
Abstract
Introduction
P
The hydrogen peroxide released from bleaching agents diffuses through the enamel and dentin and penetrates the dental pulp. 3 Inside the pulp chamber, hydrogen peroxide may be toxic to dental pulp cells by inducing oxidative stress. 4 –6 Tooth sensitivity is the most common clinical consequence of dental bleaching. 1 It is reported an incidence rate of 67–87% of tooth sensitivity after tooth bleaching. 1,7,8 The intensity of the adverse effects is directly related to the concentration of hydrogen peroxide in the gel and also to the number of bleaching sessions. 4 –6 In addition, the thinner the enamel/dentin thickness, the more intense the tooth sensitivity will be and more severe damage to the pulp tissue can occur. 9 –11
Some therapies have been proposed to prevent or reduce the pulpal damage and the consequent tooth sensitivity caused by tooth bleaching. A prebleaching administration of anti-inflammatory drugs and topical application of sodium fluoride and potassium nitrate desensitizing agents, as well as the use of antioxidant molecules, have been proposed in literature. 2,8,12 –16 Since the pathway for pulp tissue damage following tooth bleaching involves oxidative damage to pulp cells, therapies using antioxidant agents have been recognized as an interesting alternative for preventing the occurrence of conditions leading to intense oxidative stress. 1,13 Some in vitro studies have shown that antioxidant molecules, such as alpha-tocopherol and ascorbic acid, were capable of preventing hydrogen peroxide-mediated pulp cell damage in vitro. 1,2,13 These antioxidant agents may inactivate the extracellular ROS from bleaching gels, as well as the intracellular ROS released by cells undergoing oxidative stress. 1,2,13
Photobiomodulation with low-power laser is used in a variety of areas of medicine with the aim of injured tissue regeneration. 17 This therapy results in analgesic, anti-inflammatory, and biomodulatory effects. 4,18 The laser light within the red visible and near-infrared wavelengths corresponds to the energy absorption spectrum of the respiratory chain components. Under stress conditions, photobiomodulation increases the cellular metabolism. 5,18,19 Some publications showed a direct correlation between photobiomodulation and antioxidant cascade activation. 17,20 –23 Zhang et al. 23 revealed that 111 genes were upregulated by the red light irradiation and can be grouped into 10 functional categories. Most of these genes directly or indirectly play roles in the enhancement of cell proliferation and suppression of apoptosis. Some of these genes were related with regulation of antioxidant system. Dantas et al. 17 showed that a 780 nm low-power laser (10 J/cm2, 40 mW) was able to compensate the cytotoxic effect of 35% hydrogen peroxide on human pulp fibroblasts in vitro. On the contrary, Lima et al. 6,9 showed an opposite result in vitro, with odontoblast-like cells, whereas low-power laser was not able to compensate the detrimental effects of hydrogen peroxide. In vitro studies usually show us valuable information; however, the results cannot be predictive to what really occurs in vivo. Controlled clinical trials should be developed to verify the effects in vivo.
In a randomized placebo clinical trial, Moosavi et al. 24 showed positive results in a study that tested photobiomodulation on tooth sensitivity induced by in-office bleaching with the parameters of 660 or 810 nm, 200 mW, 15 sec, and 12 J/cm2. Irradiation was performed after tooth bleaching and at 24 h after therapy; pain level was significantly lower in the laser group at 810 nm in comparison to the laser group at 660 nm and placebo group.
As the study cited above was the first clinical trial published in this scenario, further studies should be performed to analyze other parameters and techniques of photobiomodulation application to be applied in prevention of tooth sensitivity after bleaching. The aim of the present study was to analyze through a randomized placebo blind study, three protocols of photobiomodulation: before bleaching, after bleaching, before and after bleaching in the prevention of tooth sensitivity through the following parameters: 40 mW, 780 nm, 10 J/cm2.
