
Abstract
Osteoporosis
O
Wright et al. reported that there were >99 million U.S. adults over the age of 50 in 2010 in the United States. Based on an overall 10.3% prevalence of OP, Wright et al. predicted that in 2010, 10.2 million older adults had OP. The overall low bone mass (LBM) prevalence was 43.9%, from which they estimated that 43.4 million older adults had LBM. These researchers predicted that 7.7 million non-Hispanic white, 0.5 million non-Hispanic black, and 0.6 million Mexican American adults had OP. A total of 33.8 million Caucasians, 2.9 million African Americans, and 2.0 million Hispanics had LBM. Therefore, OP and LBM at the femoral neck or lumbar spine affected an estimated 53.6 million older U.S. adults in 2010. Although Caucasian women comprised the majority of individuals with OP or LBM, a substantial number of men and women from other racial/ethnic groups also had osteoporotic bone mineral density or LBM. 3 Hip fractures from OP have a large economic impact. The cost of osteoporotic fractures in the United States was estimated at $19 billion in 2005. 4
OP is primarily a metabolic bone disease that is primarily caused by changes in lifestyle, increased age, and underlying diseases. Chronic inflammatory diseases, metabolic disorders, and nutritional deficits increase the risk for OP. Secondary OP is caused by endocrinological disorders and medications such as glucocorticoids. 5 Currently, most drugs decrease bone loss by reducing bone resorption; however, newer therapies may enhance bone mass by directly increasing it. Current alternative treatments include bisphosphonates (BP), calcitonin, selective estrogen receptor modulators, and inhibitors of the RANK pathway. However, adequate calcium and vitamin D levels are prerequisites. Newer drugs, the targets of which are osteoclasts, such as cathepsin K and c-Src kinase, are not completely clinically approved.
The therapies that target osteoblasts act through the Wnt-β catenin signaling pathway and include Dkk-1 inhibitors and sclerostinantagonists. 6 BPs are the drugs of choice for most patients with OP. Alendronate and risedronate are FDA approved for the prevention of bone loss in menopausal women, treatment of postmenopausal OP, and prevention and treatment of glucocorticoid-induced OP. 7 However, serious adverse effects associated with BPs include BP-related osteonecrosis of the jaw 8 and gastrointestinal effects. 9 Prolonged BP therapy may suppress bone remodeling to the extent that normal bone repair is impaired, which results in an increased risk of fracture. 10 At present, most marketed drugs decrease bone loss by diminishing bone resorption. The upcoming therapies may directly increase bone mass, as in the case of parathyroid hormone. 6
However, due to daily injections and expense of treatment, parathyroid hormone is not the best candidate as a first-line therapy for OP. 11 This review article intends to present a method that improves bone quality through stimulation of osteoporotic mesenchymal stem cells (MSCs) by low-level laser therapy (LLLT).
Prall et al. reported that osteoporotic MSCs have reduced osteogenic differentiation when cultured in their standard differentiation media. 12 Osteoporotic MSCs had adequate induction of osteogenic differentiation due to BMP-2 stimulation. Therefore, BMPs-2 and −7 might represent effective therapeutic agents for the treatment of fractures in patients with OP. However, side effects, such as life-threatening inflammatory swelling and promotion of adipogenesis, are apparent. 13
Due to the growing burden of musculoskeletal diseases and injuries on healthcare, and side effects of some therapeutic pharmacological agents and growth factors, there is a growing need for safe, available, and cost-effective therapies. OP has a remarkable impact on the quality of life of patients and costs hundreds of hours of inpatient and outpatient hospital services and resources. There are growing interests in the use of the therapies such as vibration therapy, low-magnitude high-frequency vibration, mechanical stimulation, and LLLT to improve bone structure and muscle performance in a variety of patients. Anabolic effects of loading on the musculoskeletal system is a necessity for promoting bone strength, especially in frail individuals unable to do normal physical activities and the techniques mentioned could be considered nonpharmacological analogues of physical activity. These techniques have been promising in certain musculoskeletal diseases and have had positive effect on both MSCs differentiation and osteogenesis. 14 –16
In an OP animal model, researchers observed an association between OP and a reduction in the number and growth of bone marrow (BM) MSCs. The BMMSCs showed impaired engraftment to the fracture area and osteoinduction, in addition to disordered bone regeneration. 17,18
The application of LLLT has recently extended to beyond its traditional domains in medicine such as wound repair and inflammatory skeletal conditions. 19 One of these novel application areas is using LLLT for biostimulating and increasing proliferation rate of cells in vitro. In the next paragraph, biostimulatory effect of LLLT on bony cells in vitro will be explained in more detail.
