
Abstract
Introduction
I
Different irrigation solutions have been proposed for decreasing endodontic infection and sanitizing root canals. 4 Of these solutions, NaOCl is the most widely used irrigation agent due to its broad antibacterial spectrum and its capacity to dissolve organic remains of necrotic tissue. It can be used in varying concentrations of 0.5–5%. At low concentrations (0.5–1%), it dissolves mainly necrotic tissue, while at higher concentrations, its dissolving capacity and antibacterial properties increase, although its tissue-toxic effects also increase. 5 However, it will only penetrate into dentinal tubules to a depth of 130 μm, while infection by bacteria can penetrate up to 1.000 μm reaching the cementum–dentin junction. 6
In this scenario, the penetration capacity of laser therapies could reduce the number of endodontic treatment failures. 6 For this reason, therapeutic strategies, such as photodynamic therapy (PDT), are under investigation in endodontics because of their bactericide action both on permanent and deciduous teeth. 7 Photodynamic inactivation of microorganisms is based on the administration of a photosensitizer (PS) followed by low-dose irradiation with visible light of an adequate wavelength. 8
The use of a PS capable of absorbing light and initiating the formation of free radicals expands the range of PSs that can be used. 9 For this reason, the action of different PSs has been the subject of widespread research, particularly phenothiazine dyes, porphyrins and phthalocyanines. 10 Currently, methylene blue is the most widely used for bacterial management in endodontic treatment by PDT. 11,12
Chitosan has been extensively investigated in the biomedical field, 13 which has revealed its antimicrobial activity. 14 Various theories have been proposed to explain its antibacterial action, the most widely accepted hypothesis being its action on bacteria that facilitates the loss of their intercellular components. This involves a mechanism whereby positively charged chitosan attaches to the bacterial membrane provoking a change in the membrane's permeability, which causes the exit of its intercellular components, and so cell death. 15
The effects of chitosan on PDT have been assayed, using them directly as a PS 16,17 or as potential enhancers of some PSs, in vitro and in vivo 18 for the treatment of cancer and in vitro for the treatment of bacteria, using rose Bengal as a PS 19 or erythrosine. 20 However, the effect of chitosan on methylene blue as a PS for the in vivo treatment of Enterococcus faecalis is unknown.
The aims of this study were to evaluate the antibacterial efficacy of PDT and chitosan against E. faecalis and study the possible enhancive effects of chitosan on the PS methylene blue in experimentally infected root canals of extracted human teeth in vitro.
Materials and Methods
Preparation of teeth
The study was approved by the Ethics Committee of the University of Murcia (Spain). The model used in this study was a modification of that described by Haapasalo and Orstavik. 21 One hundred two extracted, intact, adult, human, single-rooted mature teeth with a single canal were collected and stored in sterile 0.5% NaOCl for 2–4 weeks. Calculus and stains were removed from the root surface using an ultrasonic scaler (Cavitron; Dentsply Ltd, Ballaigues, Switzerland). 22 The external surface of each tooth was cleaned with 10% povidone-iodine. After 5 min, the disinfectant was removed from the surface with isopropyl alcohol and the tooth was decoronated to facilitate access to the root, using a rotary diamond saw (Komet, Barcelona, Spain) at 700 rpm under water cooling.
For instrumentation of the root canals, a K-file number 10 file (Dentsply Maillefer, Ballaigues, Switzerland) was used to first calculate the working length (1 mm from the root apex). Then, the canals were treated with K-file numbers 15, 20, 25, or 30 depending on the width of the canal.
The coronal two-thirds were treated with Gates Glidden burs (Dentsply Maillefer) numbers 4, 3, and 2. Last, the apical third was treated with rotary files (Wave One®; Dentsply Maillefer) to the working length. Accompanying the action of each file or bur, the canals were irrigated abundantly with saline solution and when instrumentation had been completed, they were irrigated with ethylenediaminetetraacetic acid (17% EDTA) (Dentaflux®, Madrid, Spain) for 1 min to eliminate dentinal smear and then with 2.5% sodium hypochlorite (NaOCl) (Tecnoquim S.L., Murcia, Spain). Last, the root canals were dried with number 25 paper points (Dentsply Maillefer).
