
Abstract
Introduction
T
Photobiomodulation (PBM) is a description of interventions with light therapy that modulate biological processes. Low-level laser therapy (LLLT) is a subtype of PBM where red and infrared light is generated by lasers. 5 LLLT is primarily offered as an “add-on” therapy to exercise in tendinopathy treatment, due to the proposed anti-inflammatory and stimulatory effect of laser irradiation on tendon healing. 6 Evidence of a positive interaction between LLLT and exercise has been increasing, as systematic reviews have reported accelerated recovery rates and pain reduction in Achilles, 7 lateral elbow, 8 and shoulder tendinopathy. 9 However, the effect of LLLT, almost without exception, appears to be dependent on the use of optimal laser doses, 7 –10 as recommended by the World Association for Laser Therapy. 11 Most LLLT research on tendinopathy has explored issues related to dose–response patterns, possible therapeutic mechanisms, and clinical effects. Thus, less research has focused on potential treatment interactions that might either enhance or decrease the effect of laser therapy. It was recently discovered that parallel use of the cortisol antagonist mifepristone completely blocked the anti-inflammatory effects of laser therapy. 12 For this reason, we were intrigued by a finding in our latest LLLT review on shoulder tendinopathy, 9 in which the result of a high-quality trial performed with optimal laser doses 13 might have been negatively influenced by parallel cryotherapy treatment.
The use of cryotherapy for tendon disorders is widespread, particularly in the early phases of acute injuries. 14 However, there seems to be a lack of evidence for the therapeutic mechanisms, 15 dosages, 16 and clinical effects on soft-tissue lesions. 17 It has been suggested that cooling acute tendon injuries reduces blood flow by vasoconstriction and slows down the metabolic rate of the tendon. Therefore, cooling may be helpful in controlling inflammatory reactions and preventing excessive edema. 18 In addition, the suppressive action of cryotherapy on neutrophil activity has been demonstrated in rat muscles. 19 Attenuation of this inflammatory reaction may reduce secondary tissue damage after acute injury. 20 These cells also initiate the repair process, which illustrates the importance of balancing anti-inflammatory treatments and stimulatory repair. 21
Achieving this therapeutic balance of limiting inflammation while simultaneously allowing and stimulating tendon repair seems to be the advantage of using LLLT compared with anti-inflammatory drug therapies. 22,23 The therapeutic mechanisms by which LLLT reduces inflammation are similar to the actions of nonsteroidal anti-inflammatory drugs (NSAIDs) and steroidal pharmaceuticals, as the cyclooxygenase-2 inflammatory pathway and the formation of prostaglandin E2 (PGE2) are inhibited. 24 LLLT has also demonstrated beneficial dose-dependent effects on the subsequent tendon repair process, predominantly by increasing fibroblast metabolism and collagen turnover. 25 In addition, it has been reported that the down-regulation of catabolic metalloproteinase enzymes observed after laser treatment significantly increased the biomechanical properties of tendons compared with NSAIDs. 22
Thus far, no studies have investigated the potential interaction of cryotherapy on LLLT. Therefore, the aim of this study was to compare the monotherapeutic effects of LLLT and cryotherapy with different combinations of the two modalities (LLLT first/cryotherapy and cryotherapy first/LLLT) on tendon mechanical properties and inflammation.
Materials and Methods
Animal model of standardized tendon trauma
Thirty-six male Wistar rats weighing 200–250 g, with food and water provided ad libitum, were used in this study. The Biotery of the Institute of Biomedical Sciences, University of São Paulo supplied the animals, which were randomly divided into six groups of six rats. The policies and procedures of the animal laboratory are in accordance with Brazilian laws and with those detailed by the U.S. Department of Health and Human Services. The experimental protocol was submitted and approved by the University of São Paulo Animal Research and Care Committee (No. 144/78-2).
After they were anesthetized with ketamine/xylazine (100 and 20 mg/kg, respectively), the rats were individually positioned with the right hindlimb and knee extended and the ankle in 90° dorsiflexion. Then, a mini-guillotine consisting of a block weighing 200 g, with a 2 mm wide blunt edge, was dropped from 20 cm, with guided support, to induce injury to the Achilles tendon. Previous studies have shown that the mini-guillotine model produces acute inflammation and degradation of tendon collagen. 26,27 After 24 h, the animals were euthanized with an overdose of halothane for biomechanical, histological, and biochemical analyses. After the removal of skin and connective tissue, the Achilles tendon was removed and processed for further analysis.
Experimental groups
The 36 rats were randomly divided into six experimental groups of six rats each, as follows: 1. Control group (CG): Animals did not undergo any type of procedure. 2. Injured nontreated group (ING): Animals underwent tendon trauma and received no treatment. 3. LLLT group (LG): Animals underwent tendon trauma and LLLT treatment 1 h after injury. 4. Cryotherapy group (CTG): Animals underwent tendon trauma and 20 min of cryotherapy treatment 1 h after injury. 5. LLLT first/cryotherapy group (LCG): Animals underwent tendon trauma and LLLT treatment followed by 20 min of cryotherapy 1 h after injury. 6. Cryotherapy first/LLLT group (CLG): Animals underwent tendon trauma and 20 min of cryotherapy followed by LLLT treatment 1 h after injury.
Treatments
All treatments were performed 1 h after administering the tendon trauma.