Low-Level Laser Therapy
Light therapy is based on the effects of light energy on the cell metabolism of living systems. LLLT has a photochemical effect comparable to photosynthesis in plants in accordance with the amount of absorbed light and it exerts a chemical change. 20 The cellular and molecular mechanism of LLLT suggests that photons are absorbed in the mitochondria by cytochrome-c oxidase. 17 For example, the Helium–Neon (He-Ne) red laser elicits a cellular response to light. LLLT stimulates ATP production. Low levels of free radicals or reactive oxygen species activate transcription factors such as nuclear factor kappa B (NF-κB) to induce transcription of numerous products responsible for the beneficial effects of LLLT. 20
Incerti Parenti et al. used a diode laser with the specifications of 915 nm at 1, 5, 10, 20, and 50 J/cm2 to irradiate Saos-2 human osteoblast-like cells. They assessed cellular morphology, viability, and cytotoxicity. DNA content and release of vascular endothelial growth factor (VEGF), receptor activator of NF-κB ligand (RANKL), and osteoprotegerin (OPG) were evaluated. The results indicated that viability was modulated by the laser in a dose-dependent manner. The 10 J/cm2 dose induced a biostimulatory response, whereas 20–50 J/cm2 doses had bioinhibitory and cytotoxic effects. DNA content increased at the 10 J/cm2 dose, but decreased at 50 J/cm2. They observed a rapid, transitory trend toward an increased RANKL/OPG ratio and the tendency toward a delayed increase in VEGF release at the 1–10 J/cm2 doses. Incerti Parenti et al. suggested that additional studies should be performed with the biostimulatory dose of 10 J/cm2 to establish an ideal treatment regimen in the laboratory and clinical settings. 21
Oliveira et al. compared the influence of LLLT and light-emitting diode (LED) light therapy at 10 and 50 J/cm2 on human osteoblast proliferation and differentiation. The involvement of extracellular signal-regulated kinase (ERK) signaling on proliferation was also investigated. The researchers evaluated its activation during proliferation under different light therapies by Western blot analysis and measurements of carboxyfluorescein diacetate succinimidyl ester (CFSE)-based osteoblast proliferation in the presence or absence of the ERK-specific inhibitor. Osteogenic differentiation was evaluated through in vitro mineralization and gene expression of type I collagen (COL1A1), and osteonectin [secreted protein acidic and rich in cysteine (SPARC)] by real-time polymerase chain reaction. The results showed increased numbers of viable cells and an increased proliferation rate after radiation independent of the LLLT type.
However, only red laser irradiation at 10 J/cm2 and the infrared laser at both doses induced ERK1/2 activation. LED did not induce ERK1/2 activation. The ERK inhibitor prevented LLLT-induced proliferation. Red laser stimulation resulted in upregulated COL1A1 gene expression. They observed upregulation of SPARC with infrared stimulation. However, both LED doses increased COL1A1 and SPARC expressions. All LLLT treatments increased mineralization in a dose- and time-dependent manner. LLLT and LED differently modulated the metabolism of human osteoblasts. The increased proliferation occurred by mechanisms dependent and independent of ERK signaling activation, and osteogenic differentiation markers. 22
The cell culture is one of the most useful techniques for production of viral vaccines and hybrid cell lines. However, the growth rate of some of the much-needed mammalian cells is slow. LLLT can enhance the proliferation rate of various cell lines. Cells such as fibroblasts and osteoblasts grow when exposed to laser irradiation. Studies of the effects of LLLT on cell cultures report enhanced ATP, RNA, and DNA synthesis in SCs and other cell lines. LLLT has been shown to improve cell proliferation without causing any cytotoxic effects. 20
Mitochondria play a central role in MSC metabolism because not only they are sites of cellular respiration and energy production, but also they are the principal photoacceptors present inside cells. MSC differentiation is associated with an increase in mitochondrial content and activity, which suggests that LLLT and its effect on mitochondria is highly beneficial to MSC differentiation and proliferation. 19 In the next part, LLLT effect on MSCs is briefly reviewed.
