
Abstract
Introduction
T
Some investigations have reported positive effects of photobiomodulation (PBM) on osteoblasts in vitro. Laser radiation significantly stimulated cellular proliferation, bone nodule formation, alkaline phosphatase (ALP) activity, and ALP gene expression compared to a nonradiation group. 8 Another in vitro study reported that PBM increased osteoblast viability, as well as its DNA. In addition, PBM induced a rapid transitory trend toward an increase in the receptor activator of nuclear factor κ-β ligand/osteoprotegerin ratio, along with a tendency toward delayed increase in vascular endothelial growth factor release. 9 Thus, in vivo studies suggested that PBM could promote fracture healing by increasing trabecular bone volume, callus volume, osteoblast numbers, and high stress load in rats. 10
PBM could relieve pain and improve the healing process of closed bone fractures in the human wrist and hand. 11 PBM (850 nm, 100 mW, 8 J/cm2) might stimulate fibroblast proliferation and angiogenesis, as a key component of bone regeneration during the early phase of healing. 12 Garavello et al. confirmed that PBM (He-Ne laser, 31.5 and 94.5 J/cm2) accelerated the deposition of bone matrix and histological characteristics compatible with an active recovery of the injured tissue. It significantly increased the number of blood vessels in a fracture model in rats. 13
Some studies demonstrated that PBM promoted bone regeneration in diabetic animals. Patrocinio-Silva et al. utilized an 808 nm laser (100 mW, continuous wave laser, 0.028 cm2, 3.57 W/cm2, 33 sec, 120 J/cm2, 3.3 J per point) on nonfractured long bones (tibia and femur). They induced TI DM by administration of streptozotocin (STZ); after 1 week, they began laser treatment, which was administered for 18 sessions over 6 weeks. At the end of the experiment, animals were euthanized and their tibias and femurs were extracted for evaluations. The diabetic control group had extensive resorptive areas attributed to osteoclast activity, compared to the control. Laser-treated animals had increased cortex.
Patrocinio-Silva et al. reported that PBM produced increased Runt-related transcription factor 2 (RUNX2) expression, bone mineral content, and bone mineral density (BMD) compared to diabetic control group (DCG). In addition, PBM produced a statistical increase in biomechanical properties that included maximum load at failure [in newton (N) parameter]. It could be possible that TI DM was not established in the animals due to the short-term duration of 1 week. Therefore, the biomechanical data were not normalized. It was suggested that further experimental studies and clinical trials should be developed to provide additional information that concerned the mechanisms of action of PBM in diabetic bone. 14 Nascimento et al. created a partial osteotomy in the femur of alloxan-induced diabetic rats. PBM [780 ± 10 infrared gallium-aluminum-arsenide (IR GaAlAs) laser, 70 mW, 0.04 cm2, laser beam surface area: 17.5 J/cm2] was performed every 48 h for 7 days. PBM significantly increased ALP and improved bone healing in the diabetic animals. 15
Although there are promising reports of in vitro and in vivo experiments, the results of other studies that concern the effects of PBM on bone healing in healthy and diabetic animals are contradictory. 16 –21
The most recent progresses in imaging technologies, such as computed tomography (CT), have made it possible to evaluate the healing process of the bones by measuring the Hounsfield unit (HU) of bone tissue. 17,22
Fracture healing could be assessed in terms of anabolic (bone formation) and catabolic (bone resorbing) reciprocation. Thus, in an anabolic response, the bones produce the sequence of steps that result in bridging of the fracture by newly emerging bones. Recently, this is a topic of interest. Catabolic action is an indispensable component of remodeling for bone during the later stages of repair, although excessive or dysregulated catabolism may impede union. Apparently, controlling catabolism by PBM in such circumstances, especially in TI DM, can be as important as an anabolic stimulator.
To the best of our knowledge, no study has investigated the effects of PBM with pulsed wave (PW) laser at an 890 nm wavelength, 80 Hz frequency, and 1.5 J/cm2 on biomechanical properties and the HU of the callus of partial tibia osteotomy in STZ- induced TI DM in rats during catabolic response. 23 Our previous study showed the positive effect of PBM with the abovementioned properties on biomechanical strength and histological properties of the callus in a complete osteotomy of the tibia in animal model at a relatively late stage of the bone healing process. 11
The present study aims to assess the effects of PBM on HU and biomechanical properties of the callus of a partial tibia osteotomy in STZ-induced TI DM (STZ-D)rats during catabolic responses.
Materials and Methods
Animals and study design
This experimental study used 20 adult female Wistar rats, 4 months of age that weighed ∼210 g. We randomly divided the rats into four groups: 1. healthy control, no TI DM, and no PBM; 2. no TI DM and PBM; 3. diabetic control, TI DM, and no PBM; and 4. no TI DM and PBM.
Each rat had a code, and the researcher was unaware of the group assignment in most cases. Rats received food and water ad libitum and were weighed on a weekly basis throughout the study. TI DM was induced in groups 3 and 4. A partial transversal standardized osteotomy was made with a drill in the right tibia of each rat. The tibias of rats from groups 2 and 4 received PBM treatments. At 30 days after the surgery, the rats were sacrificed and the right tibias were submitted to CT scanning and a three-point bending test for evaluation of the callus of the bone defect. The Medical Ethics Committee at Shahid Beheshti University of Medical Sciences, Tehran, Iran approved all study procedures (protocol no: 10397-1393-1-91-13237).