Low-level laser therapy
A single LLLT application was performed 1 h after controlled tendon trauma with an infrared laser unit (DMC®, São Carlos, Brazil). The laser unit emitted a continuous optical output of 100 mW with a wavelength of 810 nm to a spot size area of 0.028 cm2, providing a power density of 3.57 W/cm2. Optical power was calibrated using a Thorlabs power meter (Thorlabs Instruments, Newton, NJ). The optical power output of the laser unit was measured before, halfway through, and after the experiment. Laser irradiation was performed with skin contact in the middle portion of the Achilles tendon. The laser delivered an energy of 3 J in one single point, corresponding to an irradiation time of 30 sec. Energy density was 107.14 J/cm2 (Table 1). The laser treatment parameters were chosen according to previous studies performed by our research group. 24,28
The laser was held stationary in skin contact, targeting the middle portion of the Achilles tendon (area of pathology).
Cryotherapy
The animals’ injured Achilles tendons were treated for 20 min with small rubber bags containing 10 g of crushed ice. The ice came from a freezer, which held a stable temperature of −20°C. The rubber bags were fixed at the region of the Achilles tendon with rubber bands, and the hindlimb was kept elevated. Thermography recordings (ThermaCAM S65HS; Flir System, Boston, MA) before cooling showed a minimum Achilles skin temperature at 28.8°C (SD ±0.5). Skin temperature was 17.1°C (SD ±1.0) after 3 min and 19.2°C (SD ±0.4) after 10 min of cryotherapy (see supplementary Fig. S1 at
Analyses
A sample of six animals was used for all of the analyses, all of which were performed by one observer. The initial analyses were performed at the University of São Paulo. To ensure consistency of the analyses and reproducibility of the histology and cytokine results, a second laboratory, at the University of Mogi das Cruzes (Mogi das Cruzes, São Paulo, Brazil), duplicated the blinded analyses.
Histological analysis
The tendon tissue samples were fixed in a 10% formalin solution (Formaldeído PA; Synth, Diadema, São Paulo, Brazil) for 72 h. The samples were then dehydrated in a series of alcohol baths (Alcohol PA; Synth), beginning with 50% and progressing to 100%. The samples were cleared in xylol (Xilol PA; Synth) for 4 h and embedded in Paraplast® (Tyco, Mansfield, MA) for 4 h for impregnation. Slices that were 5 μm in thickness were cut, stained with hematoxylin and eosin, and mounted on glass slides. The specimens were photographed using a microphotographic camera (Dino-Eye AM-423X model; Dino-Lite Digital Microscope®, São Paulo, Brazil) connected to a personal computer. Standardized photos were taken of all groups at a magnification of 100 × at specimen level.
Cytokine analysis
Cytokine generation was analyzed, and interleukin (IL)-1β, IL-6, IL-10, and tumor necrosis factor-α (TNF-α) levels in the tendon samples were determined by an enzyme-linked immunosorbent assay (R&D Systems, Minneapolis, MN) according to the manufacturer's instructions. For this purpose, 96-well plates (R&D Systems) were coated with 100 μL of monoclonal antibody for each cytokine (anti-IL-1β, IL-6, and IL-10) and diluted in sodium carbonate buffer (Sigma-Aldrich, São Paulo, Brazil) (0.1 M, pH 9.6); anti TNF-α was diluted in sodium phosphate buffer (0.2 M, pH 6.5). The plates were incubated (4°C) for 18 h. For blocking, the plates were washed four times with phosphate-buffered saline containing 0.05% Tween 20 (PBST), then filled with 300 L/well of blocking solution (3% gelatin in PBST; Sigma, St. Louis, MO) at 37°C for 3 h, and subjected to a new cycle of washes. Next, 100 μL of properly diluted samples or standards of recombinant cytokines was added to the plate and left for 18 h at 4°C. After washing, 100 μL of the respective biotinylated antibodies for the specific detection of each cytokine was added and left for 1 h at room temperature. After the plates were washed, 100 μL of streptavidin peroxidase was added and left for 1 h at room temperature (22°C), followed by further washing. The reaction was revealed by adding 100 μL/well solution of 3,3′,5,5-tetramethylbenzidine and stopped by adding 50 μL/well of sulfuric acid (2 M). Readings were performed in a Spectrum Max Plus 384 spectrophotometer (Molecular Devices Corporation, Sunnyvale, CA) at a wavelength of 450 nm, with correction at 570 nm. Sample concentrations were calculated from standard curves obtained from the recombinant cytokines.
Biomechanical testing
A universal tensile test machine (zL2.5; Zwick Roell, Ulm, Germany) was used to perform mechanical testing of the tendons. Testing was performed immediately after tendon removal to avoid the influence of incubation. 29 The mechanical characteristics were extracted from the force-displacement curves obtained from cyclic loading at a constant velocity of 1 mm/min for each tendon. 22 At each cycle, tendon displacement was increased by 10% and force was released until 0.1 N was reached. The sequence was repeated until complete tendon failure was achieved.
Statistical analysis
The Kolmogorov–Smirnov test was applied to assess normality of distribution of the dependent variables. The Kruskal–Wallis test, followed by pairwise comparisons using the Mann–Whitney U test, was used to test for differences between the ING and the four treatment groups (LG, CTG, LCG, and CLG). The healthy noninjured CG was compared with the ING to validate the trauma model. Biomechanical data and cytokine concentrations are expressed as medians and interquartile range. Differences were considered statistically significant at p < 0.05. Tendon specimens were evaluated qualitatively for differences in collagen organization, tenocyte infiltration, and degree of eosin staining. To increase readability, the findings are presented quantitatively in a four-point histology score table and the mean score for each group is reported.
