
Abstract
Introduction
W
To date, there have been only three documented cases of generalized urticarial eruption following laser tattoo removal. All three cases have been amenable to medical therapy or experienced self-resolution of symptoms. None of them demonstrated an antigenic culprit of the allergic reaction. 3 –5 We present below a unique case of a generalized urticarial eruption following laser tattoo removal that was found to be associated with titanium dioxide in the tattoo pigment, was recalcitrant to medical therapy, and was cured only after surgical excision of the tattoo remnant.
Report of a Case
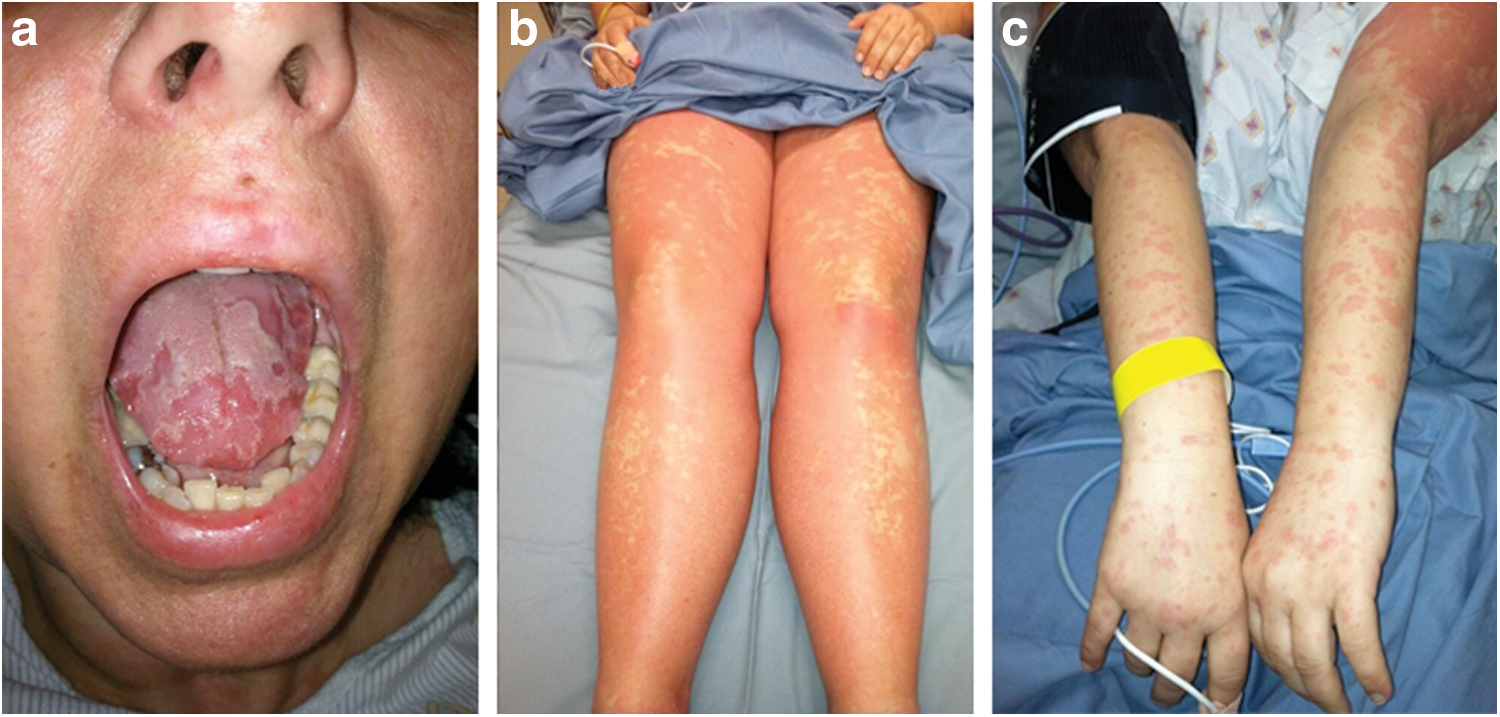
A 46-year-old German female presented with a 3-day history of rapid-onset, diffuse, indurated, migratory erythematous pruritic plaques (Fig. 1a–c). Less than 24 h before the onset of her diffuse cutaneous symptoms, she had received a fourth laser treatment for removal of a 7 × 15 cm blue/green tattoo on her right shoulder (Fig. 2) with a 1604 nm Q-switched Nd:YAG laser. The patient received her laser tattoo removal treatments from an unaffiliated dermatology practice, and the exact settings and manufacturer of the laser were unknown by the patient. The patient denied any adverse local or generalized cutaneous or systemic reactions to the previous three laser treatments. She also denied any preceding respiratory illness or new medication use before the onset of her symptoms. The patient reported that it had been 20 years since she first received the tattoo and denied any history of local or generalized allergic reaction from the time of its placement up until the fourth laser treatment. The patient also denied any personal history of allergies or atopic disease. A 4 mm punch biopsy was performed and revealed superficial perivascular inflammation with dermal eosinophils, consistent with urticaria.