Materials and Methods
This phase I clinical trial was conducted according to the Declaration of Helsinki and was approved by the Ethics Committee of the School of Dentistry, University of São Paulo (No. 34935414.6.0000.0075). Each patient signed a written informed consent to participate in the study. This study was conducted as a randomized, placebo blind clinical trial and 50 patients were enrolled.
• Inclusion criteria: Good general health, good oral hygiene. Volunteers should be between 18 and 40 years.
• Exclusion criteria: Patients who use corticosteroids, analgesics, or anti-inflammatory medications before, during, or after dental bleaching were excluded. Patients who have in the superior and inferior incisors, canine, and premolar teeth (1) endodontic treatment, (2) composite fillings, (3) laminates, (4) metallic or ceramic crown, (5) caries, (6) cracks, (7) erosion, (8) abrasion, (9) abfraction, (10) dentinal hypersensitivity, and (11) periodontal disease were excluded from the study.
Study groups
Volunteers were randomly divided into the following groups (n = 10): (1) control, (2) placebo/no irradiation, (3) laser before bleaching), (4) laser after bleaching, and (5) laser before and after bleaching. Randomization was performed using the software:
In-office dental bleaching
Before in-office dental bleaching, volunteers underwent prophylaxis with water slurry of pumice and rubber prophylaxis cup. All volunteers were submitted to dental bleaching (superior and inferior incisors, canine, and premolars), performed by two researchers (K.M.R. and A.P.C.C.). The protocol applied is described below: Previously, gingival tissue was protected using a light-cured resin dam (Top Dam®, FGM, Joinville, SC, Brazil). A 35% hydrogen peroxide gel (Whiteness HP®, FGM, Joinville, SC, Brazil) was applied to incisors, canine, and premolars of both arches in a total time of 45 min, according to the manufacturer's instructions. Bleaching gel was refreshed every 15 min. After each 15-min dental bleaching, gel was removed and teeth were washed with water and dried with air spray. Two bleaching sessions were performed with a 1-week interval.
Tooth sensitivity assessment
Patients were asked to record tooth sensitivity before, immediately after, and every seven consecutive days after each bleaching session using the following scale: 0 = no tooth sensitivity, 1 = gentle sensitivity, 2 = moderate sensitivity, and 3 = severe sensitivity. Three researches were responsible for patient's sensitivity report collection (K.M.E., A.P.C.C., and S.R.B.).
Treatments applied
Volunteers received treatment according to the allocated group: • Control: Only in-office dental bleaching was performed. Patients were not submitted to additional treatments. • Placebo: Low-power laser (MMOptics ®, Sao Carlos, Brazil) was positioned perpendicularly, in contact, on each tooth during 10 sec per point in two points (Fig. 1). The first point was positioned in the middle of the tooth crown (Fig. 1A) and the second in the periapical region (Fig. 1B). Irradiation was performed with switched off equipment. • Laser before bleaching (n = 10): Low-power laser (MMOptics, Sao Carlos, Brazil, laser spot size area of 0.04 cm2) was used immediately before dental bleaching with the parameters of 780 nm, 40 mW, 10 J/cm2, 0.4 J per point, perpendicularly, in contact, on each tooth during 10 sec per point in two points (Fig. 1). The first point was positioned in the middle of the tooth crown (Fig. 1A) and the second in the periapical region (Fig. 1B). A power meter was used to check the power output. Details of photobiomodulation parameters applied are described in Table 1. • Laser after bleaching (n = 10): Low-power laser was used immediately after dental bleaching in the same way cited in the group, laser before bleaching. • Laser before and after bleaching (n = 10): Low-power laser was used immediately before and after dental bleaching in the same way cited in the group, laser before bleaching.