Results
Tendon mechanical properties
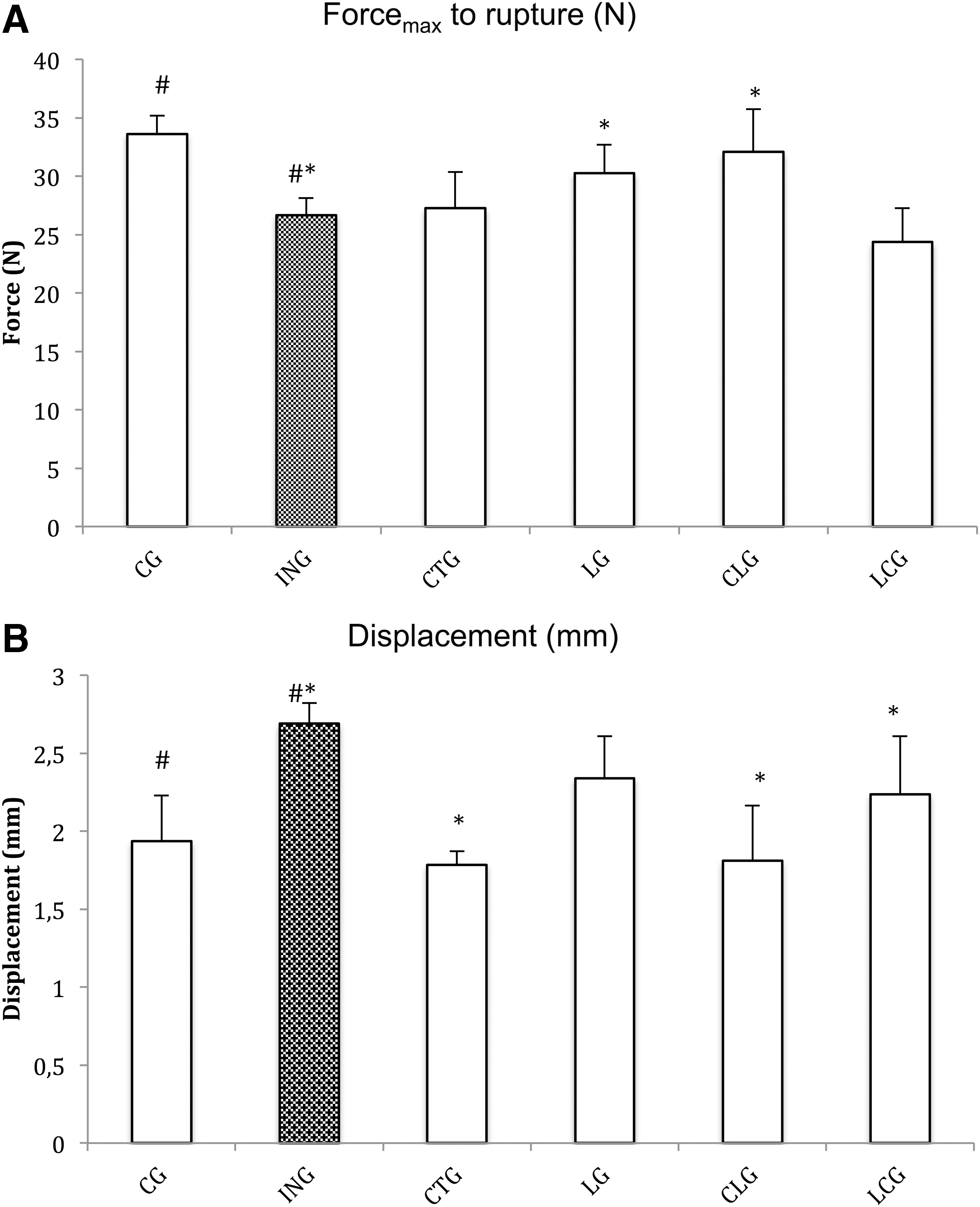
The Kruskal–Wallis test revealed a statistically significant difference in force (N) and displacement (mm) across the ING and the four different treatment groups, at X 2(4) = 5.3, p = 0.02 and X 2(4) = 5.3, p = 0.02, respectively. The CLG recorded the highest force (Md = 32.1 N) and the LCG recorded the lowest force (Md = 24.3 N) at the rupture point. The CTG and CLG recorded equally low displacement levels (Md = 1.8 mm), whereas the highest displacement rate was found in the ING (Md = 2.7 mm). Results from the pairwise Mann–Whitney U statistical test on force and displacement are summarized in Table 2. Between-group differences in force (N) and displacement (mm) at tendon failure are illustrated in Fig. 1A and B.
Measurements of
Mean rank in each group and significance level for each comparison are shown.
CG, control group; CLG, cryotherapy first/LLLT group; CTG, cryotherapy group; ING, injured nontreated group; LCG, LLLT first/cryotherapy group; LG, LLLT group.
Trauma model (comparison against healthy CG)
A comparison of the healthy controls to the ING tendons showed a significantly decreased force (p = 0.02) and increased displacement (p = 0.02) after tendinopathy by blunt trauma (i.e., inferior biomechanical properties were found for the injured tendons compared with the healthy tendons).