The tooth apices underwent retrograde sealing with resin-modified glass ionomer (Vitrebond®, 3M Espe, Madrid, Spain). The teeth were then stored in demethylated ethanol 70% (Tecnoquim S.L.) for 24 h and afterward autoclave processed at 121°C for 15 min. Afterward, the teeth were placed in vertical position on 96-well microtitration plates (Biolab® S.L, Madrid, Spain) filled with sterile Brain Heart Infusion (BHI) broth (Merck, Madrid, Spain) so that the root was covered. 23 Then, the samples were placed in an incubator (Selecta®, Madrid, Spain) at 37°C for 1 h.
Cultivation of E. faecalis and root canal inoculation
E. faecalis strain ATCC 29212 (American Cell Culture Collection) was cultivated in its pure form in 1 mL BHI (Merck) until it reached an optical turbidity of 1 McFarland standard, with a concentration of 3 × 108 cell/mL (quantified by spectrophotometry with a wave length of 600 nm and absorbance of 0.137 nm), and incubated at 37°C for 1 h.
An hour later, each of the 85 teeth (17 were used as a negative control group) was inoculated with 0.1 mL E. faecalis (at a concentration of 3 × 108 cell/mL), which were then incubated at 37°C for 48 h in a vertical position.
Testing procedures
After 48 h of incubation in the vertical position, the teeth were randomly divided into six experimental groups (17 teeth per group) according to postinstrumentation procedure. Randomization was performed using an online service (
In Group 1, the canals infected with E. faecalis were filled with 2.5% NaOCl (Tecnoquim S.L.) for 5 min, removed with sterile paper points, and irrigated with normal 0.85% saline solution. 23
In Group 2, the root canals underwent PDT. This was performed with a PDT illumination setup (Helbo® Photodynamic Systems GmbH & KG, Walldorf, Germany), with a wavelength of 660 nm and a power density of 100 mW. To perform the treatment, 100 μL of methylene blue at a concentration of 0.01% (mass per volume) was applied to the root canal. This was left in situ for 3 min. Subsequently, the root canal was exposed to laser light for 60 sec.
Group 3 root canals received topical applications of chitosan (low viscous, low molecular weight) (Sigma-Aldrich® Chemistry, S.A., Madrid, Spain) dissolved in acidified water with acetic acid 1% (Sigma-Aldrich Chemistry, S.A.), at a concentration of 3 mg/mL (concentration proposed by Shrestha and Kishen 19 for its antibacterial activity against E. faecalis and Pseudomonas aeruginosa). To administer the treatment, 100 μL of chitosan (3 mg/mL) was applied topically to each root canal with a sterile micropipette.
Group 4 root canals received the same PDT treatment as Group 2, but to study the possible enhancive effect of chitosan on the photosensitive methylene blue, immediately following topical application to root canals of 100 μL methylene blue, topical application of 100 μL of chitosan was added at a concentration of 3 mg/mL. Both applications (PS and chitosan) were left in situ for 3 min. Subsequently, the root canal was exposed to laser light for 60 sec.
Control groups consisted of Group 5 with no treatment (positive control) and Group 6 with no inoculation and no treatment of the bacterium (negative control).
Bacteriological evaluation
Following all treatments, canals were filled with normal 85% saline solution and samples were taken by the sequential use of three paper points (Dentsply Maillefer) inserted to the working length. The paper points were transferred to Eppendorf tubes containing 0.1 mL of normal 0.85% saline solution and centrifuged for 5 min at 10,000 rpm. in an Eppendorf centrifuge (Beckmann Coulter® S.A., Madrid, Spain).
Afterward, the paper points were carefully removed and the supernatant was eliminated from the Eppendorf tubes. Ten serial dilutions were placed (100 μL) in triplicate on the surface of blood agar plates (Scharlau® S.L., Barcelona, Spain) and incubated at 37°C for 48 h. The number of colonies was counted at the appropriate dilution and the number of colony-forming units (CFU)/mL was calculated. 24
Scanning electron microscope analysis
Five teeth from each group were analyzed. The teeth were fixed in a buffered formalin solution for 1 week and dehydrated by immersion in ethanol solutions (70%, 95%, and 100%). Longitudinal grooves were made carefully along the entire length of each root with a metallic water-refrigerated disk (Komet).
The teeth underwent metallographic preparation for analysis under a scanning electron microscope (SEM) (Oxford Instruments INCA 300 EDX System, Abingdon, Oxford shire, United Kingdom). Initially, the specimens were analyzed by navigation at different magnifications. Two SEM micrographs were obtained from each third. The root canal was measured and the central part of each middle third was evaluated. The SEM images were obtained at 1600 and 5000 magnifications. Images were then analyzed to identify the presence or absence of contamination and debris on the root canal surface 4 using MIP-4® histomorphometry software (Digital Image, Barcelona, Spain), calculating the percentage of area with contamination and debris in relation to the total area under examination.