Induction of type 1 diabetes mellitus (T1 DM)
TI DM was induced in groups 3 and 4 by administration of STZ (Enzo Life Sciences, Inc., Farmingdale, NY) dissolved in sterile distilled water at a single dose of 40 mg/kg (i. p.). TI DM was defined as a blood glucose concentration greater than 250 mg/dL, which was measured from blood samples obtained from the rats' tails (Gm 300; Bionime, GmbH, Switzerland) precisely 7 days after the STZ injection. The blood glucose level and body weight were monitored once each week throughout the experiment. All diabetic rats were maintained for 30 days after administration of STZ to establish T1 DM. 19,20
Partial transversal standardized osteotomy
The right leg of anesthetized rat was shaved and aseptically prepared with povidone/iodine. The skin was cut longitudinally right below the knee on the medial side. A circular partial transversal standardized osteotomy deep to the central medullary canal was made with a low speed drill (terminal, 1.5-mm diameter; Delab; Dental Fabriktreffurt, Germany). The site was irrigated with saline solution to avoid burning. The muscles were sutured with 03 cat gut, and the skin was sutured with 04 nylon reverse cutting needle. The rats received antibiotic therapy injections with ceftriaxone at a dose of 50 mg/kg immediately before the surgery and 24 and 48 h after surgery. 20
Photobiomodulation
We used a PW laser (Mustang 2000; Technical Co., Moscow, Russia and LO7 probe) as shown in Table 1. The PBM protocol for the current study was applied successfully on the experimental rat model. We observed complete osteotomy fracture healing in healthy rats. 10 PBM began the next day after surgery and was performed on the tibias thrice per week for 30 days. In the laser-treated rats, the right tibias were completely irradiated by three laser shoots with the laser pen held perpendicular to the bone from a distance less than 1 cm. The first laser shoot was performed on the bone defect, the second laser shoot was performed at a distance of 1 cm from the center of the bone defect, and the third laser shoot was performed 1 cm from center of the bone defect (Fig. 1). All rats were sacrificed with an overdose of anesthesia 30 days after the onset of the treatments. We removed the right tibias for HU assessment followed by the three-point bending test, biomechanical examinations.
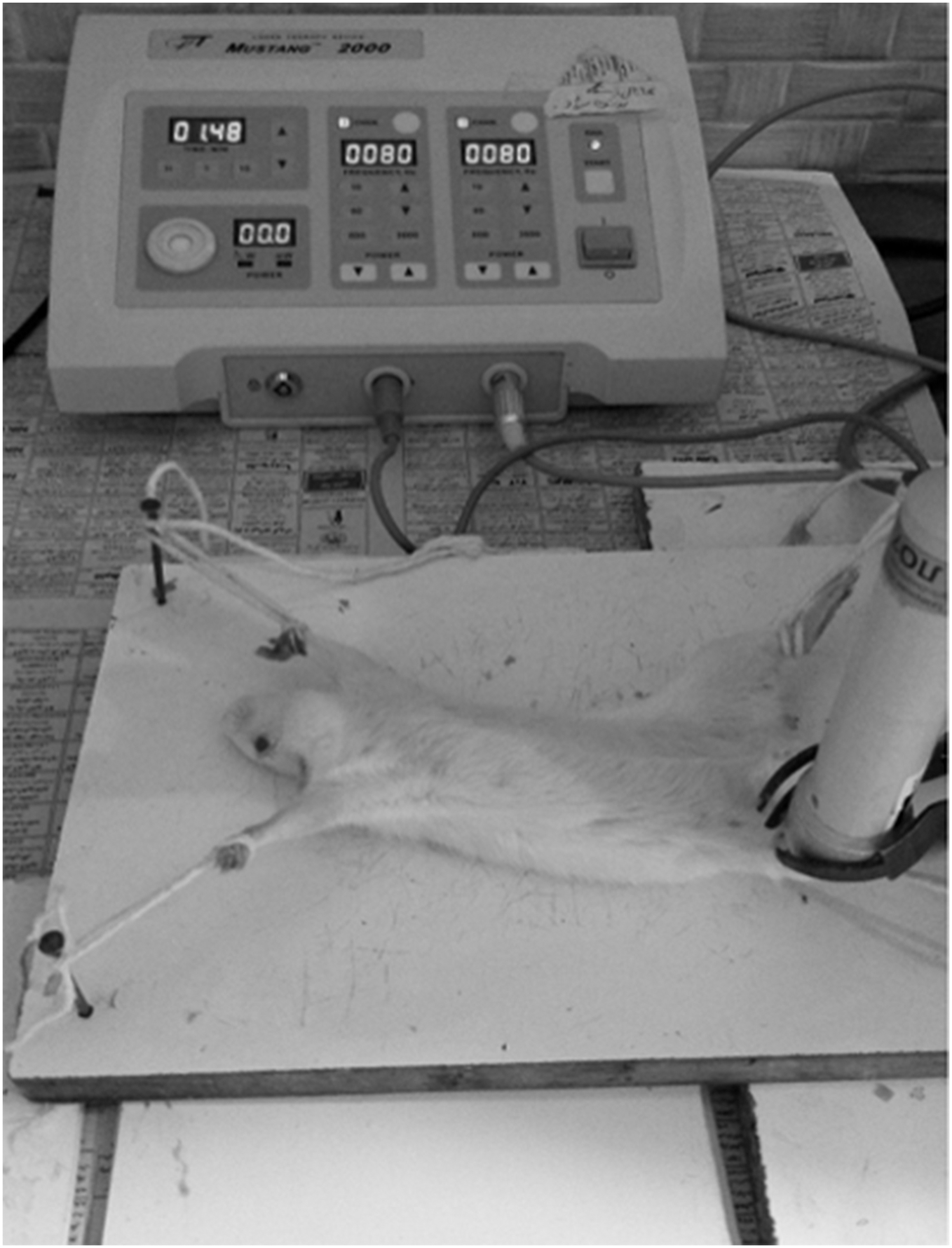
Laser radiation technique.
CT scanning
Callus densities of the bone defects were qualitatively evaluated by CT scan multislides with the following parameters: kv: 100, ma: 50, sections: 2 mm, and FOV: 240 mm (Toshiba, Aquilion 16, Japan) 30 days after partial osteotomy. We determined the callus densities of the bone defects immediately after sacrificing. All calluses were tested by an expert radiologist unaware of the group assignments. Bone and callus densities were reported in HU.