Monotherapies (comparison against ING)
Tendons treated with LLLT tolerated higher forces (p = 0.04), but they were not significantly less displaced than the nontreated tendons (p = 0.19). Tendons treated with cryotherapy were significantly less displaced (p = 0.02), but they did not tolerate higher forces at the rupture point than the nontreated tendons (p = 0.56).
Adjunctive therapies (comparison against ING)
The CLG displayed improved force (p = 0.02) and displacement rates (p = 0.04) compared with the nontreated group. The LCG showed significantly lower displacement (p = 0.04), but there was no effect on force (p = 0.15), compared with the nontreated group.
Biochemical results
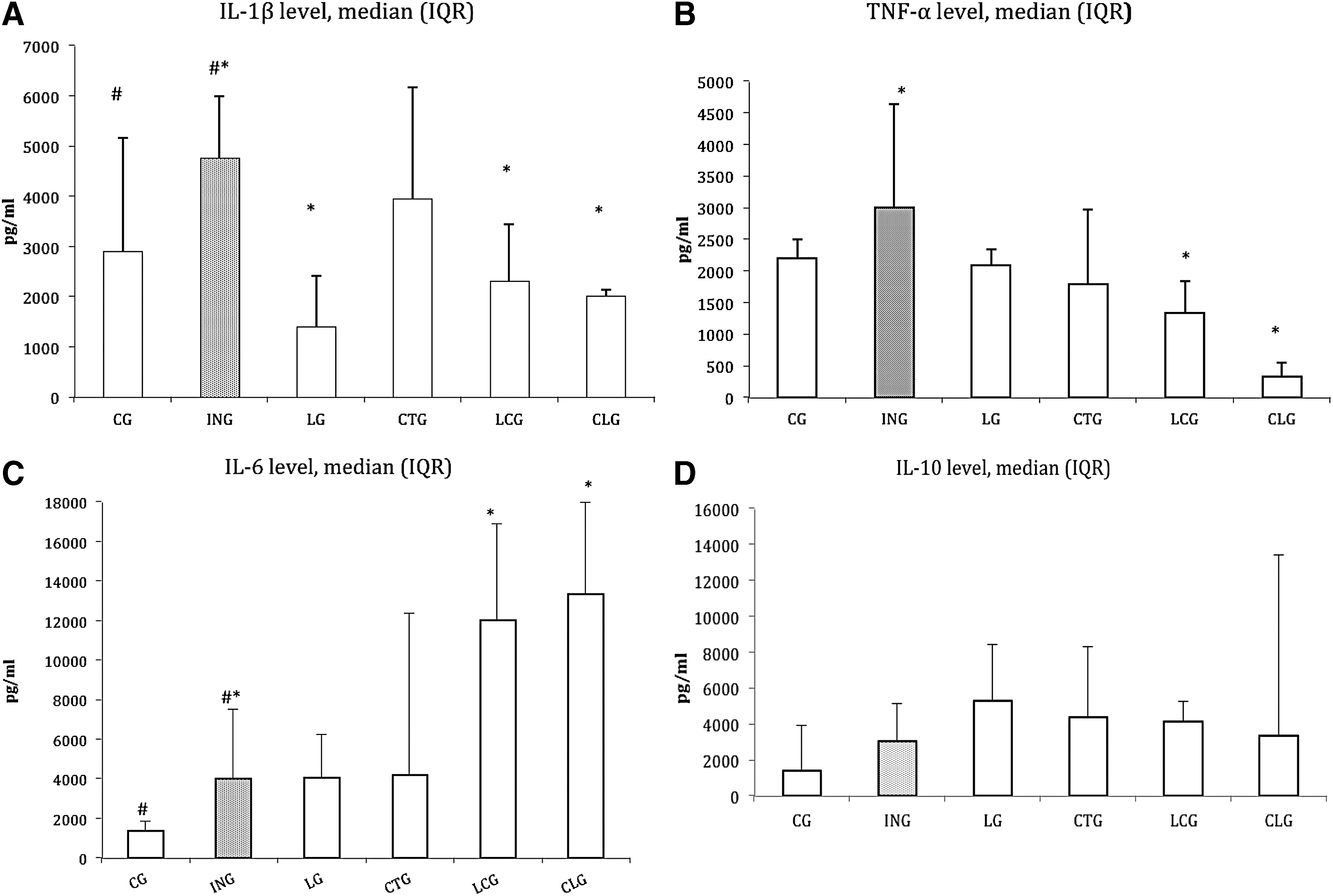
The Kruskal–Wallis test revealed a statistically significant difference in IL-1β, TNF-α, and IL-6 cytokine expression across the ING and the four different treatment groups, at X 2(4) = 16, p = 0.00; X 2(4) = 18.5, p = 0.00; and X 2(4) = 15.9, p = 0.00, respectively. The LG recorded the lowest IL-1β median score (Md = 1393). The CLG recorded the lowest TNF-α median score (Md = 321) and the highest IL-6 median score (Md = 13,313). The Kruskal–Wallis test showed no statistically significant differences across the groups for the expression of IL-10, at X 2(4) = 2.5, p = 0.64. The LG recorded the highest IL-10 median score (Md = 5281). The output from the pairwise Mann–Whitney U statistical test on cytokine expression is summarized in Table 3.
The mean rank for TNF-α, IL-1β, IL-6, and IL-10 cytokine expression in each group and significance level for each comparison is shown.
