 (SB50), 100 μm Al2O3 (SB100), and 250 μm Al2O3 sandblasting (SB250), respectively, while the SLA group was 1.96 ± 0.07 μm (Table 1).
Surface morphology of roughened substrates
The different surface morphologies of the Ti materials depended on the pretreatment methods (Fig. 1). In the case of SLA, there was the presence of etching-induced round-shaped grooves.
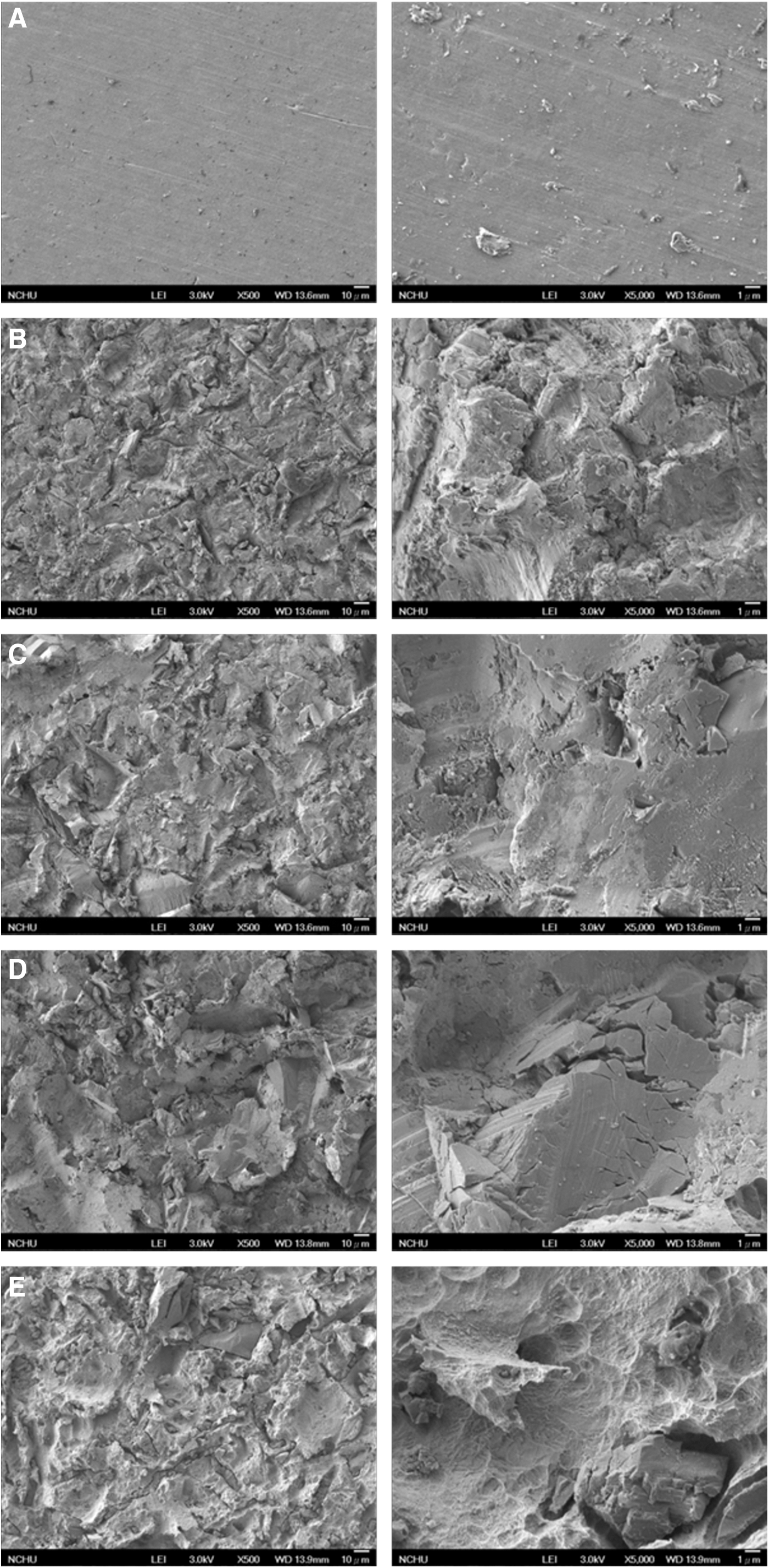
Surface topographies of Ti specimens roughened by
Contact angle
Figure 2 shows the contact angle images and corresponding average values of all group surfaces. The contact angle measured on the Grit group was around 58°. The average contact angles for SB50, SB100, and SB250 groups were 61°, 66°, and 73°, respectively, significantly being lower (p < 0.05) than that of SLA (101°).
