
Abstract
Introduction
L
Among studies on the efficacy of laser hair removal (LHR), vascular treatment, and pigment or tattoo removal, very few of them have standardized the exact treatment technique. 6 –9 Therefore, limited studies have focused on describing or comparing the efficacy of new laser systems that assess the actual techniques used in clinical practice, including the extent of the omitted area, extent of the overlapped area, or number of shots per area.
Studies on dermatological laser treatments tend to assume that physicians use the best parameters and techniques to perform the treatments. 10 –12 It is also assumed that treatments performed by the same physician do not differ in terms of techniques. Therefore, we developed a device that measures the omitted or overlapped areas during laser irradiation, 13,14 and we used it to assess the omission rate and overlapping rate of physicians who performed simulated hair removal procedures using a diode laser.
Materials and Methods
This study protocol was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB no.: C-1503-147-661). The study was conducted in accordance with the 2013 revision of the Declaration of Helsinki.
Setup of the laser beam detection kit
In this study, we used a high-powered, long-pulse diode laser system (800 nm; LightSheer XC, Lumenis, Santa Clara, CA) at 25 J/cm2, 100 ms, and 1 Hz for fluence, pulse duration, and frequency, respectively. The shape of the light output window was square (12 × 12 mm2). This diode laser is used for various types of hair removal devices, 6,15 –18 and it is currently one of the most widely used laser systems for hair removal.
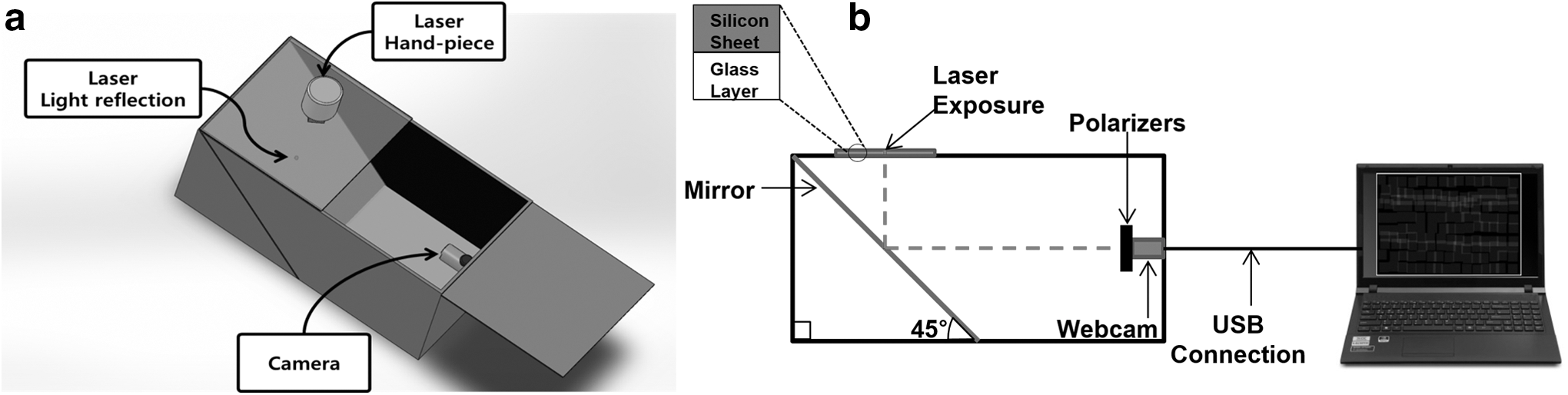
Figure 1 depicts the design of the setup of the laser beam detection kit (LBDK). A semitransparent silicone sheet (150 × 100 mm2) was used as the target area, and it was placed on top of the glass layer to mimic friction on human skin. Figure 2 shows the hand-piece tip of the laser device used during the clinical trial.