7 × 15 cm blue/green tattoo on right upper arm.
The patient was started on cetirizine 10 mg daily and a 2-week prednisone taper. Six days later, she had resolution of her pruritis and marked decrease in the number and size of her urticarial lesions. Three weeks later, she continued to have intermittent mild urticarial plaques at areas of pressure or scratching. She was titrated up to 20 mg of cetirizine daily, which successfully suppressed her symptoms. The patient continued taking her regimen of antihistamines and received a fifth laser treatment at the same unaffiliated treatment facility 3 months after her initial generalized urticarial reaction. Within 24 h, the patient's generalized urticaria recurred, despite the continued use of cetirizine at the time of the treatment. She was given 360 mg of fexofenadine daily, in addition to her daily cetirizine, which successfully controlled her symptoms.
Despite counseling against further laser tattoo removal treatments, the patient received one final treatment 2 months following her fifth laser treatment. Her symptoms recurred as before, and the patient was subsequently given 40 mg of intramuscular triamcinolone, started on doxepin 50 mg as needed, and switched to levocetirizine 5 mg twice daily. Despite these aggressive medical interventions, her symptoms were poorly controlled.
Three months following the final laser treatment and despite continuing high-dose daily antihistamines, the patient's generalized urticaria persisted. At that point, the patient stopped all medication and consented to surgical excision of the remaining tattoo, as she was determined to have her tattoo removed and the risk of further laser treatments did not seem reasonable to her.
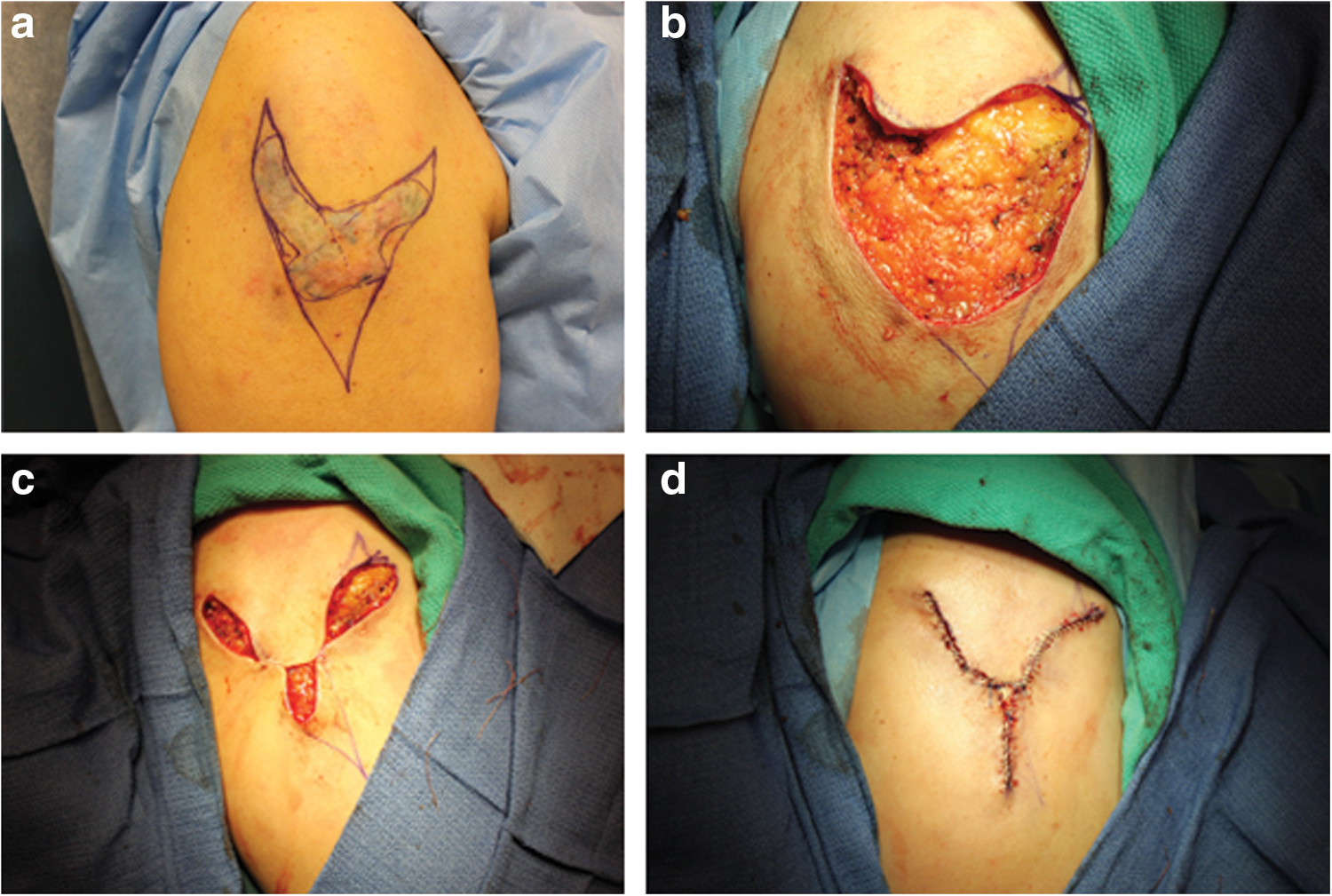
A surgical treatment plan using a V to Y/Mercedes advancement flap, which was inclusive of all the clinically visible tattoo pigment and took advantage of the shape and orientation of the tattoo, was agreed upon with the patient (Fig. 3a). The entire tattoo was excised and the flaps were raised by dissection in the subcutaneous plane. The remaining wound edges were undermined and hemostasis obtained (Fig. 3b). A total of three Burrow's triangles were excised after placement of the two key sutures resulting in closure of the central portion of the defect (Fig. 3c). The remaining smaller defects were closed in a layered manner. Where the edges were not closed, a full thickness skin graft derived from one of the discarded Burrow's triangles was inset to fit the residual defect (Fig. 3d).