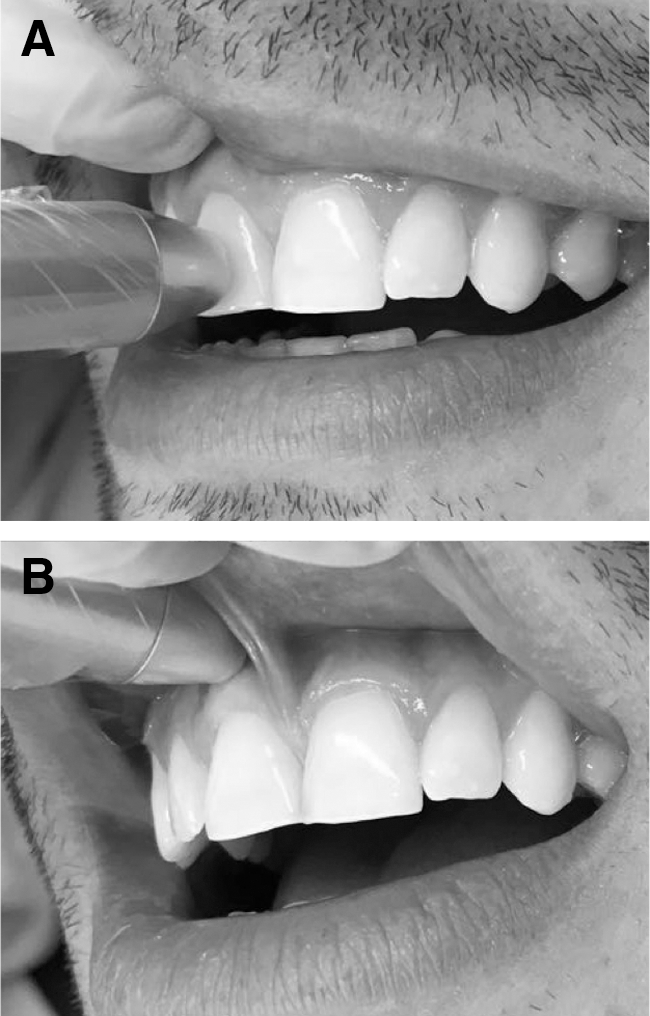
Points of photobiomodulation application.
Statistical analysis
The comparison of the sensitivity between groups was performed using the nonparametric Kruskal–Wallis test, with a significance level of 5%.
Results
The study was conducted from September 2014 to March 2015. A flow chart of the progress of this randomized placebo blind study, according to the CONSORT statement, is included (Fig. 2). 25 The baseline characteristics from 50 patients enrolled in this study are given in Table 2.
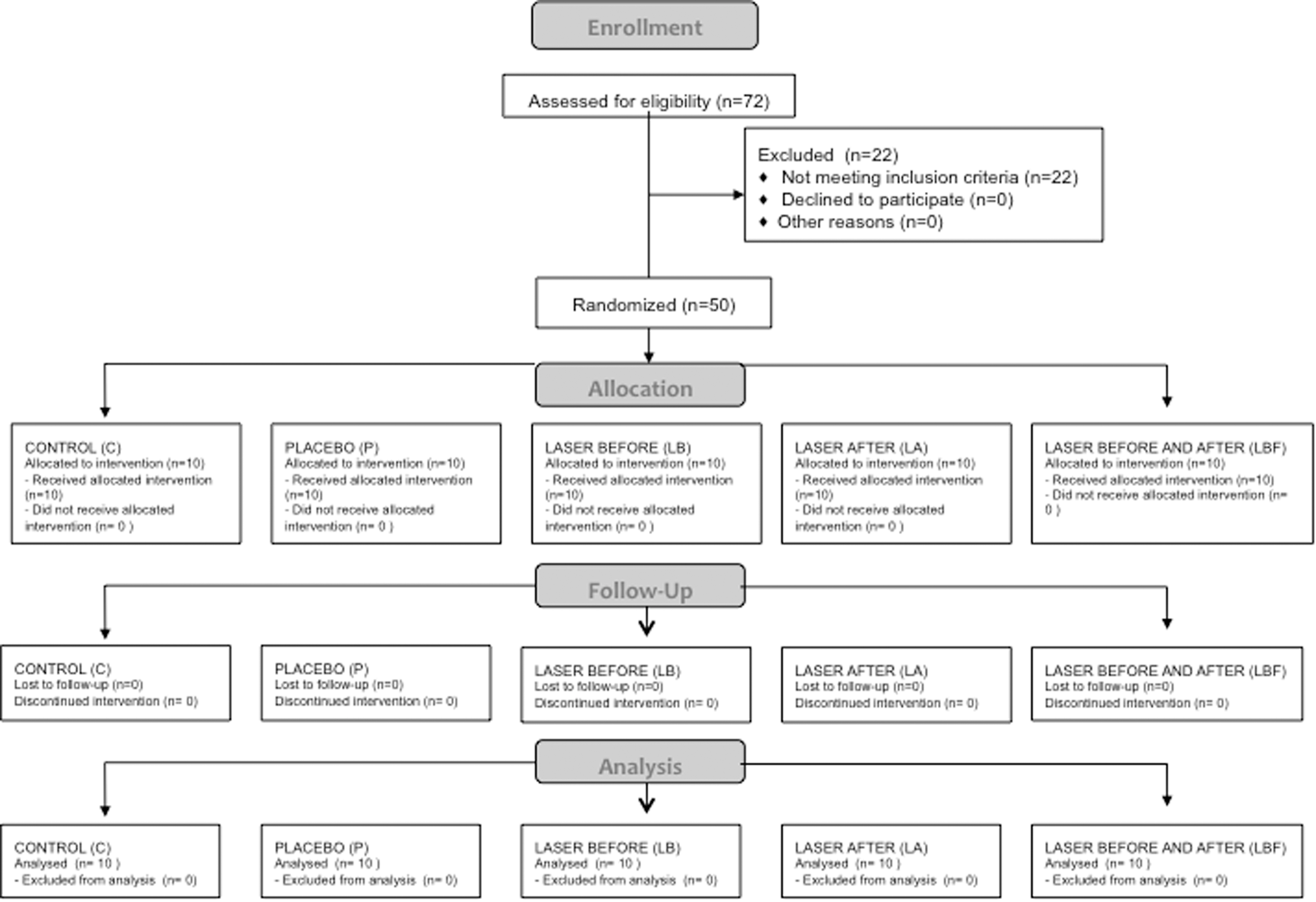
Consort flow diagram. C, control; LA, laser after; LB, laser before; LBF, laser before and after; P, placebo.
There was no statistical difference between groups after both bleaching sessions. Mean and standard deviation (SD) from sensitivity recorded by each group after first and second sessions are described in Tables 3 and 4, respectively.
SDs, standard deviations.
Discussion
The present controlled clinical trial investigated the photobiomodulation protocol of 780 nm, 40 mW, 10 J/cm2 in the prevention of tooth sensitivity caused by in-office dental bleaching. This photobiomodulation protocol was adopted once, in vitro, it showed positive results, which could compensate the deleterious effect of 35% hydrogen peroxide on human pulp fibroblasts. 17 In this clinical trial, three moments of laser application were tested: before in-office bleaching, after in-office bleaching, and both periods. Two sessions of in-office bleaching were performed and patients reported the intensity of sensitivity before bleaching, immediately after the end of the bleaching procedure, and every seven subsequent days.
Photobiomodulation has shown positive results in alleviating oxidative stress in different research and clinical models, for example, in chronic inflammation, diabetes, and chronic spinal cord injury. 8,20,21 In the present study, it was chosen to perform dental bleaching without any light activation, to avoid interference from other light sources than the low-power laser used. It is common to use LED light to activate dental bleaching. However, literature suggests that LED light can also provide some photobiomodulation effect in tissues. 26 So, for this reason, no LED light was used during the bleaching procedure in this study. The degree of final bleaching color was not evaluated, as it was not the objective of the study; however, all patients from all groups were satisfied with the final results.