LLLT Effect on MSCs
MSCs have the ability to generate cells of connective tissue lineages, including bone and cartilage. These cells have created tremendous interest due to their potential use in tissue engineering and regenerative medicine. 23 Stimulation of SCs by LLLT has been examined in numerous contexts. LLLT stimulates the growth, proliferation, and differentiation of SCs both in vitro and in vivo, which is essential for experiments related to disease control in humans. 24 –26 Table 1 shows the important specifications of laser-treated MSCs.
LLLT, low-level laser therapy; MI, myocardial infarction; MSC, mesenchymal stem cell.
Wu et al. used murine BMMSCs to investigate the potential mechanism for LLLT-mediated enhancement of bone formation. BMMSCs received daily irradiation with a gallium–aluminium–arsenide (GaAlAs) laser at energy densities of 0, 1, 2, or 4 J/cm2. The lactate dehydrogenase assay showed no cytotoxic effects of LLLT on the BMMSCs. The 4 J/cm2 dose of LLLT significantly promoted BMMSC proliferation and osteogenic differentiation, and moderately increased expressions of osteogenic markers. Further tests demonstrated that LLLT regulated insulin-like growth factor 1 (IGF-1) and bone morphogenetic protein 2 (BMP-2) signaling to promote cell proliferation and/or osteogenic differentiation. 35
Leonida et al. examined the effects of Nd:Yag laser radiation on proliferation and differentiation of human BMMSCs (hBMMSCs) induced into osteoblast lineage in a scaffold. They used two laser protocols with the Nd:Yag laser. One group received laser treatments at 15 Hz, 100 mJ, and 1.5 W, whereas the other group received laser treatments at 15 Hz, 150 mJ, and 2.25 W. The third group received no laser treatment (control group). Leonida et al. found that after 7 days, proliferation significantly increased in the laser-treated scaffolds compared with the control. They observed an increase in differentiation in the laser-treated groups. The researchers concluded that LLLT might lead to reduced healing times and potentially reduce the risks of failure. 37 Soleimani et al. cultured hBMMSCs and induced differentiation in osteoblasts treated with LLLT. They used a laser (GaAlAs laser, 810 nm, and 2 and 4 J/cm2) on days 1, 3, and 5 of the differentiation process of hBMMSCs induction to osteoblasts. The hBMMSCs differentiation to osteoblasts was examined according to alkaline phosphatase (ALP) activity. Soleimani et al. reported that laser significantly stimulated hBMMSC proliferation compared with the control group. They observed significant enhancement of ALP activity in the irradiated hBMMSCs that differentiated to osteoblasts. 40
Li et al. treated BMMSCs with LLLT (LED array, 630 nm, 5 and 15 mW/cm2, and 2 and 4 J/cm2). They evaluated the proliferation, clonogenic potential, and osteogenic differentiations of the BMMSCs after laser radiation. Li et al. observed enhanced BMMSC growth following multiple laser exposures at 15 mW/cm2 and 4 J/cm2. The number of colony-forming unit fibroblasts increased in the laser-treated group under the optimal parameters. Laser treatment during osteogenesis significantly increased expressions of ALP and osteocalcin. 41 In the next paragraph, we postulated that transplanting the in vitro cultured recovered osteoporotic BMMSCs into bony sites at risk of OP or fracture, could improve bone structure and enhance biomechanics. The ability of LLLT to stimulate MSCs suggests that osteoporotic MSCs may respond well to LLLT with improved bone quality and accelerated fracture healing.
Transplantation of Cultured BMMSCS
Recently, transplantation of in vitro cultured BMMSCs with an appropriate osteogenic phenotype into sites at risk for development of osteoporotic bone has resulted in improved bone structure and enhanced biomechanical properties. 47 Allogeneic MSCs are responsible for exerting a wide range of local, predominantly suppressive signals that affect innate and adaptive immunity. Nonetheless, these cells also maintain a degree of immunogenicity under certain conditions, which may limit their longevity and reduce their beneficial effects. 48 Taken together, laser-treated osteoporotic autologous BMMSCs may represent a promising therapeutic agent to protect bones of patients with OP and prevent fractures.
