
Abstract
Introduction
T
Calcium hydroxide (CH) has been widely used as an intracanal medicament owing to its antimicrobial properties against a vast majority of endodontically relevant pathogens. 3,4 However, Enterococcus faecalis, the most common bacterium in persistent infections, is known to withstand the antibacterial effect of CH. 5,6 Among several medicaments proposed as an alternative to CH, a triple antibiotic paste (TAP) containing metronidazole, ciprofloxacin, and minocycline has been utilized to disinfect the root canal during regenerative endodontic procedures. 6,7 In addition to its antibacterial effect against common endodontic pathogens, 6 TAP was shown to eradicate established biofilm of E. faecalis 8 and exert a residual antibacterial effect against E. faecalis for up to 2 weeks. 8
To maintain the sealing and bonding efficacy of permanent root filling or biomaterials, interim medicaments should be completely removed from the root canal system. 9 In general, the removal of intracanal medicaments is accomplished by a variety of irrigation regimens and techniques. 10,11 Laser-activated irrigation (LAI) using an erbium, chromium:yttrium–scandium–gallium–garnet (Er,Cr:YSGG) laser at a wavelength of 2780 nm was shown to be capable of removing the smear layer, 12 debris 13 and improving root canal disinfection 14 eliciting damage to surrounding tissues. 15 Ethylene diaminetetraacetic acid (EDTA) has been the most commonly used chelating agent with laser activation. Phytic acid (inositol hexaphosphate, IP6) is an alternative chelating agent whose biocompatibility and smear layer removal efficacy has been recently demonstrated. 16 Phytic acid solution can be extracted with low cost from rice bran 17 and has multiple negative charges, rendering it an effective chelator of multi-valent cations such as calcium, magnesium, and iron. 18,19 However, its potential on the removal of intracanal medicaments is unknown. Therefore, the aim of this in vitro study was to evaluate the efficacy of LAI of EDTA and phytic acid in the removal of CH and TAP from root dentin. The null hypothesis tested was that LAI would not affect the removal ability of EDTA and phytic acid to remove intracanal medicaments.