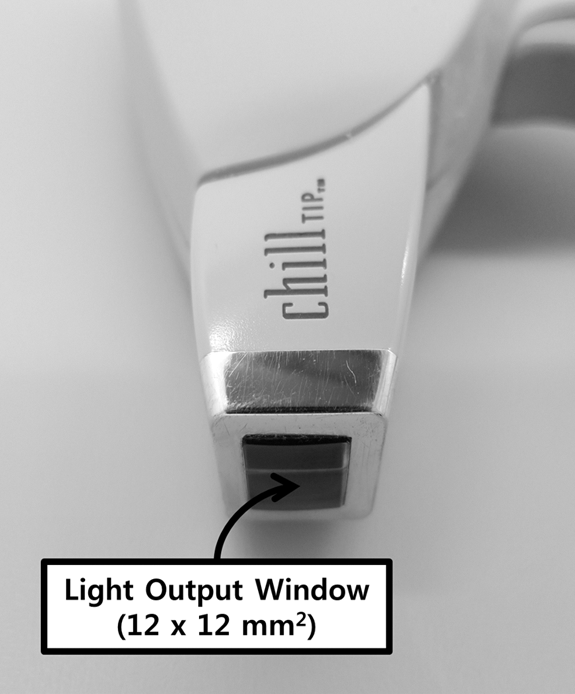
Hand-piece tip of the laser device used during the clinical trial. The light output window's area was 12 × 12 mm2, and it was surrounded by the cooling area.
Study design
Eight laser physicians were recruited as subjects. Four physicians were from clinic A (a primary private clinic), whereas the other four physicians were from clinic B (a tertiary referral hospital). Physicians were asked to do their best to achieve uniform distribution of laser delivery on the rectangular target area. All physicians applied gel to the target area during the trial to simulate the actual LHR practice.
Before the trial, the physicians were free to practice with the laser. Since the energy transferred around the peripheral area of each laser beam is negligible, physicians were told to assume that the effective spot size was 10 × 10 mm2 even though the actual spot size was 12 × 12 mm2. Each physician performed five consecutive trials per round and another round of five consecutive trials 1 week later. Each trial was recorded from the start to the end. In between the trials, physicians were permitted to take a break.
Image processing procedures
A laser distribution map (LDM) was created through multiple steps using image processing algorithms. Block diagrams of the image processing steps are presented in Fig. 3.
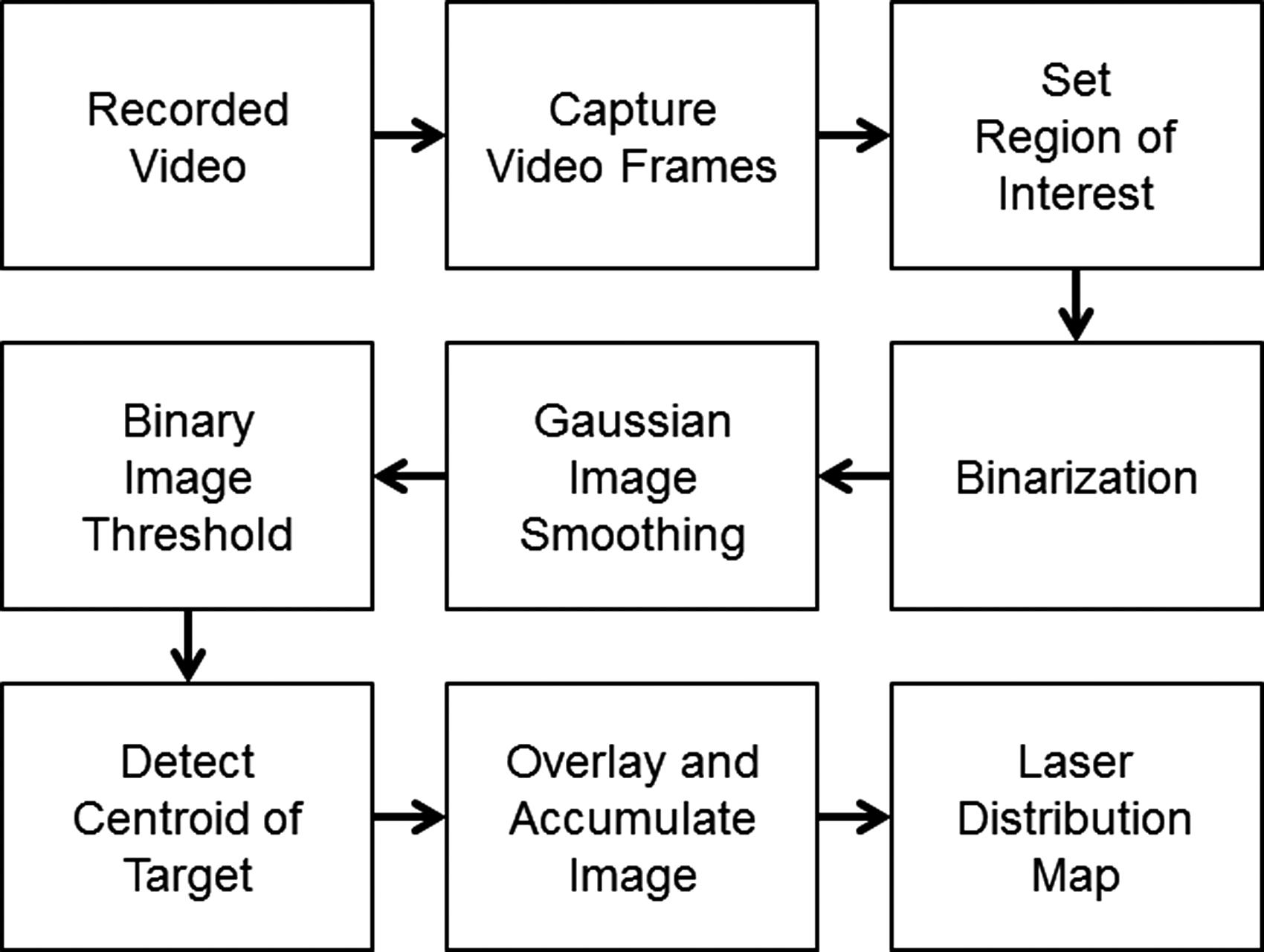
Block diagrams of the image processing steps.
In this study, Noh's methods for image processing and detecting the locations where the laser beam was fired were followed, as previously described. 13 It is the calibration between physical distance and image space distance to collect the exact ratio in terms of pixel per millimeter. From the experiment, 1.2 pix/mm of ratio was collected. Since the camera is rigidly mounted, immobile, and installed inside the simulation bed, this ratio was set and the same was used throughout the procedure. Once the video frames are given as input, region of interest is set to neglect any noises outside of possible laser delivery region. This technique allows blocking reflection made by the flash round the edge-line of the image, bringing only the wanted cluster of lights. Next, the pulse of laser irradiated frames was collected from the video recording. These are what is called as “raw image” and these frames were converted to black and white (binarization) image to further diminish the noise.