Three-point bending test
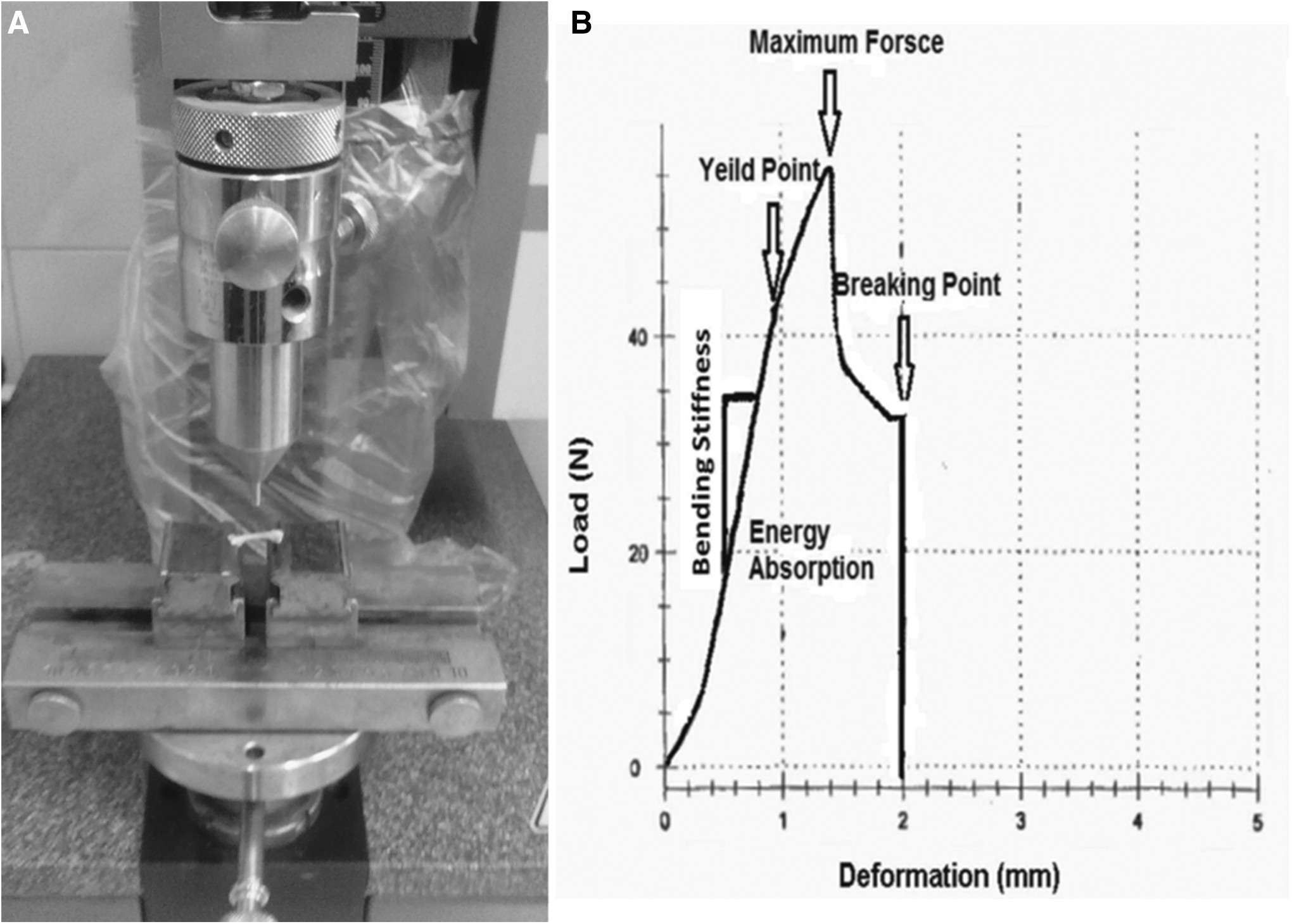
We conducted the three-point bending test to assess the biomechanical properties of five bones in each group. Bones were subjected to the three-point bending test on a material testing instrument (Zwick/Roell Group, Z 2.5 H 15WN, UIm, Germany) until fracture. The bones were placed in a similar orientation in the testing machine. We used two loading points, 20 mm apart, to mount each bone after which a press head was activated to compress the midline of the bone shaft until fracture. Compressive loading speed in the test was 0.08 mm/s for all tests. Data were recorded to the material testing instrument from the load-deformation curve, and we calculated the following values: bending stiffness (N/mm), energy absorption (N mm), maximum force (N), and stress high load (N/mm2; Fig. 2). These biomechanical properties have already been explained. 20
Statistical analysis
We used the paired Student's t-test to analyze the initial and final body weights as same as first and last blood glucose levels. Data were expressed as mean ± standard deviation. Normal distribution of data was analyzed using the one-sample Kolmogorov–Smirnov test. The analysis of variance (ANOVA) was performed to compare the changes between groups, while we used the least significant test (LSD) to identify differences. p < 0.05 was considered statistically significant.
Results
General observations
As expected, diabetic rats from groups 3 and 4 exhibited significant decreases in body weight at the end of the experiment (Table 2).
HU analysis
The ANOVA for HU density of callus produced a p value of 0.000. We observed a significant increase in the mean callus density in the healthy groups compared to the diabetic groups (LSD test, all p = 0.000). Our result indicated a significant increase in the mean callus density in group 4 (TI DM and PBM) compared to the control diabetic group (LSD test, p = 0.007). No significant differences existed in the mean callus density for groups 1 and 2. Figure 3 lists the results for the HU analysis.