Materials and Methods
Specimen preparation
Eighty periodontally involved, freshly extracted, human maxillary anterior teeth with straight roots were used. The crowns were sectioned off below the cementoenamel junction so that the length of all roots was adjusted to ∼16 mm. The root canals were prepared using ProTaper rotary instruments (Dentsply-Maillefer, Ballaigues, Switzerland) up to master apical file F4 (size 40, taper 0.06) with 2 mL 5.25% sodium hypochlorite (NaOCl) between each file size. Prepared root canals were irrigated with 5 mL NaOCl, followed by 5 mL 17% EDTA, to remove the smear layer. The canals were subsequently dried with paper points.
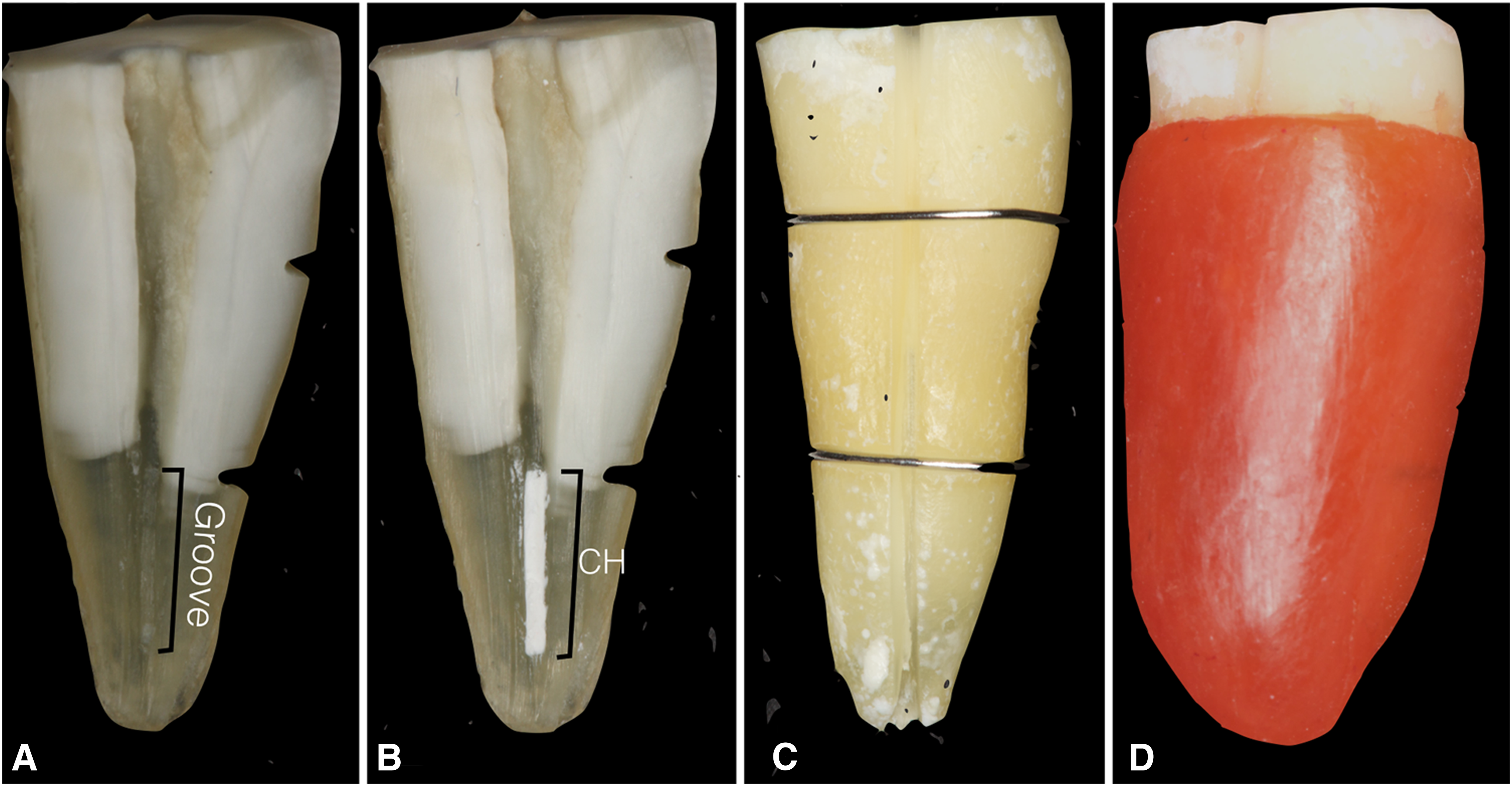
Longitudinal grooves were cut on the buccal and lingual root surfaces without damaging the inner layer of dentin around the canal. The roots were split longitudinally through the canal using a hammer and chisel, allowing subsequent reassembling. A groove was prepared 2–6 mm from the apex in one canal wall, 20 with standardized dimensions (4 mm length, 0.2 mm width, and 0.5 mm depth) (Fig. 1A) that are comparable with that of an apical oval root canal. 21
Representative images:
Following preparation of grooves, digital micrographs were taken perpendicularly under 1:1 magnification and transferred to an open-source image analysis program (ImageJ V.1.36 for Macintosh; National Institutes of Health, Bethesda, MD) to confirm dimensions, and make corrections, whenever necessary. A toothbrush was used to remove debris from the root halves and grooves, followed by a final flush of 5 mL 17% EDTA for 1 min and 5 mL 2.5% NaOCl for 1 min, respectively. The root canals were dried with paper points and divided randomly into two experimental groups (n = 40/group) with respect to the material used to fill the grooves: Group A, chemically pure Ca(OH)2 (Sultan Chemists, Inc., Englewood, NJ) mixed with saline (1:1.5 w/v) (Fig. 1B), and Group B, a mixture of ciprofloxacin, metronidazole, and minocycline at a 1:1:1 ratio ground into a powder mixed with sterile saline.