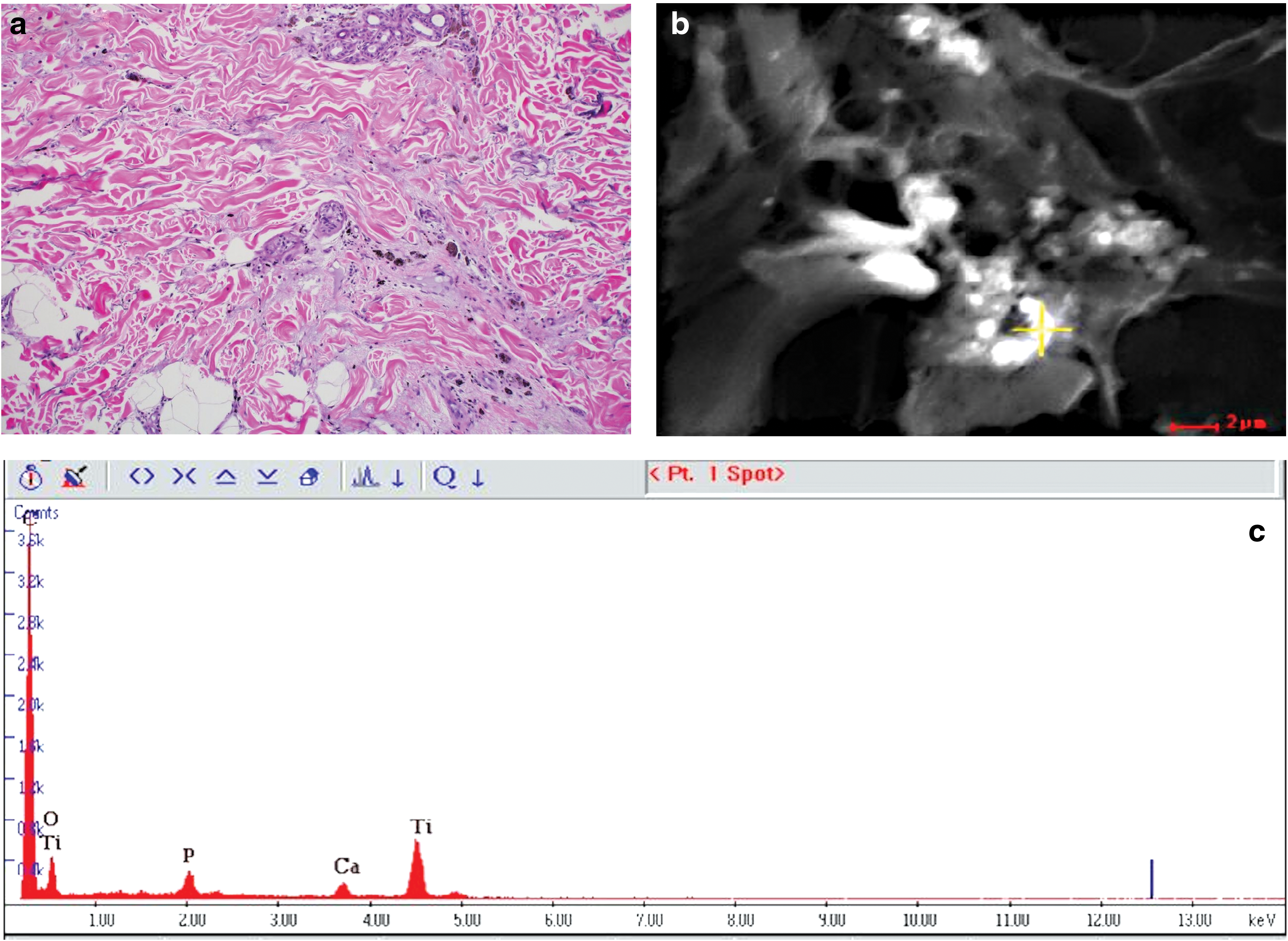
Microscopic examination of the excised tissue revealed tattoo pigment within dermal macrophages with associated perivascular and interstitial lymphocytes and eosinophils consistent with an urticarial reaction in the tattooed skin (Fig. 4a). Scanning electron microscopy and energy-dispersive X-ray analysis revealed titanium dioxide and calcium phosphate in the tissue (Fig. 4b, c). The titanium dioxide was presumed to be from the tattoo pigment, while the calcium phosphate was presumed to be of endogenous origin (dystrophic calcification).
Within 2 weeks of surgical excision of the tattoo, and without the use of antihistamines or corticosteroids, the patient reported complete resolution of her diffuse urticarial lesions and pruritis. Beginning 1 month after excision, the patient received a 1-year course of laser treatments to improve pliability and reduce the thickness and vascularity of her scar. These included three Lumenis Carbon Dioxide (CO2) treatments at 10,600 nm, four Sciton Intense Pulsed Light treatments at 560 nm, and three Candela Vbeam Perfecta Pulsed Dye Laser treatments at 595 nm. The patient did not experience any local or generalized allergic reactions with these treatments (Fig. 5). One-year following her tattoo excision, the patient remained symptom free.

Post-surgical scar on 1-year follow-up, after laser treatments.
Discussion
Adverse reactions to tattoo pigments have been well documented and investigated over the past several decades as tattoos have become more common in the general population. The most common adverse reaction following initial tattoo placement is a lichenoid reaction most common to mercury sulfide (cinnabar) found in red tattoo pigment. 6,7 Other allergic reactions following tattoo placement include photoallergic or phototoxic reactions from cadmium sulfide (yellow and red pigment), granulomatous and pseudolymphomatous reactions associated with red pigment and other pigments, and localized urticaria from cobalt and carbon (blue and black pigment). 7,8