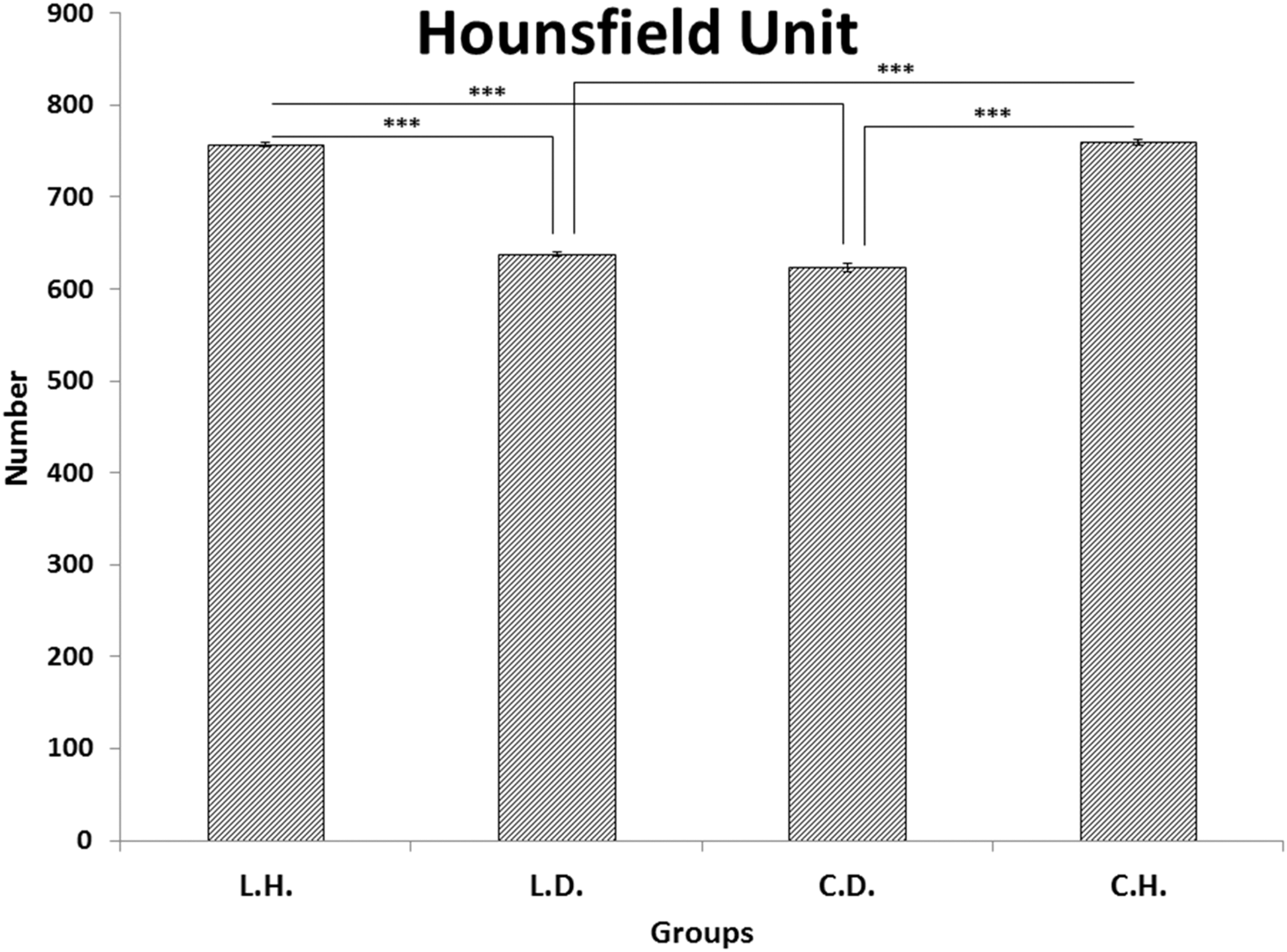
Mean ± SD of the Hounsfield units (HUs) for the study groups according to ANOVA. Groups: 1. control, no diabetes mellitus (DM), and no PBM; 2. PBM and no DM; 3. control, DM, and no PBM; and 4. DM and PBM. ***: p < 0.001. The ANOVA for the HU density of the callus produced a p value of 0.000. We observed a significant increase in the mean callus density in the healthy groups compared to the diabetic groups (LSD test). There was a significant increase in the mean callus density in group 4 compared to the control diabetic group (LSD test). ANOVA, analysis of variance; LSD, least significant test; PBM, photobiomodulation; SD, standard deviation.
Three-point bending analysis