After filling the grooves with the aid of a spreader to ensure proper loading of the materials in grooves, the roots were carefully reassembled under an operating microscope and secured with wires (Fig. 1C) and sticky wax (Fig. 1D) and the apical foramen was also sealed with wax (Fig. 1D). The access cavities were temporarily sealed with a cotton pellet and Cavit (ESPE, Seefeld, Germany) by using a Heidemann spatula, after which the roots were stored at 37°C and 100% relative humidity. After 1 week of storage, the root canals were irrigated with 5 mL 2.5% NaOCl, and the specimens were further randomly assigned to four groups (n = 10/group) defined by the final irrigation solution (EDTA and phytic acid) and irrigation technique (needle irrigation and LAI) used for removal of the medicaments: Group 1: 5 mL 17% EDTA with syringe irrigation using a 27-gauge Monoject (Kendall; Covidien, Mansfield, MA) needle. The needle tip was placed ∼1 mm from the apex. The treatment time was 2 min. Group 2: Needle irrigation was performed as with group 1 using 1% phytic acid as the irrigant. Group 3: Irrigation with 17% EDTA for 15 sec, followed by LAI for 15 sec using Er,Cr:YSGG laser (Waterlase; Biolase Technology, Irvine, CA). The parameters are summarized in Table 1. The irrigant was not aspirated from the canal, thus laser irradiation was always performed within an irrigant-filled canal. The cycle was repeated four times. The total volume of irrigant was 5 mL, and total time of treatment was 2 min.
22
Group 4: LAI was performed as with group 4 using 1% phytic acid as the irrigant.
The root canals were dried with paper points and the root halves were coded to prevent identification of the experimental group. The roots were then separated for evaluation. The amount of remaining medicaments in the longitudinal groove of the coded and randomly distributed specimens was scored under a stereomicroscope (Wild M3B; Leica, Heerbrugg, Switzerland) at 40 × magnification by two calibrated endodontists using a scoring system described by van der Sluis et al.
23
: 0: Cavity is empty. 1: Less than half of the cavity is filled with the tested medicament. 2: More than half of the cavity is filled with the tested medicament. 3: Cavity is completely filled with the tested medicament.
Statistical analysis
SPSS V11.5 for Windows (SPSS, Inc., Chicago, IL) was used for statistical evaluation of the scores. The data were analyzed using the Kruskal–Wallis test, and post hoc comparisons were made with the Mann–Whitney U test (both p = 0.05).
Results
Figure 2 shows distribution of CH and TAP remnant scores after irrigation with tested techniques and irrigation solutions. Removal of intracanal medicaments was significantly affected by the type of irrigation technique (p < 0.05), but not by the type of irrigation solution (p > 0.05). For both EDTA and phytic acid, LAI was more efficient than needle irrigation in removing both CH and TAP (p < 0.05). Irrespective of the irrigation technique and solution, significantly less TAP remained in canals than CH (p = 0.0001). As for the type of final irrigation solution, roots irrigated with phytic acid showed lower, but not significantly different, removal scores (better removal efficiency) than those irrigated with EDTA (p > 0.05).