In this study, any value of RGB above 40 is converted to white. The limit was tuned experimentally for optimal result. After binarization, locating the centroid of the white figure is conducted. Once the x and y coordinate of the centroid is revealed, it is taken as a center of the laser irradiation spot and square image of laser spot is reconstructed. The reconstructed laser spot is 12 × 12 pix2, which is equivalent to 10 × 10 mm2 square in real-world measurement. The square figure represents the actual size and figure fired from the LOW of the laser device.
To provide visual discrepancy of nonirradiated to multiple irradiated region, a color gradation scheme is adopted. The more irradiated the region, the black colored it turned. The template are on real world is 150 × 100 mm2 and it turned out to be 180 × 120 pix2 in the calibration process. To provide visual recognition between the nonirradiated and multiple irradiated regions, the color gradation scheme was used. Each laser spot was marked on the LDM, and any overlapped regions were superimposed on one another; the more overlapped the regions, the smaller the pixel values.
Evaluation of the laser physician's technical skill
All statistical analyses were performed using a computer statistics program (SPSS, IBM Corp., Armonk, NY). The primary effectiveness assessment was based on the omission percentage (
The data of 80 trials (10 trials per physician) were collected. To validate the statistical analysis of the experimental data, analysis of variance (ANOVA), the Kruskal–Wallis test, and Mann–Whitney test with post hoc Bonferroni adjustment analysis were used to determine whether there were significant differences among the physicians' laser delivery performance. Differences between clinics A and B were also analyzed using the independent t-test and Mann–Whitney test. The test result for significant difference was set by the p-value less than 0.05.
Results
Pattern of the LDM
Figure 4 shows the sample results of the LDM for half of the physicians. Each physician's performance was different. In Fig. 5, the graph shows the distribution of the omission and overlap percentages for all 80 trials.