PBM administration resulted in a significant increase only for stress high load values of the callus partial osteotomy tibia in healthy rats compared to the two control groups.
Bending stiffness, maximum force, and energy absorption
The ANOVA for bending stiffness, maximum force, and energy absorption revealed no significant differences among the experimental groups (Figs. 4 –7).
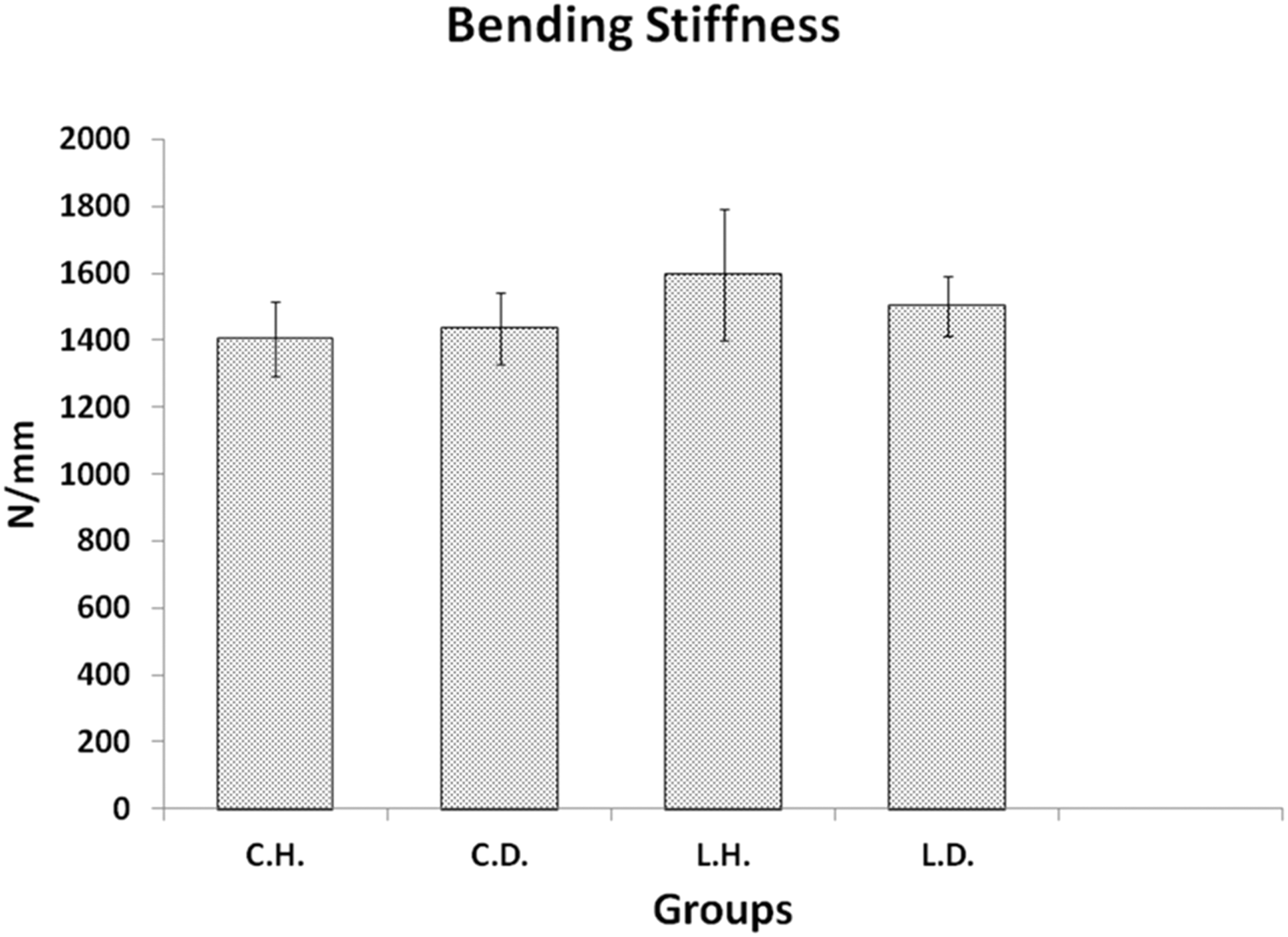
Mean ± SD of the bending stiffness compared by the ANOVA. There were no significant differences among the experimental groups.
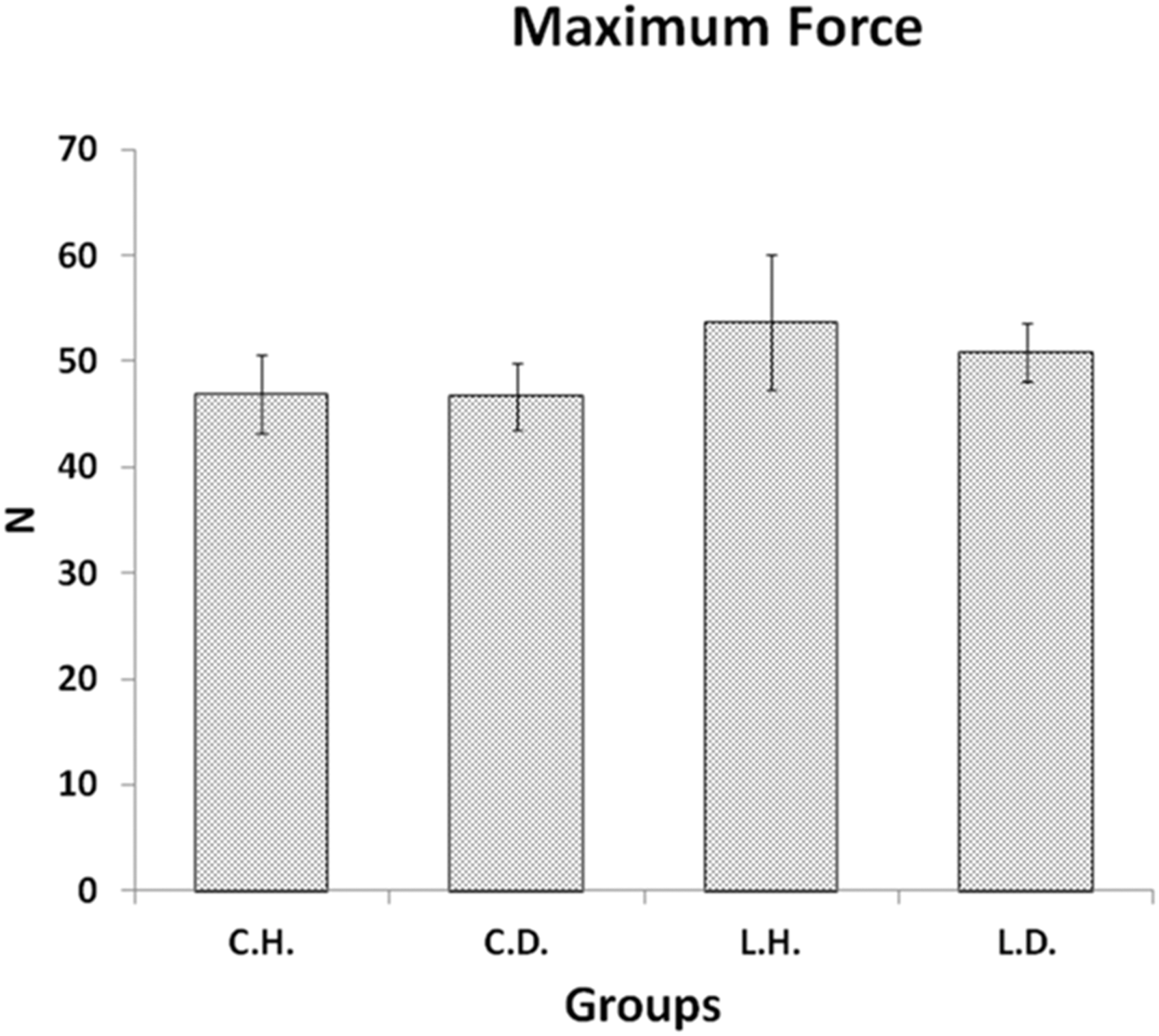
Mean ± SD of the maximum force compared by the LSD test. There were no significant differences among the experimental groups.