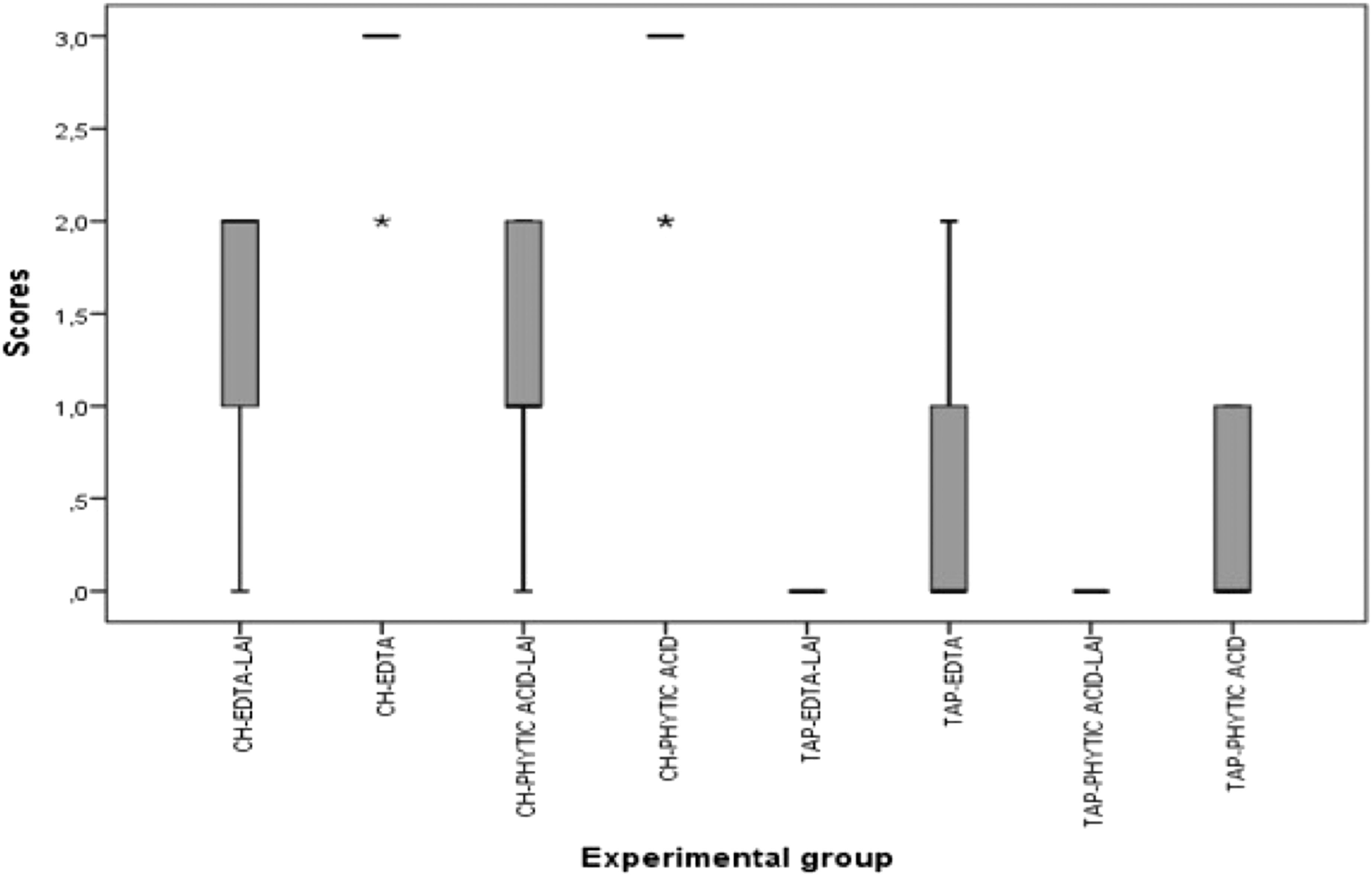
Box plots showing the distribution of scores for the removal of TAP and CH medicaments according to the experimental groups. Medians, interquartile ranges, and outliers are represented. *Outliers. EDTA, ethylene diaminetetraacetic acid; LAI, laser-activated irrigation; TAP, triple antibiotic paste.