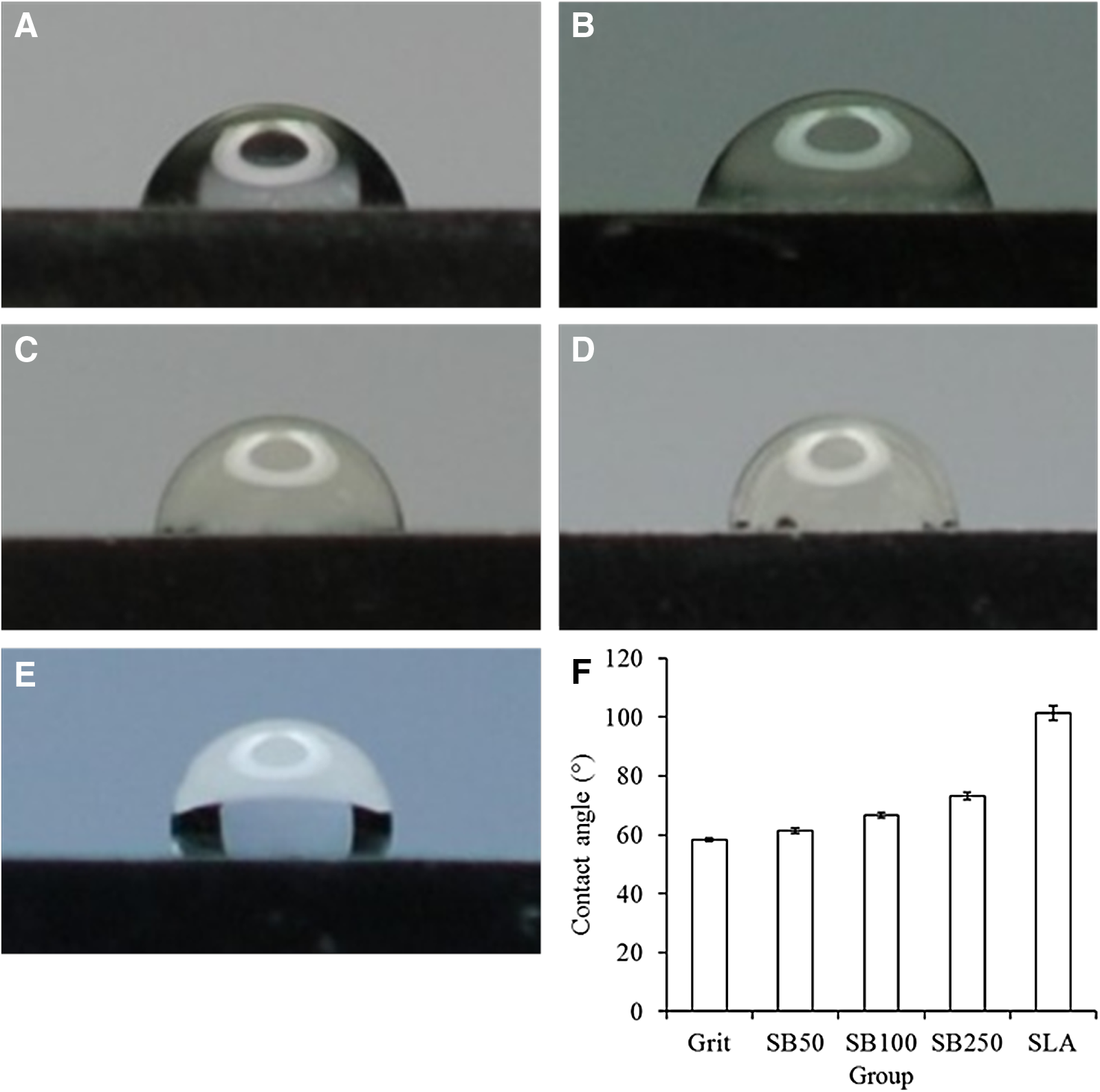
Water contact angle of Ti specimens roughened by
Roughness effect on bacterial adhesion
All groups exhibited an increased absorbance value with an increasing culture time (Fig. 3). No significant difference (p > 0.05) in bacterial adhesion was found among the groups at all culture time points, except the SB50 and SB250 groups at 12 h of culture. Similarly, scanning electron micrographs also indicated the increased amount of bacterial adhesion with the increase in culture time (Fig. 4).
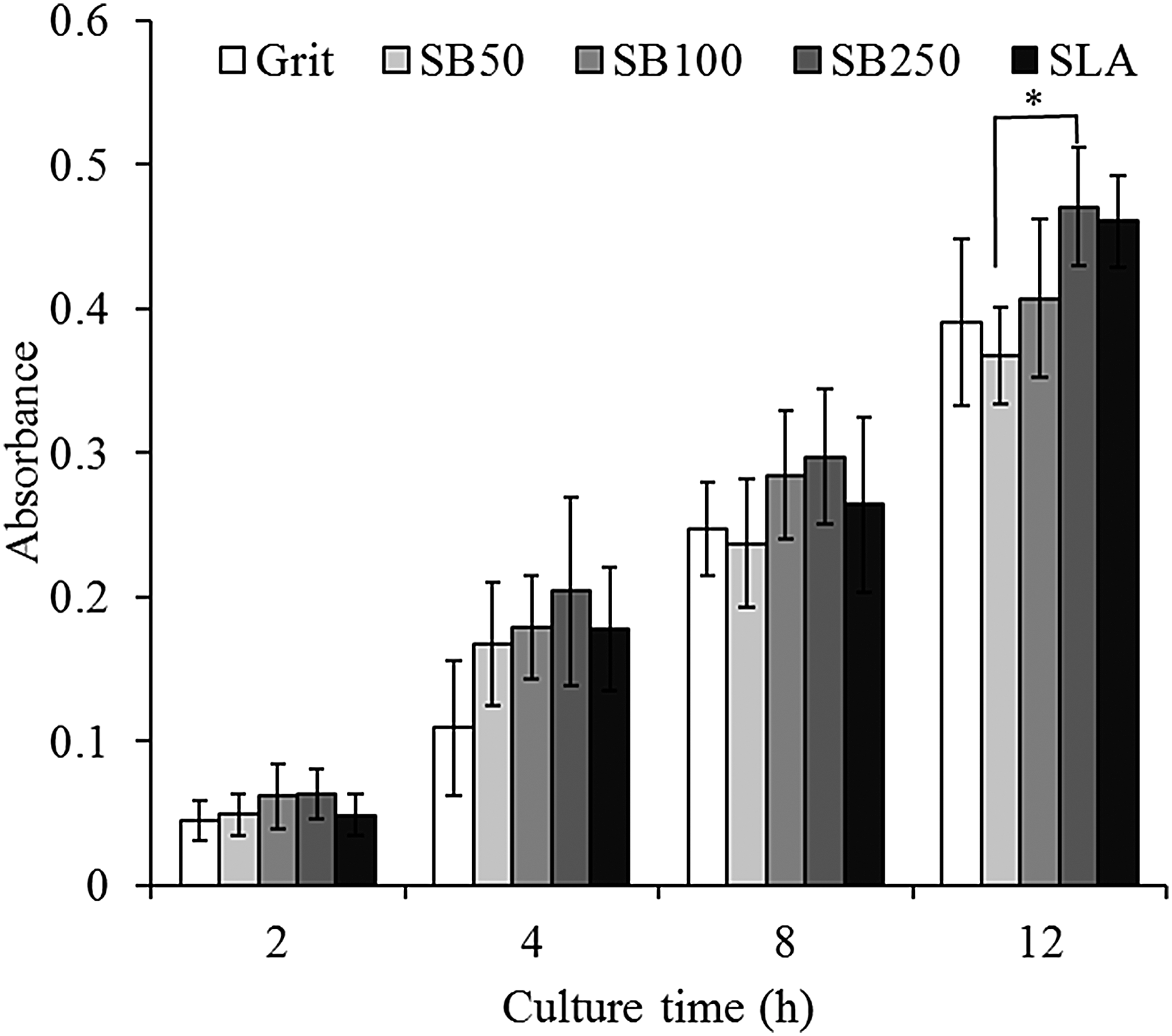
The amount of Escherichia coli adhesion on the five roughened surfaces after 2, 4, 8, and 12 h of culture. *Statistically significant difference (p < 0.05) between the two groups (n = 15).