While local reactions to tattoo pigment following tattoo placement or laser tattoo removal therapy are well documented, reported cases of diffuse allergic reactions following laser tattoo removal are rare. 1 –5 These rare reactions are thought to be caused by widespread immune activation against tattoo pigment that is released during the process of laser therapy. The energy from the laser causes selective photothermolysis of pigment-containing cells, resulting in release of tattoo pigment from inside the dermal cells into the extracellular space. The pigment is then taken up by the lymphatic system and distributed throughout the body, where it is recognized as a foreign antigen by distant lymphocytes and mast cells, leading to a generalized allergic reaction. 9
We propose this same mechanism in our patient. We hypothesize that serial laser treatments led to increased fractioning and exposure of extracellular titanium dioxide, which was the only known foreign antigen found through scanning electron microscopy and energy-dispersive X-ray analysis of the patient's excised tissue. The end result was postulated to be a significant priming of immune response to residual titanium haptens, systemic dispersion, and widespread immune activation causing generalized urticaria. While it was not reasonable to subject the patient to the surgical risk of lymph node biopsy or excision, prior reports have clearly demonstrated tattoo ink in distant nodes following tattoo removal. Our patient's presentation is consistent with these prior reports and explanations of how laser tattoo removal treatments result in both local and generalized cutaneous reactions. 9
Prior reported cases of generalized urticaria following laser tattoo treatment have not identified which component of tattoo ink may have led to the generalized urticarial reaction. 3 –5 The majority of cases of chronic urticaria are idiopathic, and it is possible that our patient's symptoms were not secondary to titanium dioxide. However, the patient's rapid and recurrent onset of generalized urticaria with challenge and rechallenge of laser tattoo removal, her abrupt resolution of symptoms within days of the surgical excision of her remaining tattoo ink, and the scanning electron microscopy findings strongly implicate titanium dioxide, perhaps altered by laser treatment, as the antigenic source of our patient's urticaria. We do not feel the laser therapy alone was the cause of the patient's urticaria, as she had subsequent laser treatments for the cosmetic appearance of her excision scar without recurrence of local or generalized urticaria and pruritis.