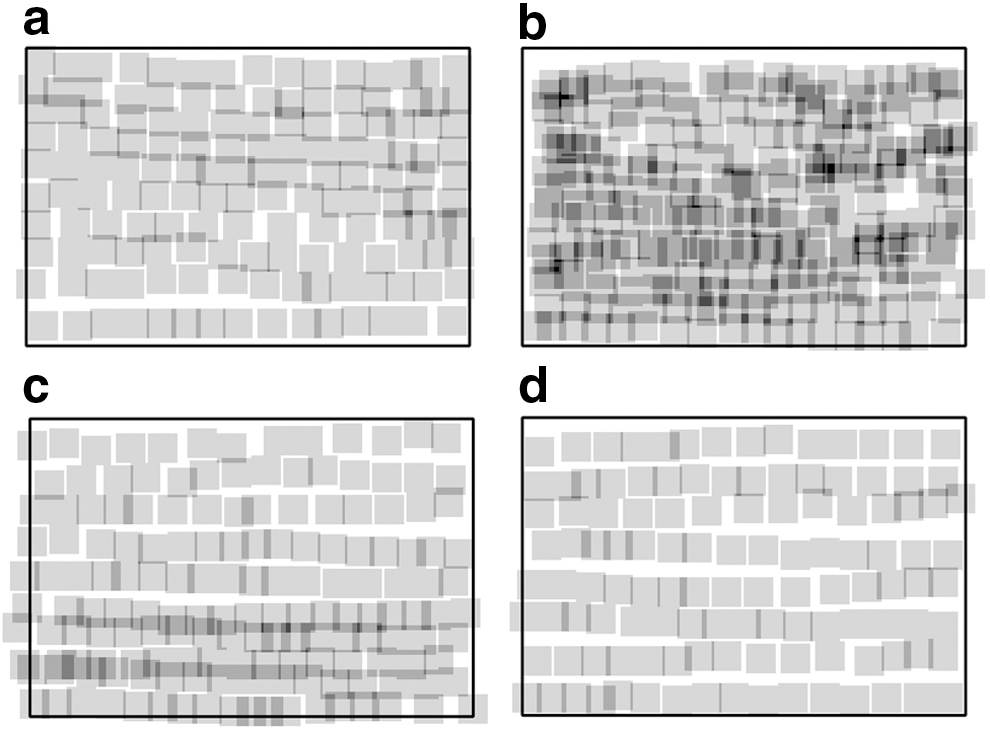
The performance of half of the physicians.
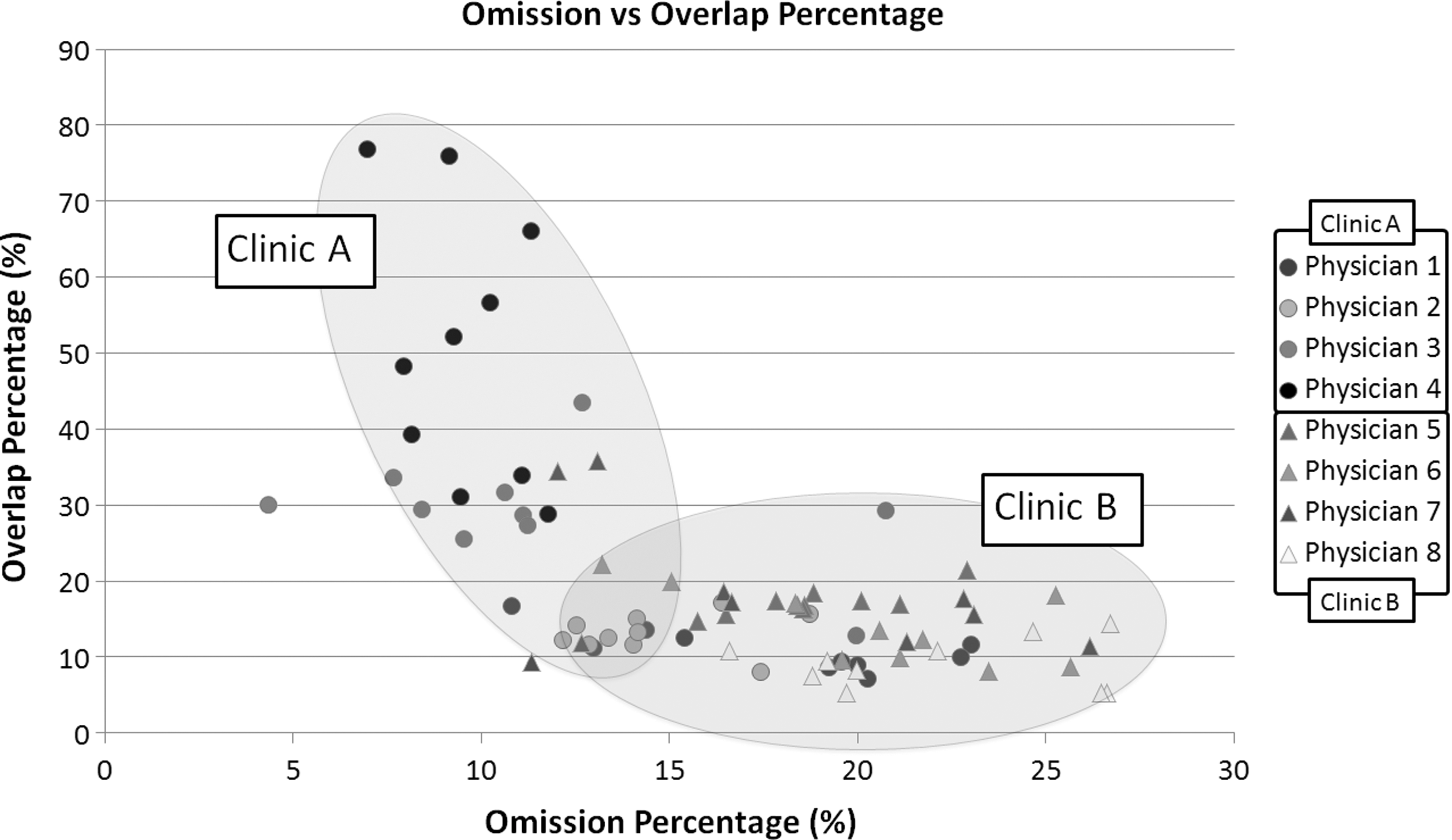
Omission and overlap percentages for each physician. Graph showing the distribution of the percentages for all 80 trials. Physicians were given their own colors to distinguish themselves from one another and represent their affiliation; physicians from clinic A are represented as circles, whereas those from clinic B are represented as triangles.
Comparison among the physicians
Table 1 shows the omission and overlap percentages of each physician. All physicians were compared with one another, which created 28 different combinations. According to ANOVA and post hoc using Dunnett T3 analysis that the omission percentages in 12 of 28 cases were statistically different (p < 0.05). On the basis of the Mann–Whitney test with post hoc Bonferroni adjustment analysis of each case, the overlap percentages in 14 of 28 cases were statistically different (p < 0.0018). Table 2 summarizes the results. The number of shots performed by each physician and trial were analyzed, and the results showed that 13 of 28 cases were statistically different even though physicians irradiated the same target size (p < 0.0018).
SD, standard deviation.
Comparison between clinic A and clinic B
Data from the physicians of clinic A and clinic B were statistically different in terms of the omission percentage, overlap percentage, and number of shots (Table 3), indicating variation in performance. The omission percentage was analyzed using the parametric method, whereas the overlap percentage and number of shots were analyzed using the nonparametric method. According to the results of the analyses, the two clinics had a difference in performance in terms of these three aforementioned criteria.
Discussion