Surface morphology of E. coli adhesion on
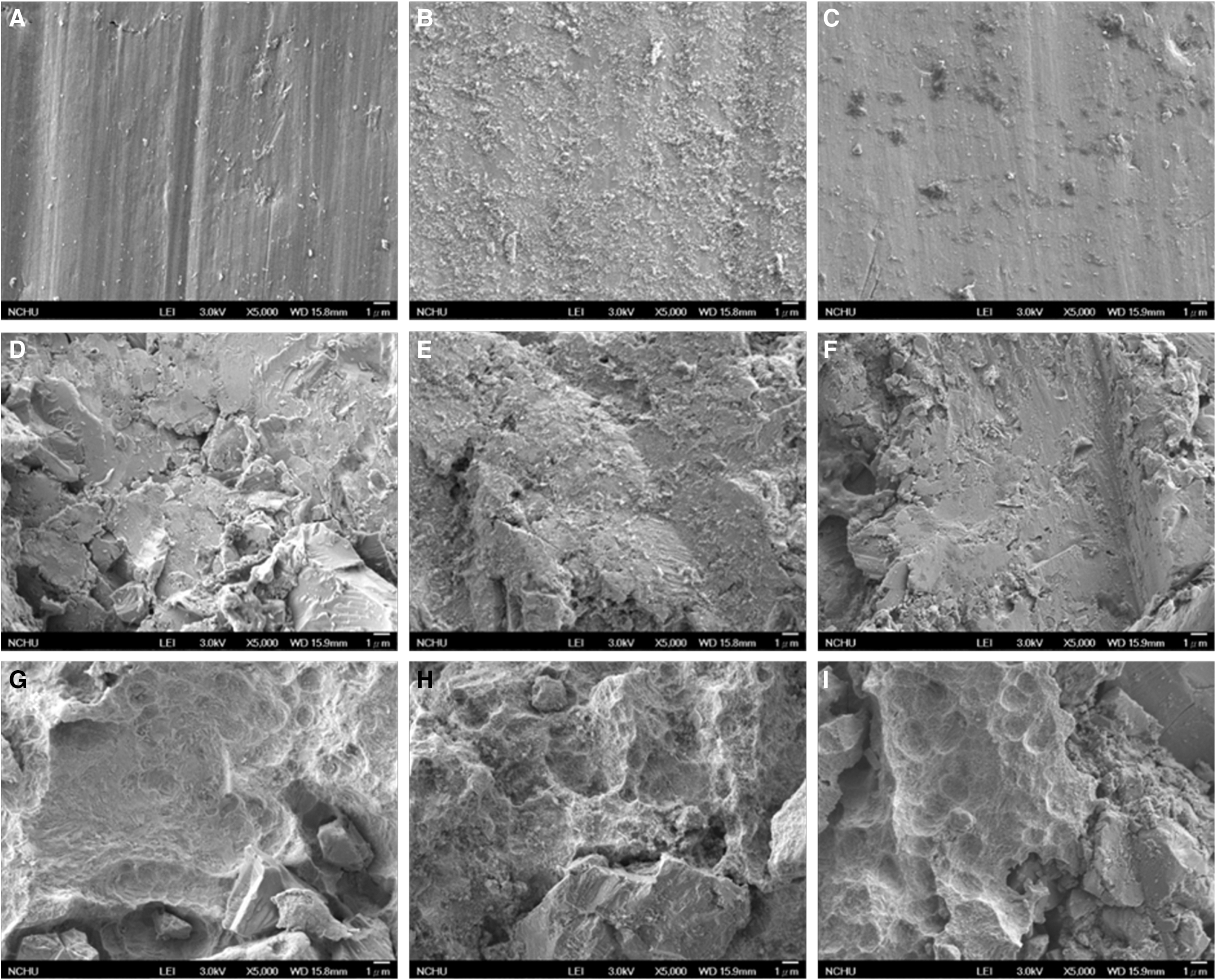
Cleaning effect
Figure 5 indicates that the three different cleaning treatments caused no damage to the morphology of the titanium surfaces. Compared with the controls, the plastic curettage reduced appreciably about 30% of E. coli adhesion. No statistically significant difference in bacterial quantity was noted among pretreatment surfaces (Fig. 6). In contrast, mostly E. coli was not found on implant cleaning, treated by air-powder abrasion and laser debridement. Consistently with Fig. 6, fewer E. coli strains (indicated by arrows) adhered on surfaces