Statistical analysis
Data were analyzed using the SPSS version 20.0 statistical package (SPSS®, Inc., Chicago, IL). A descriptive study was made of each variable. Analysis of variance and the Tukey test were applied to quantitative variables, in each case determining whether variances were homogeneous. Statistical significance was established as p < 0.05.
Results
The E. faecalis count in root canals (expressed as log10 CFU/mL) was zero in the negative control group. The positive control group showed a greater number of CFU/mL (6.01 ± 0.84 log10 CFU/mL), with statistically significant differences in comparison with the other treatment groups (p ≤ 0.05). The treatment group showing the lowest CFU count was the combined PDT+Chitosan 3 mg/mL (3.77 ± 1.47 log10 CFU/mL), followed by the PDT-alone group (3.81 ± 1.46 log10 CFU/mL), which obtained similar results to the results for applications of 2.5% NaOCl (3.87 ± 1.88 log10 CFU/mL) (Table 1).
Groups marked by different superscript letters showed significant differences.
CFU, colony-forming units; PDT, photodynamic therapy; SD, standard deviation.
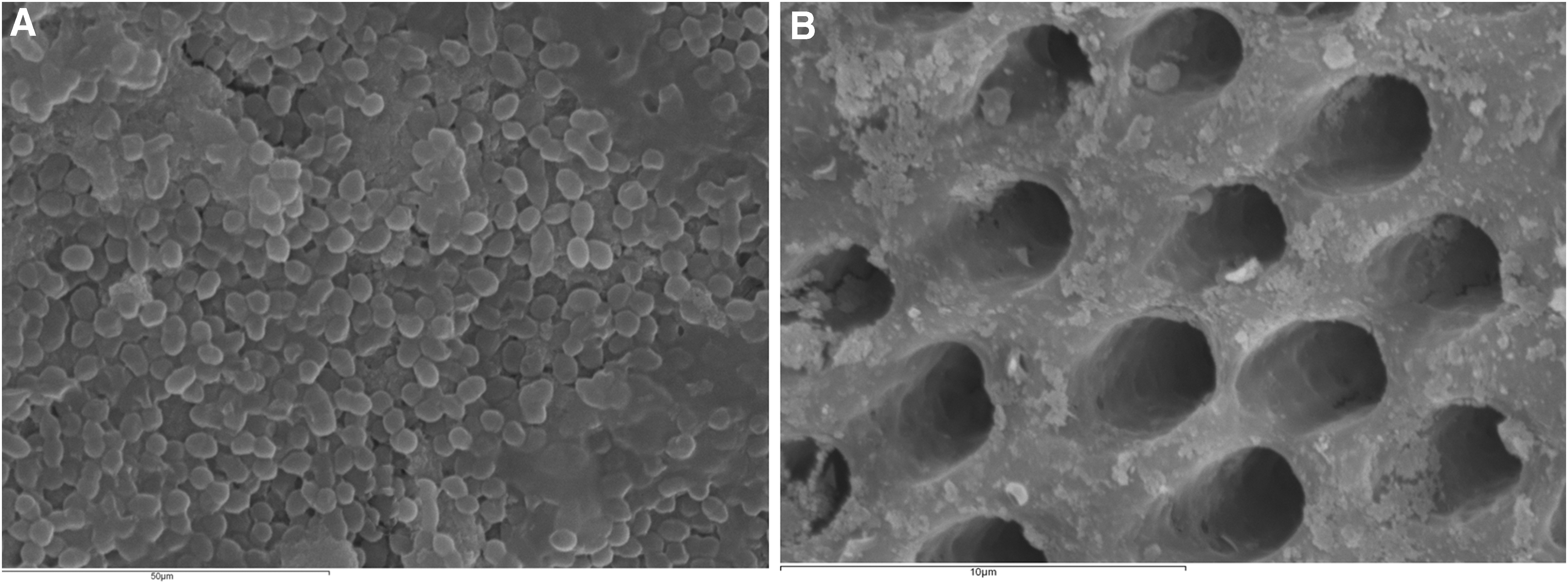
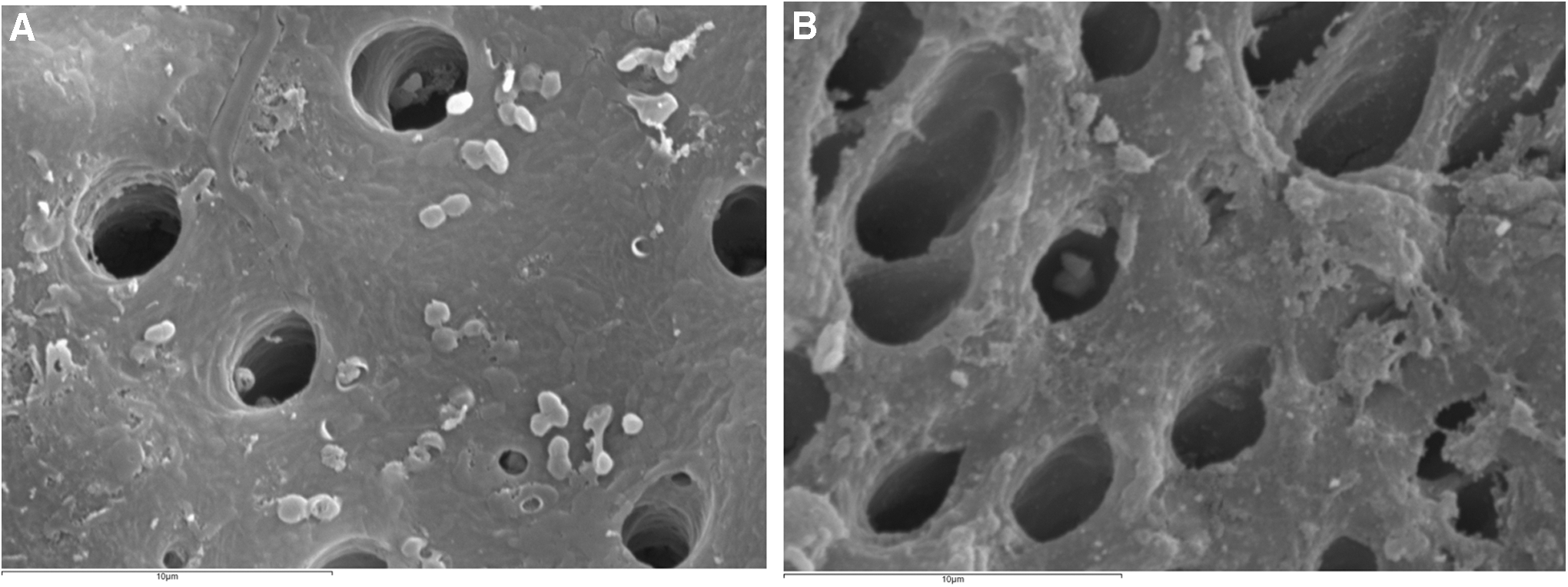
Comparing the percentage of area with contamination and debris in relation to the total area under study (coronal+middle+apical), a higher percentage was obtained in the positive control group (25.14% ± 6.09%) (Table 2) (Fig. 1A), while the combined PDT+Chitosan 3 mg/mL group showed the lowest contaminated area percentage (19.39% ± 7.99%) (Fig. 1B), followed by the 2.5% NaOCl group (22.19% ± 4.41%) (Fig. 2A), which obtained similar results to PDT alone (23.07% ± 7.49%) (Fig. 2B). Nevertheless, no statistically significant differences were found between any of the treatment groups.