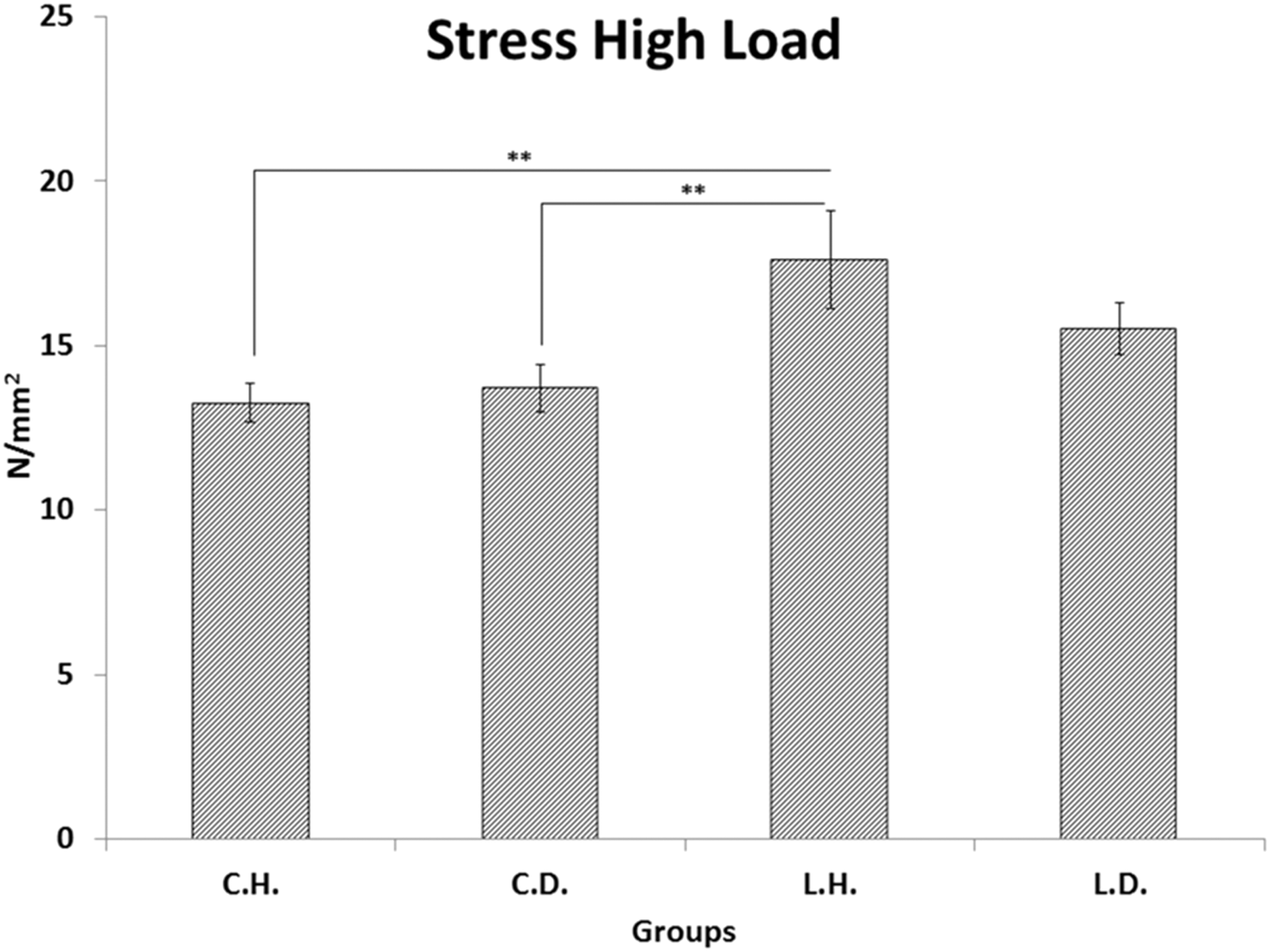
Mean ± SD of the high stress load in the groups compared by the LSD test. **p < 0.01.
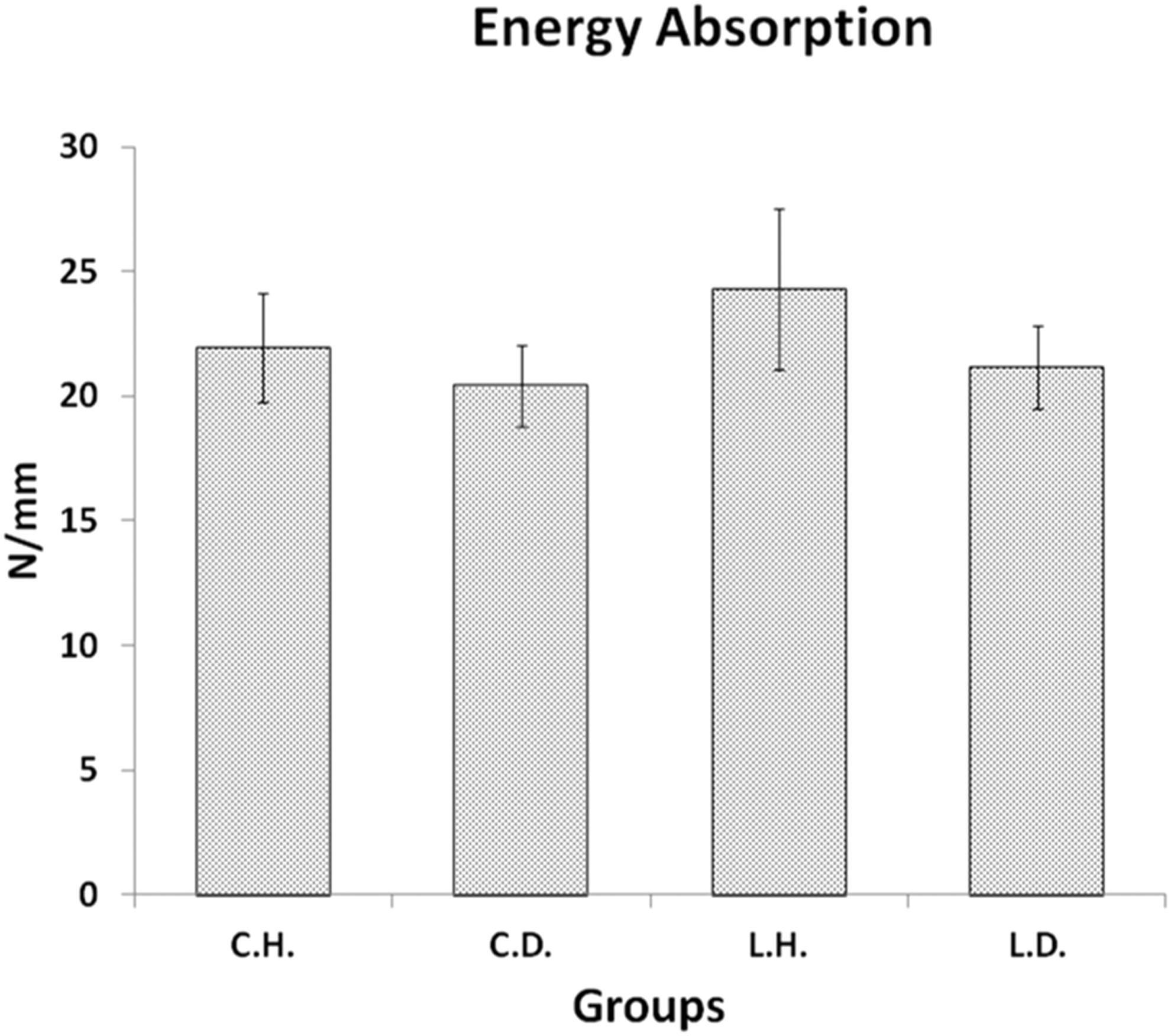
Mean ± SD of energy absorption compared by the ANOVA test. There were no significant differences among the experimental groups.
Stress high load
The ANOVA for high stress load produced a p value of 0.013. There was a significant increase in the high stress load in the group 2 compared to the healthy control (LSD test, p = 0.004) and diabetic control group (LSD test, p = 0.007; Fig. 7).
Discussion
The global increasing prevalence of DM, its complications, consequences, and treatments, led to a greater social and financial burden for society. The bones are one of many organs largely affected by DM. Bone lost is observed in TI DM, where in extreme cases this loss mirrors osteoporosis. Thus, there is a greater risk for fractures. Not only do patients with DM have increased risk for fractures but also they are more prone to impaired bone healing after a fracture. In TI DM and TII DM, the bone quality declines and eventually causes a greater risk for fracture. After a fracture, there is a delay in the healing process in patients with DM, including nonunion, which is attributed to changes in the state of bones and fracture healing. Researchers are investigating this at the cellular and molecular levels. According to the data, there is a lack of significant data in terms of fracture healing in DM patients compared to healthy individuals. However, animal models for both DM types have led to progress in research. Identifying the molecular and cellular changes in the bone in diabetes and understanding how they arise will allow for targeted intervention to improve diabetic bone fracture. 24
In the current study, we have used a biomechanical measurement of the effect of PBM on bone fracture healing, which is the ultimate proof of actual alterations in bone repair—the strength of the healed bone. 25
We observed that PBM at an 890 nm wavelength, 80 Hz pulse frequency, 1300-s duration, 8.32 W/cm2 power density, and 1.5 J/cm2 energy density significantly increased the biomechanical properties of the callus of a partial osteotomy in healthy rats. However, PBM at the abovementioned properties could not stimulate fracture healing in STZ-D rats and failed to cause any beneficial effects in the biomechanical properties of the callus from the partial osteotomy in STZ-D rats. The findings of this study supported other reports that evaluated the effects of PBM on fractures in experimental diabetic animals.
David et al. found that biomechanical properties of irradiated bones (He-Ne laser; 0, 2, or 4 Joules every other day for 2–6 weeks) were significantly weaker than the controls. 16 Kazem Shakouri reported that the calluses of healed bones in laser group (GaAlAs laser, 4 J/cm2, 780 nm, 5 min/day) were not only weaker than those of intact bones in the same group but also of those in the control group. 17 Mota et al. [indium-gallium-aluminum-phosphorus (InGaAlP), 670 nm, 30 mW, 90 J/cm2] and Magri et al. (808 nm, Ga-Al-As laser, 100 mW; 0.028 cm2; 3.57 W/cm2; 30, 60, and 120 J/cm2) reported no significant differences in biomechanical properties between control and laser groups. 18,21 Abdi et al. observed that PBM (He-Ne laser, circular beam shape, 66.8 and 369.4 J/cm2, three times per week) resulted in significantly greater bending stiffness and high stress load in the healthy group compared to the diabetic groups. 19 Javadieh et al. showed that PBM (890 nm, 70 W peak power, 3000 Hz, circular beam shape, 1 cm2 spot size, 23.3 and 11.6 J/cm2, three times per week) significantly increased bending stiffness and maximum force in diabetic rats compared with a DCG. There were no significant differences between normalized data of the biomechanical properties (stress high load). 20 Of particular relevance, these investigations assessed the strength of the uniting fracture. The current study, however, was the first experiment where both healthy and diabetic laser-irradiated fractures were subjected to biomechanical testing to determine the effect of the radiation on the strength of fracture healing. We considered this to be the most important parameter to assess the return of function to the bone in particular and the animal in general. 26