following treatment by air-powder abrasion and laser debridement, as shown in Fig. 7, compared with the control and plastic curettage groups.
Surface topographies of Ti specimens roughened by
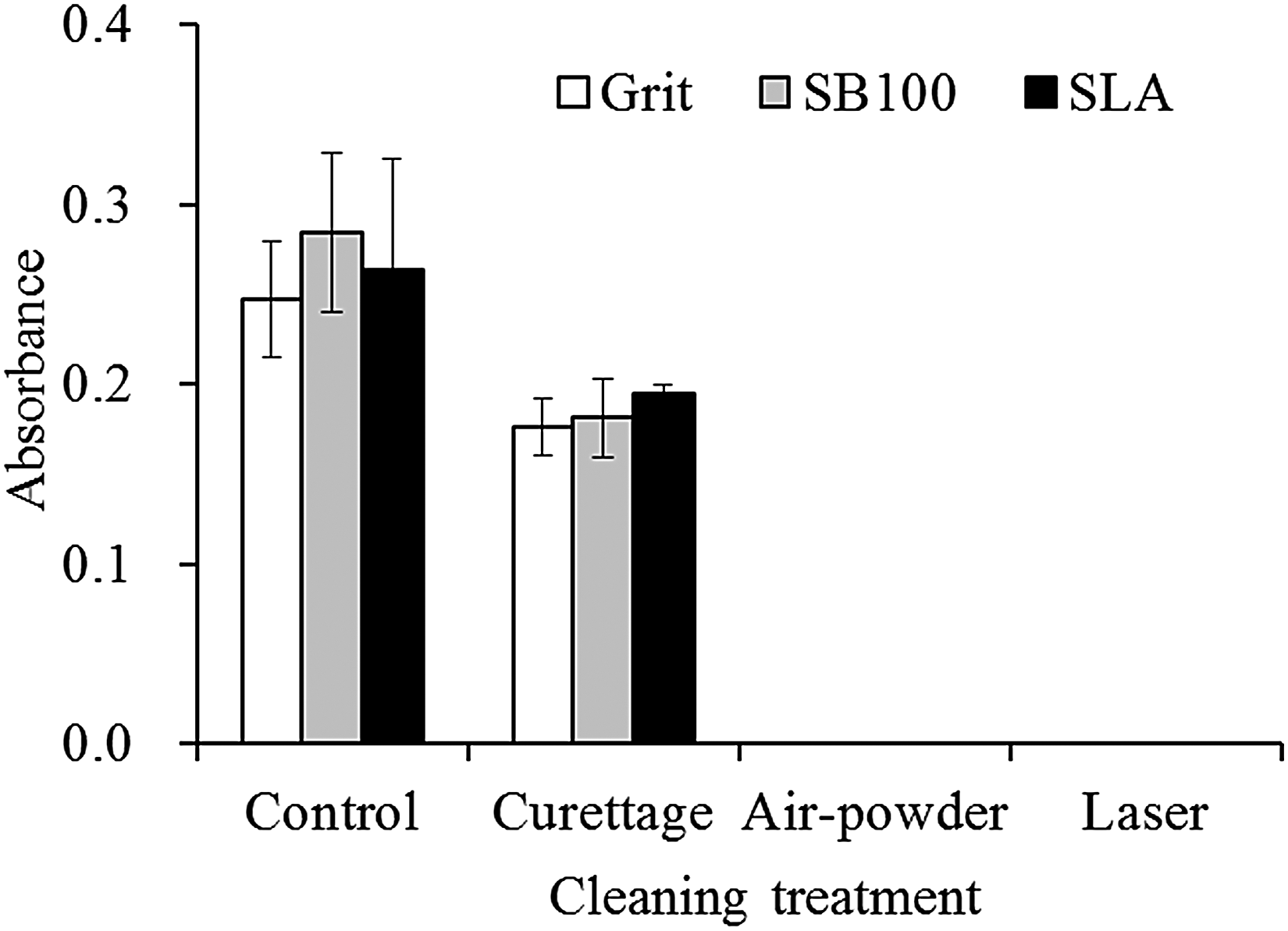
The amount of residual E. coli. on roughened Ti specimens after different cleaning treatments compared with the control without treatment (n = 9).

Scanning electron micrographs showing the effect of (
Discussion
Topographical modification of titanium implant surface has been documented as one of the most influential factors leading to enhanced osseointegration. 15 An average surface roughness of 3 μm is more suitable than 0.5 μm in favoring osteoblast differentiation in vitro. 16 Surface roughness also influences bacterial plaque accumulation. Bollen et al. suggested that an increase in surface roughness above a threshold roughness of 0.2 μm resulted in a simultaneous increase in plaque accumulation. 17 However, few studies focus on the commercially available dental implants that display a range of surface roughness (0.35–2.5 μm). 18 In the present study, the Ra value changed from the lower value of 0.2 μm for the Grit group to the significantly higher value of 2.7 μm for SB250 group, indicating a significant difference from the SLA group (2.0 μm). It is reasonable that the greater the Al2O3 sandblasting particles, the higher the Ra value obtained. The Ra value of the SLA implant was similar to a previous study, 19 which was identical to the dental implant surface currently used in clinical practice. It is worth noting that SLA had a significantly higher Ra value than SB100, although the two groups were pretreated by the same 100-μm-size Al2O3 particles. One of the possible factors that the acid etching may increase the Ra value is hydrogen desorption, which in turn results in an increase of the subsurface hydrogen concentration and the formation of a titanium hydride. 20 Cochis et al. also found an increased roughness because of the formation of craters on samples treated with SLA, 21 similar to the structure revealed in this study.