Groups marked by different superscript letters showed significant differences.
SD, standard deviation.
Discussion
E. faecalis is a gram-positive facultative anaerobic coccus that has been identified as a frequent cause of treatment failure in root canal therapy. 25 It has a high capacity for survival due to its ability to form biofilm, its resistant cytoplasmic membrane rich in glycerol, its capacity for survival over long periods of limited nutrition, its ability to maintain its pH level due to the blocking capacity of the cytoplasm, and its capacity to adhere strongly to the dentinal tubule through the production of angiotensin-converting enzyme (which promotes union) and serine protease. 3
For this reason, its prevalence is higher in persistent infections than in primary infections. 1 Despite instrumentation, irrigation, and intracanal medication, the bacteria can survive in the dentinal tubules as a persistent infection, 6 although in vitro trials of antibacterial endodontic treatments have used a variety of microorganisms such as Actinomyces Israelii, 26 Fusobacterium nucleatum, 27 Porphyromonas gingivalis, 12 Prevotella intermedia, and Peptostreptococcus anaerobius 27 among others. In this study, bacterial inoculation was performed at a concentration of 3 × 108 cell/mL, as used by other researchers such as Estrela et al., 4 slightly stronger than that used by Fimple et al., 12 (2.5 × 108 cell/mL). In the light of the results obtained by the positive control group, this concentration was seen to be effective and achieved satisfactory experimental in vitro root infection.