IL, interleukin; TNF-α, tumor necrosis factor-α.
Trauma model (comparison against healthy CG)
Our experimental model significantly increased IL-1β (p = 0.01) and IL-6 (p = 0.04) levels in the ING (Fig. 2A, C). TNF-α and IL-10 expression increased, but it did not differ significantly (p = 0.20, p = 0.10) from those of the healthy controls (Fig. 2B, D).
Levels of inflammatory cytokine IL-1β
Monotherapies (comparison against ING)
The LG showed significantly decreased levels of IL-1β (p = 0.00) and bordered the threshold for statistical significance (p = 0.06) for IL-10 cytokine expression (Fig. 2A, D). TNF-α expression was nonsignificantly (p = 0.15) reduced in the LG (Fig. 2B), whereas IL-6 expression remained equal (p = 0.42) to that of the ING (Fig. 2C). The CTG displayed cytokine expression in favor of an anti-inflammatory response, but no significant between-group differences were found (Fig. 2A–D).
Adjunctive therapies (comparison against ING)
Both groups combining LLLT and cryotherapy showed significantly reduced levels of IL-1β (p = 0.00, p = 0.01) and TNF-α (p = 0.00, p = 0.02). The expression of IL-6 increased significantly (p = 0.00) in both groups, whereas IL-10 remained at levels (p = 0.75, p = 0.63) similar to those of the ING (Fig. 2A–D).
Tendon histology
The morphological appearance of the healthy control tendons had overall features consistent with normality. The collagen bundles were lightly stained (pale pink) and showed no signs of rupture. Tenocytes (dark blue) were situated regularly between the collagen bundles (Fig. 3). Accordingly, the normal tendon tissues corresponded with a score of 3 out of 12 points in our semi-quantitative histology analyses (Table 4).
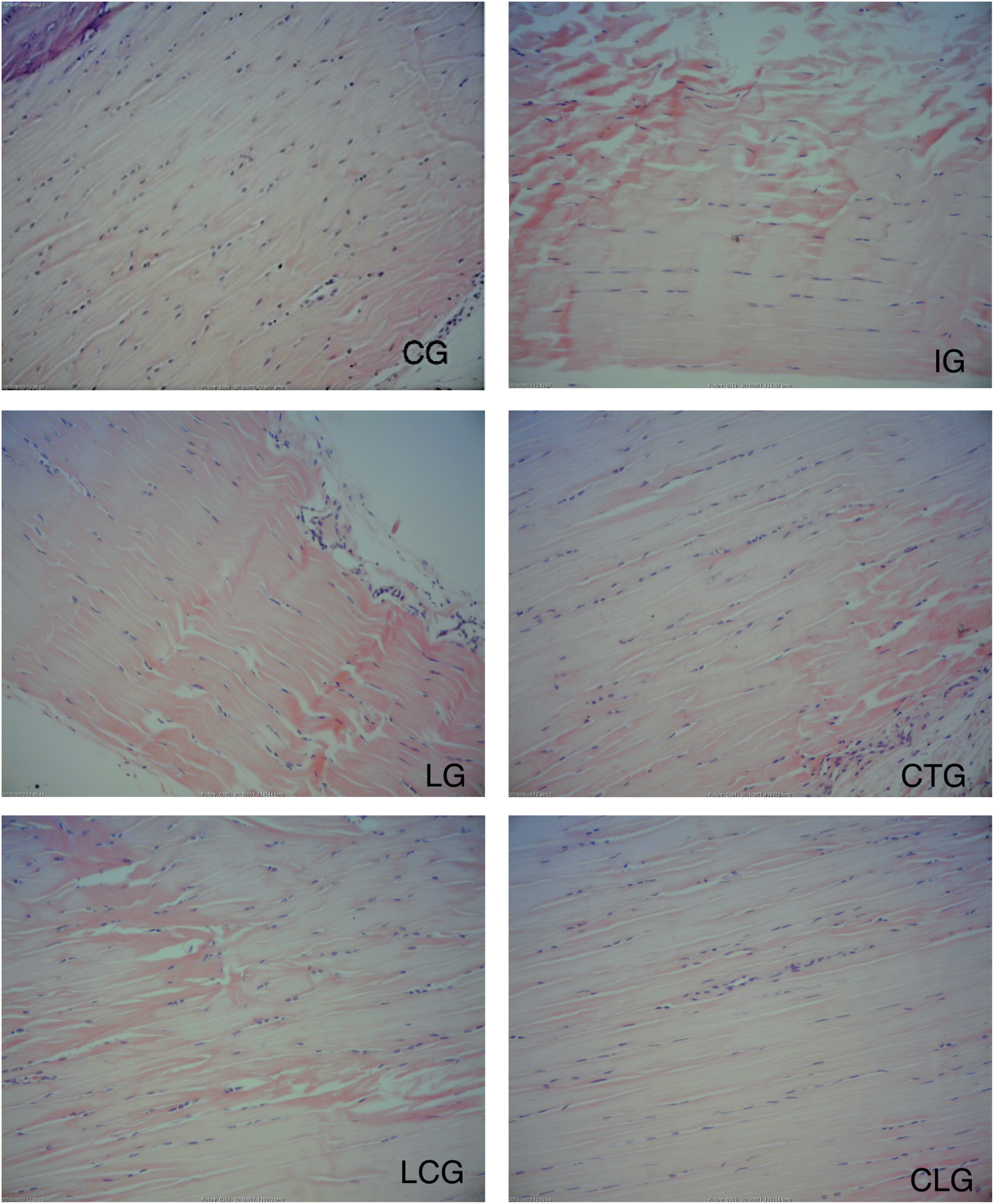
Histological microphotographs (100 × ) of Achilles tendons 24 h after trauma. CG, control group; ING, injured nontreated group; LG, LLLT group; CTG, cryotherapy group; LCG, LLLT first/cryotherapy group; CLG, cryotherapy first/LLLT group. Collagen bundles are uninterrupted with homogeneous light staining; tenocytes are regularly perfilated between the collagen bundles (CG). Region of severe tendon disruption showing a multitude of interrupted collagen bundles with darker eosin staining and randomly scattered tenocytes around the lesion (ING). Irregularly shaped collagen bundles with a small degree of interruption, perfilated tenocytes between the collagen bundles, and slight heterogeneous staining, indicating slight tendon disruption (LG). Collagen bundles showing slight disruption, slight bundle interruption, slightly disorganized tenocytes around the lesion, and slightly irregular staining (CTG). Moderate signs of tendon disruption. Irregularly shaped collagen bundles and moderately heterogeneous staining. Tenocytes scattered irregularly around lesion (LCG). Almost normal appearance with no signs of tendon disruption. Collagen bundles are largely uninterrupted with slightly heterogeneous eosin staining, and tenocytes are regularly perfilated between collagen bundles (CLG).