The patient in our case experienced generalized urticaria that was ultimately recalcitrant to over 6 months of medical therapy. Initially, pre- and post-treatment with high dose second-generation antihistamines was moderately effective at managing our patient's symptoms, and this approach has been reported to be successful. 1 –5 However, the patient's symptoms became increasingly difficult to manage and her urticaria and pruritis persisted, despite intramuscular corticosteroids and 3 additional months of daily high-dose antihistamines following her final laser tattoo removal treatment. The patient then stopped all medical management for her urticaria and experienced rapid, complete, and lasting resolution of her symptoms within days of surgical excision of the remainder of her tattoo.
In contrast, the other documented cases of generalized allergic reactions following laser tattoo removal therapy were amenable to medical therapy, experienced self-resolution of symptoms, or had loss of patient follow-up. 3 –5 In addition, none of these cases, or other cases investigated by the authors, required or demonstrated surgical intervention as a cure for generalized allergic reactions to tattoo pigment. Had laser tattoo removal treatment ceased early on, our patient would not likely have required excision, and medical management with antihistamines and steroids alone would likely have been sufficient to treat her symptoms. However, the partially treated tattoo was cosmetically unacceptable to the patient, which is why she continued with laser tattoo removal treatments, and ultimately desired excision of the remainder of her tattoo.
It is important to note that the patient in this case had a tattoo that was a suitable size for excision. In the authors' experience, and as reported in the literature, the use of fractional ablative lasers can be a valuable addition to traditional tattoo removal lasers by creating a port for pigment extrusion and may be a better option for patients who experience allergic reactions from tattoos that may be too large for surgical excision. 10 However, there is only limited data to indicate that this method of tattoo removal would prevent or preclude a similar type of allergic tattoo reaction in someone who has not been previously sensitized and only a few reports indicating that it is potentially safer than other forms of laser tattoo treatment in a previously sensitized individual. Given our patient's intractable urticaria, and her staunch belief that a scar would be preferable to a partially treated tattoo, a surgical approach was used to excise the remainder of her tattoo and attempt to treat her allergic reaction.
Footnotes
Acknowledgments
Michael Lewin-Smith, MD, Joint Pathology Center, Defense Health Agency, National Capitol Region Medical Directorate, US Army Forest Glen Annex, Maryland—performed scanning electron microscopy and energy-dispersive X-ray analysis on excised tattoo. Marie Jenkins, HT, ASCP, US Army Forest Glen Annex, Maryland—performed scanning electron microscopy and energy-dispersive X-ray analysis on excised tattoo. Patrick Ellison, MD, Mohs Surgeon, and Chad M. Hivnor, MD, Staff Dermatologists at San Antonio Uniformed Services Health Education Consortium (SAUSHEC) Dermatology Residency, San Antonio, TX—involved in care of patient.
Author Contributions
Drs. Todd T. Kobayashi, Jason G. Arnold, Chad Hivnor, and Casey D. Bowen had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: T.T.K., J.G.A., C.D.B., and H.B.W. Acquisition, analysis, and interpretation of data: T.T.K., J.G.A., C.D.B., and H.B.W. Drafting of the article: H.B.W. Critical revision of the article for important intellectual content: T.T.K., J.G.A., and C.D.B. Statistical analysis: not applicable. Obtained funding: not applicable. Administrative, technical, or material support: not applicable. Study supervision: T.T.K., C.D.B., J.G.A., and Hivnor.
Author Disclosure Statement
No competing financial interests exist.