Bone strength is indirectly estimated by BMD with dual-energy X-ray absorptiometry (DXA). DXA-measured BMD accounts for 60–70% of the variation in bone strength. However, it does not capture the effects of antiosteoporotic treatment and progression of osteoporosis. Geometry and trabecular microarchitecture should also be taken into account. The assessment of the intrinsic mechanical quality of bony tissue should provide a better understanding regarding the role of tissue quality in determining bone strength. 27,28
According to previous reports, there are mechanisms behind the effect of DM on bone. Long-standing diabetes in BB rats results in severe low turnover osteoporosis related to decreased osteoblast recruitment and/or function. 29 In this regard, Verhaeghe et al. have treated diabetic rats with insulin for 12 weeks. They found increased urinary calcium excretion. Serum levels of both 1 alpha, 25-dihydroxyvitamin D3 and vitamin D-binding protein significantly decreased in diabetic rats. There was a reduced level of intestinal calbindin-D 9K with complete elimination of active duodenal calcium absorption. Trabecular bone volume decreased and the osteoblast and osteoid surfaces were less than 10% of values observed in control rats. The osteoclast surface was unchanged by DM. The bone mineral apposition rate was decreased in diabetic rats. The serum concentration of osteocalcin and bone strength also significantly decreased. 29
There is decreased osteoblast activity in a spontaneous diabetic rat model. 30 Verhaeghe et al. have performed another study in diabetic and nondiabetic BB rats using plasma osteocalcin(OC) concentrations as a marker for osteoblast activity. They observed significantly decreased OC in the DCG. 30
Diabetic animals produce sufficient amounts of immature mesenchymal tissue, but fail to adequately express the genes that regulate osteoblast differentiation, cbfal/RUNX-2 and D1 × 5, which in turn leads to decreased bone formation. 7 Parajuli et al. have evaluated exercise efficacy in TI DM. Heterozygous male and female diabetic mice and their age- and gender-matched wild-type (WT) controls were subjected to unilateral axial ulnar loading for 5 days. The heterozygous female mice reacted with improved bone formation and the loading effects did not change between heterozygous and WT females. However, loading-induced anabolic effects greatly diminished in heterozygous males. The males had reduced body weights, severe hyperglycemia, diminished bone formation, and suppressed periosteal bone appositions. These results, along with previous findings, showed the adverse effects of hyperglycemia on osteoblasts and mesenchymal stem cells. 7
The soluble form of ALP in STZ-D rats has altered kinetic properties, apparently the result of changes in metal-binding properties. 31 Fernandes et al. extracted a soluble form of ALP obtained from the osseous plate of STX-D rats, which was purified 90-fold with a yield of 26%. The calculated molecular weight (Mr) of the purified enzyme was 80,000 by denaturing polyacrylamide gel electrophoresis and 160,000 by gel filtration on Sephacryl S-300, which suggested a dimeric structure for its native form. Based on their results, it was suggested that the soluble form of ALP from STZ-D rats had its kinetic properties altered, apparently because of changes in metal-binding properties. 31
Extensive resorptive areas from osteoclast activity were observed in a DCG compared to the healthy control. In addition, the cortical bone area of control diabetic group was smaller than the healthy control group. Laser-treated animals showed increased cortical area. 14 Laser is a promising noninvasive method to stimulate osteogenesis and accelerate bone healing. 9 –11