Although the surface roughness was changed by the different pretreatment methods, no significant difference in bacterial adhesion was found in most groups. This result concurred with the findings of Pier-Francesco et al., 18 which indicated no significant difference in percentage coverage of Porphyromonas gingivalis between “smooth” samples (Ra = 155 nm) and “very rough” samples (Ra = 449 nm). They postulated that the increased size of surface irregularities was too large to offer increased bacterial retention. In contrast, da Silva et al. reported that with the increase of the surface roughness ranging from 0.17 to 3.13 μm, an increase in S. sanguis bacterial adhesion was observed. 22 In our results, the bacterial viability on SB50 was significantly lower than on SB250 at hour 12, possibly because of the extended culture time and bacterial type.
Wettability is an important factor of concern when designing orthopedic and dental implants because they dominate the biological response (e.g., cell and bacteria adhesion). 13,23 The water contact angle of the implant surfaces gradually increased with the increased Al2O3 particle size used for sandblasting. This is because the entrapped air in the micropores leads to a heterogeneous surface, which cannot be spontaneously wetted. 24 As for SLA, Alfarsi et al. reported a high contact angle of about 130°, 19 confirming the hydrophobicity of the SLA sample.
Peri-implant prophylaxis should be performed one to four times per year continuously for several years. Until recently, the protocol for effective implant prophylaxis remains unclear and the evidence for maintenance therapy following such a protocol has not been proven. 25 In addition to prophylaxis, a more important prerequisite is to avoid alteration of the implant surface profile, because surface alterations occurring over time may give rise to increased plaque accumulation, which in turn adversely affects the peri-implant region. When assessing implant-cleaning instruments, the potential for damage as well as the cleaning efficacy must be evaluated. Among these cleaning methods, air-powder abrasive system and Er:YAG laser had good cleaning effects without disturbing the original titanium surface architecture. Cochis et al. found that air-power abrasion with glycine powder did not reveal any detrimental effect on the quality of the titanium surface. 21 In contrast, the plastic curettage produced an insignificant alteration of the titanium implant surface, but its efficacy of cleaning was limited.
Recent in vivo studies by Schwarz et al. 26 and Takasaki et al. 27 demonstrated that 10 or 20 Hz Er:YAG irradiation was safe and effective for surgical treatment of peri-implantitis in dogs. Er:YAG irradiation seems promising for clinical use in peri-implantitis treatment for removing bacterial plaque and calcified deposits from microstructured implant surfaces as well as removing granulation tissue from bone defects. Regarding the alteration of the microstructured titanium surface induced by irradiation, Schwarz et al. reported that Er:YAG irradiation (100 mJ/pulse, 10 Hz) induced no visible changes on various titanium surfaces. 28 Kreisler et al. demonstrated that Er:YAG irradiation (60 mJ/pulse, 10 Hz) ensured reliable removal of bacterial cytotoxic components from implant surfaces in vitro without altering the surface morphology of microstructured surfaces. 6 In our study, laser irradiation with the energy setting as 100 mJ/pulse and 10 Hz caused no visible damage to the titanium surfaces, possibly because titanium was too hard. Nevertheless, it seems to be difficult to achieve complete decontamination of a surface with laser irradiation, because few bacteria will always remain in valleys and undercuts as shown in current SEM images. However, removal of more than 96% of the biofilm would seem to be sufficient for clinical health. 29 This requirement was fulfilled by the laser irradiation and air-powder abrasive system.
Conclusions
The surface roughness did not affect appreciably bacterial adhesion. A comparison of the decontamination protocol indicated that significantly fewer E. coli remained on implant surface when the Er:YAG laser irradiation and air-powder abrasive system were used in comparison with the plastic curettages. Air-powder abrasion and laser debridement caused no visible damage to the implant surfaces.
Footnotes
Author Disclosure Statement
No competing financial interests exist.