The total histology score ranges from 3 (best) to 12 (worst), and it comprises characteristics of collagen disruption, tenocyte infiltration, and eosin staining for each specimen. Each value represents the mean of all group samples, and the total score indicates the sum of means for each group.
The ING showed opposing characteristics, with regions of severe tendon rupture. A number of collagen bundles were disrupted, resulting in areas of prominent darker staining within the tendon. Tenocytes were scattered randomly around the lesion (Fig. 4). These findings corresponded to a total of 11 out of 12 points in the histology score (Table 4).
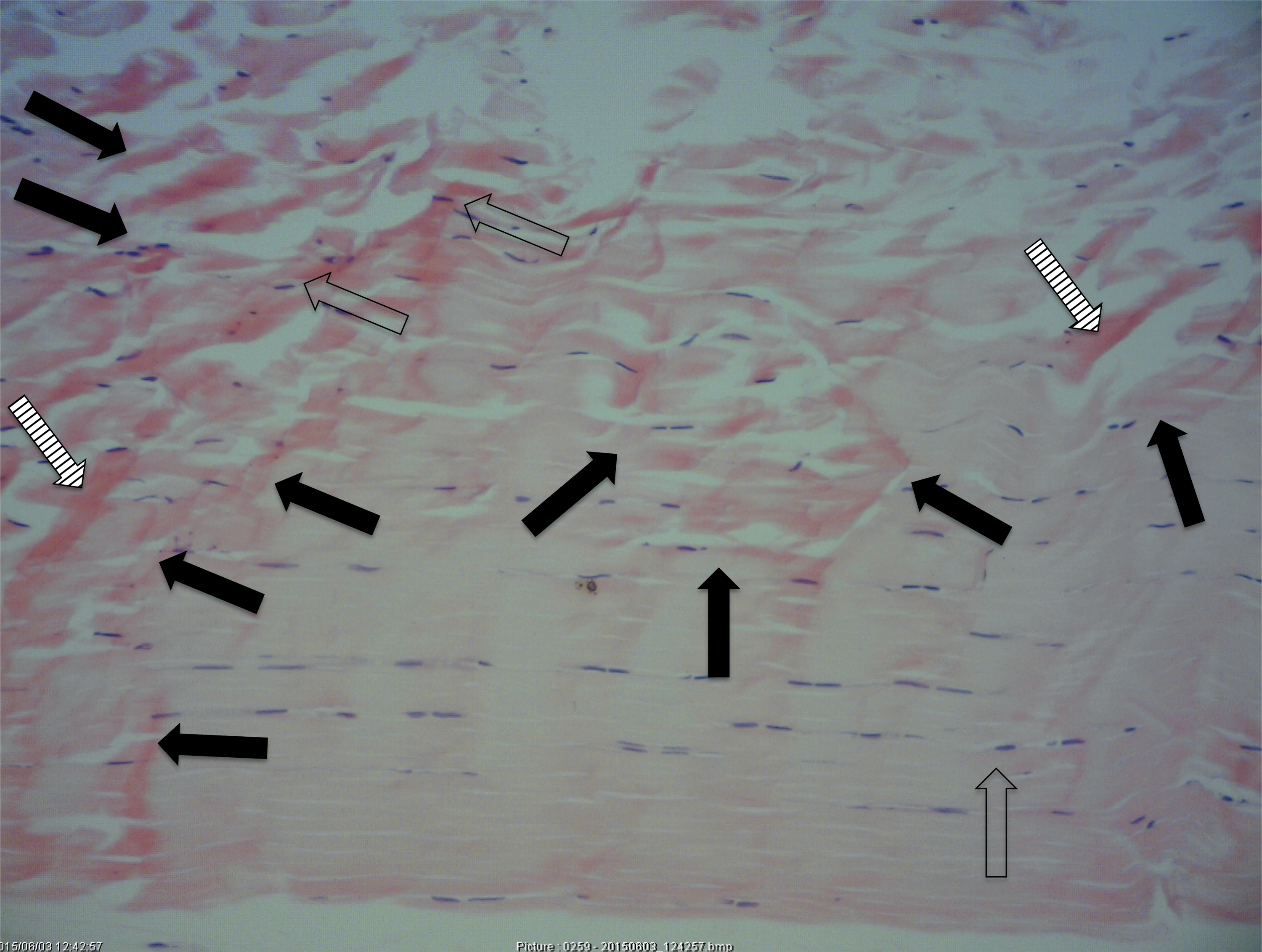
Histological microphotographs of injured nontreated Achilles tendon 24 h after injury. The specimen shows large regions of disrupted collagen bundles (black arrows) with darker eosin staining (white arrows). The tenocytes are distributed and scattered irregularly around the lesion (transparent arrows).