We have recently published a study about the effects of LLLT on viability and proliferation rate of healthy and ovariectomy-induced OP (OVX)-BMMSCs in vitro. The results showed that healthy BMMSCs responded optimally to infrared laser (810 nm) after three laser shots. In that study, OVX-osteoporotic BMMSCs responded optimally to the He-Ne laser with a one-time laser radiation application. We concluded that the effect of LLLT depended on the physiological state of the BMMSCs, type of the laser, wavelength, and number of laser sessions. These results might be applicable for regenerative medicine. Therefore, we hypothesized that transplantation of in vitro laser-treated autologous cultured osteoporotic BMMSCs with an appropriate osteogenic phenotype into sites at risk for developing osteoporotic bone might improve bone structure and enhance biomechanics. 28
Autologous osteoporotic MSCs have been successfully restored by laser treatment 28 alone and in combination with other treatments such as catabolic agents. In future studies, recovered MSCs should first be differentiated into an osteoblast cell line, after which they could be transplanted into animal models of OP. This technique might improve bone quality and structure (Fig. 1).
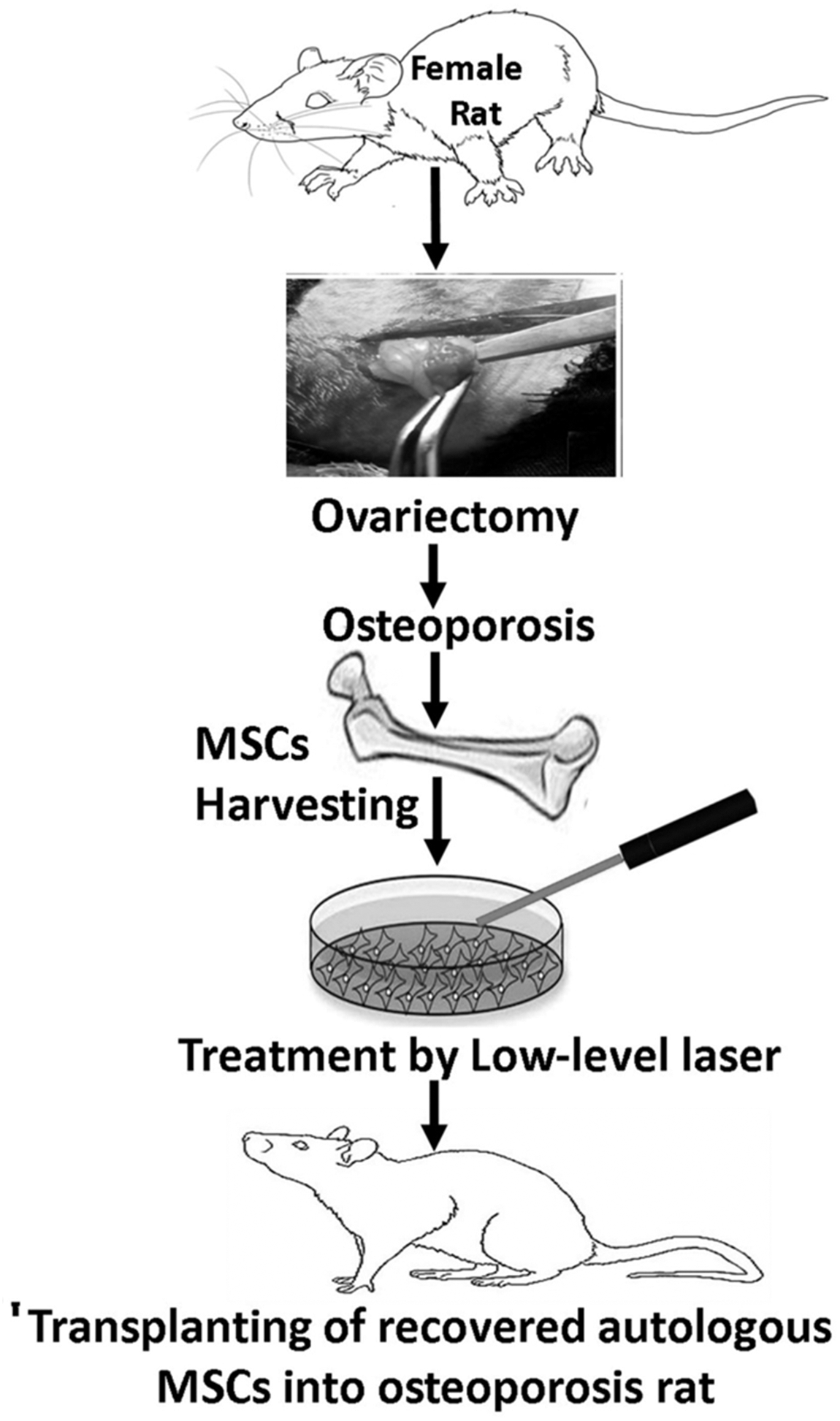
Treatment steps of autologus bone marrow mesenchymal stem cells and transplantation into an animal model of osteoporosis. MSCs, mesenchymal stem cells.