Energy-based medical devices for hair removal have been developed, and efforts continue to improve the efficacy of this treatment. The effect of patients' characteristics 19,20 and the device's mechanical properties, including the wavelength, 4,6,21 pulse duration, 12 spot size, 22,23 fluence, 24 and method of epidermal cooling, 25,26 on the treatment efficacy is currently being assessed in various studies. Such progress has also been made for lasers with other indications. 27 –29 However, very few of these studies have assessed the physician's technical performance.
In the present study, by monitoring simulated LHR treatments, we showed that in addition to the mechanical specifications and power output, the physician's technical skill can possibly affect the treatment outcome. In a previous study, we had eight laser novice practitioners perform 10 simulated treatments on a 100 × 150 mm2 silicone panel, using a tool that can distinguish irradiated and nonirradiated areas. 13 We found that treatment skill differed among the individuals and groups. The degree to which the irradiation area and patterns differed in this study would likely affect the outcome of hair removal.
The proposed research is a pilot study to identify and quantify the diversity among the physicians rather than offering mathematically idealistic laser delivery. The present study began with the assumption that the ideal treatment techniques for LHR have minimal omitted and overlapped areas. However, it figures from the result that neither of the two clinics' physicians achieved near to the idealistic result. The two clinics' physicians were both far from idealistic practice in different criteria. To improve physician's delivery skill, one has to realize his current delivery skill status and know his own deficits. These are undeniable facts that do not only apply to the eight physicians who participated as subjects in this study but to any physician who practices laser delivery.