The groups treated with LLLT or cryotherapy alone had a general appearance, indicating slight tendon rupture. Small areas of irregularly shaped collagen bundles and disruption were evident, with somewhat larger regions of dark staining in the CTG compared with the LG. The distribution of tenocytes was slightly disorganized, with small cluster formation around the lesion (Fig. 4). LLLT and cryotherapy treatment resulted in total histology scores of 6 and 7, respectively, out of 12 (Table 4).
The LCG showed consistent signs of moderate tendon rupture. There were larger regions of irregularly shaped collagen bundles and heterogeneous staining compared with the other treatment groups. Tenocytes were scattered irregularly around the lesion (Fig. 4). This treatment group displayed morphological features that most closely resembled those of the ING, resulting in a total histology score of 8 out of 12 in our analyses (Table 4).
The CLG displayed a near-normal appearance, with no sign of tendon rupture. As seen in the healthy controls, the collagen bundles were lightly stained and largely uninterrupted. The distribution of tenocytes was situated regularly between the collagen bundles (Fig. 4). As such, this group achieved a histology score of 3, similar to that of the noninjured control tendons (Table 4).
Discussion
Both isolated LLLT and cryotherapy modulated the inflammatory response after injury. Cryotherapy failed to reach statistical significance over no treatment for any of the targeted inflammatory cytokines. LLLT significantly reduced pro-inflammatory IL-1β cytokine expression in the presence of the highest levels of IL-10 across all treatment groups. We highlight this finding, as IL-1β is a catabolic mediator that is known to accelerate tendon degradation, whereas IL-10 is an effective anti-inflammatory cytokine that is associated with tendon remodeling. 30 Thus, LLLT seems to be beneficial in simultaneously reducing inflammation and stimulating the tendon repair process.
TNF-α was not significantly reduced in the LG. This intrigued us, since LLLT administered with identical parameters as in our study reduced TNF-α in collagenase-induced Achilles tendinopathy in rats 2 h post-trauma. 24 We used a trauma model to inflict tendon injury, and treatment was administered 1 h postinjury. Therefore, it is possible that the LLLT treatment was administered too soon, as proposed in a study by Joensen et al., 27 wherein 3 J of laser administered 30 min after blunt trauma led to increased tendon edema. This point is interesting, as de Almeida et al. 31 found significantly reduced TNF-α levels after 1 J of LLLT, but not 3 J or cryotherapy, in trauma-induced muscle injury in rats. Thus, it is possible that our dose of 3 J was too high, and that the combination of LLLT and cryotherapy mimics the effects seen with lower doses.
At present, no other studies have examined the effect of cryotherapy and LLLT in tendinopathy treatment. One study compared the effect of LLLT, cryotherapy, and diclofenac in acute muscle injury in rats. Similar to our study, significant effects on inflammatory markers were found after LLLT, but not cryotherapy. 31 PBM was also found to be superior to cold-water immersion therapy in reducing muscle damage and inflammatory reactions in rat muscle, 32,33 and in improving postexercise muscle recovery rates in male futsal players. 34 Our study adds to the evidence that PBM seems more effective than cryotherapy in reducing inflammatory reactions.
The combined therapies significantly reduced the levels of all targeted pro-inflammatory cytokines (IL-1β/TNF-α), but no strong evidence was found for an effect on the anti-inflammatory cytokine IL-10 compared with no treatment. The superior effects on TNF-α seen in the two groups combining cryotherapy and LLLT could represent an anti-inflammatory “add-on” effect. LLLT induces photochemical actions on mammalian cells by increasing activity of the enzyme cytochrome c oxidase in mitochondria, which, in turn, modulates the production of pro- and anti-inflammatory mediators. 5 Cryotherapy is believed to suppress inflammation primarily by decreasing blood flow, thereby slowing down the delivery of inflammatory mediators. 35 We observed a superior anti-inflammatory effect in the combined therapy groups. It is possible that LLLT becomes more efficient in presence of the suppressive actions on cell invasion induced by cryotherapy.
It has also been suggested that increased plasma levels of IL-6 inhibit the production of TNF-α in humans. 36 Interestingly, IL-6 was significantly elevated in both groups combining LLLT and cryotherapy compared with no treatment. This result was not observed in the isolated therapy groups, where IL-6 remained at the same levels as that of the ING. As IL-6 plays a dual role in tendon inflammation, displaying both pro- and anti-inflammatory effects, the results of our analysis may be interpreted likewise. Tendons in IL-6 knock-out mice have been shown to exhibit significantly inferior mechanical and organizational properties, demonstrating the crucial role of IL-6 in tendon healing. 37 IL-6 has also been shown to increase in tendons during exercise 38 and in healing human Achilles tendons postsurgery, 39 actions that are associated with cell proliferation and survival. 30 Although the role of IL-6 in tendon disorders remains unclear, our findings of increased levels after combining LLLT and cryotherapy might indicate a more rapid shift toward a resolving inflammatory phase.