Regenerative medicine may provide disease-free, functional tissues and organs that would enhance patient quality of life. Introduction of autologous SC therapy in combination with regenerative medicine can increase treatment options for more diseases. 49 However, an extensive amount of research should be undertaken in an attempt to understand the underlying mechanisms and validate the effectiveness and feasibility for clinical applications of LLLT treatment for MSCs to regenerate bone mass in OP patients.
Despite the clinical potential of stem cell-based medicinal products, potential and unanticipated risks exist. These risks deserve a thorough discussion within the perspective of current scientific knowledge and experience. Evaluation of potential risks should be a prerequisite to clinical use of stem cell-based medicinal products. Recent progress in using stem cells for tissue repair and functional restoration has provoked much attention due to its potentials in treatment of many diseases, including OP. However, besides the advantages, there are some limits and drawbacks of currently used stem cell therapy in regenerative medicine, which will be discussed in the following paragraph.
The Limits and Potential Drawbacks of Cell Therapy
The risk profile of SC-based medicinal products depends on numerous factors—the type of SCs, their differentiation status and proliferation ability, method of administration, intended site, in vitro culture and/or other manipulation steps, irreversibility of handling, need/opportunity for simultaneous tissue regeneration in case of irreversible tissue loss, and long-term survival of transplanted SCs. Altogether, these issues regulate the risk profile linked with the SC-based medicinal product. Those identified risks in clinical practice or possible/theoretic risks observed in animal studies include tumor formation, unwanted immune response, and the transmission of adventitious agents. Currently, there is no clinical experience with pluripotent SC (i.e., embryonal SCs and iPSCs).
Based on their characteristics of unlimited self-renewal and a high proliferation rate, the potential dangers of a product that contains these SCs include the risk of tumor formation, which is unacceptable. In contrast, the numerous small-sized clinical trials that use MSCs in regenerative medicine have not reported major health concerns, which suggest that MSC therapies could be relatively safe. 45 Some studies have shown that SC therapy would be cost effective if researchers considered some issues in their treatments. 47,48 Regenerative medicine and cell therapy for diseases, such as intervertebral disc degeneration, hemato-oncologic malignancies, melanomas, and prostate carcinoma, have progressed to the clinical trial stage. 53,54
Conclusions
However, side effects such as life-threatening inflammatory swelling and promotion of adipogenesis are apparent. 13
Due to the growing burden on healthcare costs of musculoskeletal system disease and injury, and side effects of pharmacological agents and growth factors, there is a growing need for safe, cost-effective and simple therapies. OP severely impacts on the quality of life and result in hundreds of hours of hospital time and resources. There is a growing interest in the use of the therapies such as vibration therapy, low-magnitude high-frequency vibration, mechanical stimulation, and LLLT to improve bone structure and muscle performance in a variety of different patient groups. Table 1 lists potential limitations in a number of studies. 27 –46 In this review we have suggested that all available wavelengths and energy densities for red and infrared lasers, along with other techniques should be used to assay cellular proliferation and viability. These studies must clarify the most appropriate LLLT parameters that stimulate healthy and osteoporotic MSCs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.