There are four hypotheses to explain the lack of a biostimulatory effect of PBM on STZ-D rats. The energy density has been selected based on a report that indicated an 890 nm laser at 1.5 J/cm2 and 80 Hz frequency could increase bone strength in healthy rats. 10 Recently, Dadpay et al. assessed the effect of PBM in experimentally induced TI DM rats. The laser-treated wounds in the healthy and diabetic animals were submitted to an 890 nm laser with 80 Hz frequency and 0.2 J/cm2 for each point in the wound. PBM significantly increased the maximum load in wounds in both the healthy and diabetic groups. Dadpay et al. reported that PBM with a pulsed IR laser at 0.2 J/cm2 significantly accelerated wound healing in both healthy and diabetic rats. 32 Consistency, it appears that in the current study, the amount of laser energy applied to the partial bone defect (partial osteotomy) in healthy rats adequately stimulated fracture healing and significantly increased biomechanical properties compared to the control group.
The lack of beneficial effects produced by laser on STZ-D animals might be related to the laser energy density used during the treatment of diabetic rats. The amount of laser energy applied to the tissue plays a key role in the biological response. In addition, the existence of a dose–response curve is well known. 10,33 Therefore, we propose that the PBM properties used in the present experiment were not sufficient to offer an extra stimulus to accelerate bone healing in TI DM rats.
This lack of a biostimulatory effect could be due to the deep systemic effects of TI DM on the bones. The STZ model used in the current study appeared to be quite intense, such that the diabetic repairing tissues at bone defect could not respond properly to biostimulation of PBM.
In addition, the use of PBM relies to a large extent on the local effects of lights on the tissues, 34 while TI DM is a systemic disease.
Other studied supported the fourth explanation. They stated that PBM in association with bone scaffold improved biomechanical properties of tibial bone callus in osteoporotic rats. 35
The results obtained from the current work supported recent findings in our laboratory. Continuous wave PBM did not accelerate bone defect and osteochondral healing process in healthy and diabetic rats according to the biomechanical evaluation, 19,36 nor did it accelerate the burn healing process in rats. 37 –39 However, other studies demonstrated that PW laser significantly increased the biomechanical properties of complete bone osteotomy in rats 10 and stiffness of repaired osteochondral defects at the defective site in rats. 40 In addition, it accelerated the healing process in surgically induced open skin wounds in healthy, diabetic, 32,41 and burn areas in rats. 42,43 PW laser devices provide more laser (light) properties than CW laser devices. 44 It is assumed that by investigating different values of these properties, including frequency, diabetic fracture research models could be more effectively studied in these devices compared to the CW laser devices to achieve better outcomes.
Treatment with the 80-Hz PW laser significantly increased the biomechanical property (stress high load), HU of the callus, and the partial osteotomy of the tibia in healthy rats compared to the control rats. However, there was no significant increase in the biomechanical properties of laser-treated type I diabetic bone defects compared to the DCG. Clearly, further studies would be needed to determine the optimal properties for PBM for bone repair in diabetic animal models.
Footnotes
Acknowledgments
The authors extend their sincere appreciations to the late Mrs. Jamileh Rezaei. This article is financially supported by the Research Department at Shahid Beheshti University of Medical Sciences, Tehran, Iran (Grant No. 10397-1393-1-91-13237).
Author Disclosure Statement
The authors declare no conflicts of interest or financial relationships to any products involved in this study.