Discussion
Because the presence of residual materials on dentin walls could compromise the adhesion, adaptation, and sealing efficacy of root canal sealers, interim medicaments should be completely removed from the root canal. 24 Various methods have been used to evaluate residual materials on root canal walls, including stereomicroscopy, scanning electron microscopy, computed tomography, and microcomputed tomography. 25 –27 In the present study, the remnants of the tested medicaments were evaluated under a stereomicroscope at 40 × magnification using a scoring method similar to that used in previous studies. 28 –30 The dentin groove model used herein was originally developed to simulate the uninstrumented root canal extensions as well as to standardize the root canal anatomy and amount of material present in the canal. 20 This test model provides a sensitive methodology and generates reproducible data. 23,25
Technically, if the two halves of the specimens are not in close proximity, there may be leakage along the crack line, resulting in altered irrigation dynamics compared with an intact root canal. Therefore, the use of this model might result in an overestimation of the reassembled halves with a leak-proof seal. To improve the quality of contact between the two parts of the reassembled tooth, the split roots were carefully reassembled under an operating microscope, secured tightly with wires from two levels, and sealed entirely with sticky wax that both prevents leakage and standardizes the dynamics of irrigation applied to all specimens. However, even under these conditions, it should be emphasized that the good, but less than perfect, adaption of the two pieces may have influenced the recorded results. The difference between localization of the groove and the tip of the needle from the root apex might explain why needle irrigation did not perform adequately, while revealing actual outcome of daily clinical practice.
Although the sequential use of NaOCl and EDTA has been recommended to achieve an adequate level of cleanliness on the root canal wall, 31 this combined irrigation regimen can lead to erosion of the dentin surface. 32 Exposure of root dentin to EDTA for extended periods might also decrease its modulus of elasticity and flexure strength, 33 leading to increased risk for root fracture. 34 Hence, the use of alternative chelator solutions with less or no detrimental effect on root dentin would be desirable. 35 Among several alternatives, phytic acid, a new naturally occurring chelating agent, was recently shown to effectively remove smear from instrumented root canals and flat coronal dentin surfaces, with better biocompatibility than EDTA on MC3T3-E1 cells. 16
In the present study, the medicament removal scores obtained after phytic acid treatment were statistically similar to those of EDTA-treated specimens. From a clinical point of view, this result might indicate that using a chelating solution that is capable of removing the intracanal medicament with minimal adverse effect on dentin would be advantageous. Based on the present data, phytic acid appears to be a suitable alternative to EDTA to remove the medicaments.
In the present study, none of the irrigation solutions were able to remove CH completely in needle or laser-assisted irrigation modes. This result confirms the findings of the recent study, demonstrating that neither needle irrigation nor LAI can remove the CH dressing completely. 36 The higher scores of CH may be explained by the small particle size and shape of CH that may allow direct penetration into open dentin tubules. 37 As for the TAP, Berkhoff et al. 9 reported that the irrigation techniques they had tested were not effective in removing the dressing from the root canal system. This result contradicts the current findings, which show that TAP was completely removed by both irrigation solutions and both irrigation techniques. Such differences could be explained by the method used by Berkhoff et al. 9 to remove the TAP as well as their utilization of the entire root canal instead of standardized apical grooves.
The effectiveness of root canal irrigation depends on both the mechanical flushing action and the chemical ability of a solution to dissolve tissue. 20,27 LAI is based on transmission of energy that results in producing transient cavitation in the liquid through optical breakdown. 38 One of the key findings of this study was complete removal of TAP in the LAI group. Moreover, LAI was statistically superior to needle irrigation in removing CH and TAP. Therefore, the null hypothesis that there is no difference between various techniques was rejected. This finding is in accordance with that of a previous study, 39 which also reported that LAI was more efficient in the removal of CH than needle irrigation, owing to its superior agitation potential. These results merit future comparisons with other irrigation techniques such as ultrasonically activated irrigation.
Conclusions
Within the limitations of this study, it can be concluded that the use of the laser-assisted irrigation facilitated removal of the medicaments from standardized grooves, while the type of irrigating solutions used as a final rinse did not play a significant role in removal of CH from dentin walls. Overall, CH was associated with significantly larger amounts of residue, whereas TAP was associated with less residue than CH with or without the use of laser-assisted irrigation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.