For LHR, one may think that the efficacy of LHR is inversely proportional to the omitted percentage. However, the Choung group 30 reported that plucking a certain amount of hair from a mouse can trigger organ-level quorum sensing, which induces an up to five times higher regeneration rate of the adjacent, unplucked hairs than using the tumor necrosis factor-α-secreting macrophages as a mediator. If this phenomenon occurs in LHR, more hairs can be regenerated with a higher omission percentage. Reports of stimulated hair regeneration in areas surrounding that of LHR support this possibility. 31,32
Areas of overlapped irradiation are at a higher risk of complications. However, this is still uncertain, as no studies have examined the correlation between the degree of overlap and the risk of complications. In addition, more studies need to examine the amount of hair removed in association with the degree of overlapped irradiation. Reliable methods for evaluating the treatment pattern also are needed. If a robot-assisted automatic LHR system is used in this field in the future, 33,34 accurate omission rates or overlap rates can be obtained, and the association between these values and the treatment efficacy would be accurately assessed in clinical studies.
In the current study, we found that physicians who generally had higher omission rates had lower overlap rates and vice versa. This means that without special training or feedback, physicians may either perform repeated passes to avoid omission, decrease the number of passes to avoid overlap, or shorten the treatment. Physicians who perform laser treatments should be aware of their own omission and overlap percentages to optimize the treatment outcomes. On the basis of the data obtained via simulated laser treatments, physicians will be able to more efficiently avoid omission and maintain an appropriate level of overlap during laser irradiation.
In our study, four physicians from clinic A had an average omission rate of 13.4%, and four physicians from clinic B had an average omission rate of 19.7%, which was statistically significantly different. All physicians from clinic A were familiar with the laser device used in this study. This indicates that treatment experience with the same laser system can have a significant effect on physicians' expertise with the laser treatment.
Regarding the average overlap rate of the two clinics, clinic A had a higher rate than clinic B (26.1% vs. 14.6%), indicating physicians' conscious efforts to decrease the omission rate. It is important to assess the effect of the overlap rate on treatment efficacy or complications in the future.
Five of eight physicians (1, 3, 6, 7, and 8) had a more than 10% discrepancy between the minimum and maximum omission rates (Fig. 5). This indicates that there is a high likelihood that even a physician using the same parameters can still have different outcomes for each treatment.
The laser device used in this study had a square spot size of a 12 × 12 mm2; however, we assumed that the efficacious spot size was about 10 × 10 mm2. Theoretically, because of its square-shaped spot size, the laser can prevent omission and overlap when the spots are adjacent to each other. However, with a circular spot, overlapping is inevitable to avoid omission. For circular spots, decreasing the omission rate is directly associated with increasing the overlap rate, and it is an important yet difficult task to determine the right combination of omission and overlap for optimal results.
However, laser treatment for nevus flammeus, which is generally treated using a pulsed dye laser with a circular spot, enables physicians to distinguish between irradiated and nonirradiated areas. Reyes et al. 35 reported that omission still occurs with 10% overlap, which results in a reticulated pattern. Adams et al. 28 also reported that overlapping laser spots are better than separated spots for treating port-wine stains with an argon laser.
This research provides reasons why different physicians may produce different laser treatment results even though they used the same laser device. We believe that our work and result of this article will be a cornerstone for other researchers who are willing to demonstrate and understand the efficacies of laser treatment technique in the near future. Further clinical trials involving more samples with diverse lasers and protocols are warranted to elucidate the relationship between physician's performance and clinical outcomes.
We assessed the omission and overlap percentages of laser irradiation to provide a detailed picture of the technical skill for common laser skin treatment via simulated LHR. Our study is the first to observe a meaningful discrepancy in these rates between clinics and physicians, and even between procedures performed by the same physician. However, our simulation method has a limitation in that the correlation between the laser treatment skill and clinical efficacy was not evaluated. A tool for assessing the real-time technical skill needs to be developed. Dermatological lasers have advanced significantly because of extensive research on the engineering of the device; however, standardization of the technical skill can also have a significant effect on efficacy and safety. A laser training program similar to a surgical training program 36,37 that helps laser physicians improve their technical skill needs to be developed in the near future.
Footnotes
Acknowledgments
This work was supported, in part, by the BK21 Plus Program through the National Research Foundation (NRF) funded by the Ministry of Education (Grant no. 22A20130011025) and the Seoul Ocean Aquarium (no. 0411-20130059).
Author Disclosure Statement
No competing financial interests exist.