However, increased levels of IL-6 cannot explain the contradictive biomechanical and histological findings in the combined therapy groups. Cryotherapy treatment before LLLT seemed to shift the injured tendon mechanics significantly toward normal behavior, whereas LLLT before cryotherapy resulted in the poorest outcome on force of all of the included groups, demonstrating a significant negative interaction. It has been demonstrated that immediate cryotherapy after acute muscle injury in rats delayed and impaired the regeneration process by inducing chronological changes in the number of macrophages and expression of growth factors. 40 In our study, the application of LLLT followed by cryotherapy (LCG) perhaps triggered similar events 1-h post-trauma. Interestingly, the LCG also showed the lowest levels of the anti-inflammatory IL-10 across all treatment groups, which could lead to poor stimulation of fibroblastic cells and tendon remodeling. 30 The polarized biomechanical results between the LCG and CLG correlated well with our histopathological analyses. The LCG displayed the poorest histology score, whereas the CLG displayed an almost normal histological appearance and had the best score out of all the treatment groups.
Our findings indicate that cryotherapy and LLLT induce different mechanisms to alter tendon biomechanics. The anti-inflammatory actions and biostimulating effects of LLLT significantly increased the ability to withstand force in tendinopathy, but they did not have an effect on tendon stiffness. The opposite actions were observed for tendinopathy that was treated with cryotherapy, wherein tendon stiffness increased significantly in the absence of any effects on force. Porcine ligament stiffness has been demonstrated to increase almost proportionally with declining temperatures, and the limited elastic response during loading has been explained by the increased viscoelasticity in cooled collagen tissue. 41 However, studies on cryotherapy-induced tendon stiffness in humans are few, and the results remain unclear. 42 In one study, increased Achilles tendon stiffness was found in healthy men after cold-water immersion of the lower leg. 43 We have shown that rat tendons subjected to cooling alone reached tissue failure at similar load levels but at lower elongation (strain) levels than nontreated tendons. Considering the transient adverse changes to joint proprioception 44 and muscle strength, 45 which are demonstrated immediately after cooling in humans, temporary activity restriction or adequate warm-up seem to be sensible precautions before initiating exercise.
Several questions arise after the results of our study. A significant decrease in capillary blood flow has been reported after local cryotherapy of human Achilles tendons. 46 Similarly, Yanagisawa et al. 47 found reduced blood volume and hemoglobin levels in the underlying skin and skeletal muscle after cryotherapy. As hemoglobin absorbs light in the near-red and infrared regions of the spectrum, 48 cryotherapy-induced vasoconstriction in the skin and underlying tendon might influence both the penetration and absorption of laser light. It is also not known whether cryotherapy alters skin or tendon density, or how it affects laser penetration. However, the counteracting negative effect seen with LLLT before cryotherapy cannot be affected by changes in the optical properties of the tissue. The subsequent cooling of an irradiated tendon produced inferior biological effects in our study, which are more likely to be caused by an abrupt reduction in the metabolic state.
The experimental trauma model produced increased expression levels of pro- and anti-inflammatory cytokines, consistent with reactions known to occur in local inflammatory tendon disease. 49 It also caused a weakening of tendon material, loss of stiffness, and loss of ability to withstand force before rupturing. These findings correlated well with the histopathological appearance of the tendons. Nevertheless, the use of animal models in tendinopathy research has several shortcomings. At present, there is no ideal model to induce tendinopathy in animals, 50 and all of the models share the common limitation of an unclear pathophysiology in human tendinopathy. 15 We decided to use the mini-guillotine model to mimic a tendon disorder with inflammatory components, which is comparable to early or acute tendinopathy. 51 Achilles tendinopathy in humans is often associated with overuse, and it can develop over months or even years. 18 In vivo animal models such as repeated uphill treadmill running would better mimic the etiology of chronic human Achilles tendinopathy. However, it is also a more stressful procedure for the animals than our mini-guillotine model. We also found no evidence of its superiority in causing inflammatory reactions. Perhaps the most important limitation of this study is the absence of a functional outcome, as activity-related pain is a common clinical feature in human tendon disorders. 52 This point should be emphasized, as histopathological changes and pain intensity do not necessarily correlate in humans. 53 Consequently, the validity of our findings would be strengthened by indirect measures of pain such as analysis of gait pattern. 50 Our cytokine analysis also showed considerable variance, indicating that the sample size should be increased in future replica studies. In view of these shortcomings, careful consideration should be given before extrapolating the findings of this study to clinical practice.
Conclusions and Summary
LLLT induced actions on cytokine expression that were associated with reduced inflammation and stimulatory repair. The combination of LLLT and cryotherapy may produce an anti-inflammatory add-on effect, and the biomechanical and histological results showed that the order of therapy administration is essential. Cryotherapy before LLLT induced positive interactions, with mechanical behavior closest resembling healthy tendons and a near-normal histological appearance. Cryotherapy after LLLT, however, displayed the poorest mechanical behavior and histological score of all the groups.
Footnotes
Acknowledgments
Dr. R.À. Lopes-Martins would like to thank Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) for the research grants 2015/06502-3.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.