NaOCl is currently the most widely used irrigation agent due to its wide antibacterial spectrum and its capacity to dissolve organic debris and necrotic tissue. 28 In this study, the application of 2.5% NaOCl reduced the E. faecalis count in root canals with statistically significant difference compared to the positive control group. However, E. faecalis is able to survive for long periods without nutrients and invades dentinal tubules to depths over 300 μm, 6 characteristics that protect it against the usual irrigating agents.
In this scenario, the penetration capacity of laser therapies could reduce the number of endodontic treatment failures, and for this reason, PDT has been adapted for endodontic disinfection; its efficacy with PSs has been evaluated in various studies. 29 In this study, the teeth treated with PDT using methylene blue as PS showed a high reduction in the CFU/mL, obtaining a lower mean value than samples treated with 2.5% NaOCl. SEM analysis obtained area percentages occupied by contaminants and debris that were very similar for teeth treated by PDT and treated by 2.5% NaOCl.
In the same way, Fimple et al., 12 investigated the photodynamic effects of methylene blue on multispecies root canal biofilms, and they achieved up to 80% reduction of CFU/mL and concluded that PDT can be an effective adjunct to standard antimicrobial treatment. Xhevdet et al., 30 also using methylene blue as PS, and using the same irradiation laser as this study (Helbo Photodynamic Systems GmbH & KG) on in vitro extracted human teeth infected with the same strain of E. faecalis used in this study (ATCC 29212), obtained a slight reduction in CFU/mL compared with teeth treated with 2.5% NaOCl. Nevertheless, the fact remains that PDT fails to bring about a 100% reduction in microbial cells. 31
New PS substances such as curcumin and others have been assayed in the hope of boosting the effect of PDT on root infection by E. faecalis. 32 Chitosan, a natural polysaccharide, has been seen to have antimicrobial activity and derivates against fungi, bacteria, and viruses. 14,33 The combination of PSs with chitosan could further improve the antibiofilm efficacy of PDT. 34 The effects of chitosan have also been assessed as potential enhancers of some PSs, in vitro for treating bacteria. Shrestha and Kishen 19 studied the possible enhancing effects of chitosan on rose Bengal PS in PDT treatment of E. faecalis and Pseudomonas aeruginosa biofilms, comparing the effects of chitosan with rose Bengal alone and methylene blue alone.
Photoactivation resulted in significantly higher elimination of both bacterial biofilms sensitized with chitosan+rose Bengal than rose Bengal alone and methylene blue alone. Chen et al., 20 studied the possible potentiating effect of chitosan on the PS erythrosine in PDT treatment of Streptococcus mutans, P. aeruginosa, and Candida albicans biofilms, finding that the antimicrobial activity of PDT was greater when erythrosine was combined with chitosan than when erythrosine was used alone. These results showed that the group of teeth treated with PDT+chitosan obtained greater reductions in CFU/mL, while the SEM observation found lower percentages of area occupied by contaminants and debris.
However, several investigations should be performed before its clinical recommendations (combination of PDT+chitosan 3 mg/mL). Some questions involving the physical and chemical characteristics, the ideal concentration for effective antibacterial power, adverse effects, and tissue tolerance must be answered. In this sense, further in vivo studies are needed to determine chitosan's effect on methylene blue as a PS for the PDT treatment of E. faecalis. In this sense, an intrinsic limitation of this study must be considered.
In groups 3 and 4, in which we used chitosan (3 mg/mL) alone or combined with PDT, this natural polysaccharide has been dissolved in acidified water with acetic acid 1% and not in deionized water (under constant magnetic stirring) as other authors. 19 To know if the acidified water itself is bactericidal, in next similar studies, a group with acidified water alone should be included.
Conclusions
In conclusion, in our study with 17 teeth per group, combining PDT and chitosan showed the greatest reduction of endodontic infection by E. faecalis compared to PDT alone or NaOCl. However, further in vivo studies are needed to determine chitosan's effect on methylene blue as a PS for the PDT treatment of E. faecalis.
Footnotes
Acknowledgments
We would like to thank to Professors Salinas J and Gallego MC (Department of Animal Health, University of Murcia, Murcia, Spain) for their help in handling with Enterococcus faecalis.
Author Disclosure Statement
No competing financial interests exist.