Photobiomodulation applied after in-office dental bleaching has already been tested with the parameters of 660 nm, 780 nm, 200 mW, and 12 J/cm2 by Moosavi et al. 24 The authors did not find any positive result at 660 nm. At 780 nm, only after 24 h, after bleaching laser application in the cervical area of the crown could reduce the intensity of tooth sensitivity after in-office bleaching.
The present study tested the same bleaching protocol of the Moosavi study (2016), 24 where three changes of 15 min of bleaching gel was performed per session, totalizing 45 min/session. Our results did not show any statistically significant difference among the groups. The results varied between none, gentle, and moderate sensitivity. None of the patients has reported severe sensitivity.
Probably the difference in parameters applied between the present study and the study by Moosavi et al., 24 as power and energy density could be speculated as one reason for the differences in results found. Moosavi et al. 24 applied a power of 200 mW, and the present study used 40 mW. Maybe for this kind of application, a higher power setting should be chosen. The same observation can be speculated for energy density, as we used 10 J/cm2 and Moosavi applied 12 J/cm2. 24
Another difference between the present study and the study by Moosavi et al. (2006) 24 was how tooth sensitivity was measured. In the study by Moosavi, sensitivity was measured with a visual analogue scale, which consists of a 100 mm horizontal line with 0 (the left side) indicating no pain and 100 mm representing the worst pain (the right side). In the present study, patients should give note to the sensitivity in a fixed score mode among four options: 0 = no tooth sensitivity, 1 = gentle sensitivity, 2 = moderate sensitivity, and 3 = severe sensitivity. Probably the latter method of measuring tooth sensitivity led to a higher variation. So, in the present study, it is hypothesized that due to the higher SD found, no statistically significant difference among groups was obtained. Further studies should be carried out to verify the most appropriate method to verify tooth sensitivity and photobiomodulation in dental bleaching studies, once this kind of methodological study cannot be found in literature.
In addition, pain is a subjective experience and its threshold varies between patients. Another reason for the high variation found can be related to individual tooth variations between patients, for example, enamel and dentin thickness, variation of hydrogen peroxide diffusion/teeth. So, it is expected to have high pain variation reported by patients.
This preliminary study was conducted between September 2014 and March 2015. During this period, 50 patients were selected for the study (10 patients per group). According to the obtained frequencies, the sample size was calculated using statistical software Minitab® (Minitab 17; Minitab, Inc.). The following parameters were used to calculate the sample size: global significance level of 95% (α = 0.05), power sample of 80% (β = 0.20), and standard error of 5%. It was observed that it would be necessary to have a sample of 323 patients to analyze the pain immediately or after 24 h in the first session of in-office dental bleaching and 369 patients in the second session. So, the required number of patients to obtain a significant pain difference in this study was incompatible with its duration. As cited above, it is important to investigate the best methodology to measure tooth sensitivity after dental bleaching before enlarging the study with other photobiomodulation parameters or study groups.
It is also suggested that other methodologies, not subjective as pain analysis, for example, oxygen saturation in dental pulp, can be evaluated in further studies after dental bleaching and photobiomodulation as complementary examination. 16
Another difference between the present study and the study by Moosavi et al. 24 is the point of irradiation. Both studies performed one point in the tooth cervical area; however, in the present study, one additional point of application was performed in the periapical area. Considering the results found in both studies, it could be suggested that the periapical point of irradiation is not necessary to obtain a positive result with photobiomodulation in preventing tooth sensitivity after in-office bleaching.
Despite the results found in the present study, photobiomodulation cannot be ruled out as an alternative equipment to control tooth sensitivity after bleaching, as other in vitro 17 and in vivo 24 studies have already shown positive results. In addition, other studies, with different methodologies of tooth sensitivity analysis, should be performed to verify the most appropriate method of analysis. Other photobiomodulation parameters should also be tested in future studies to enrich the knowledge in this scenario.
Conclusions
Within the limitations of the present study, the parameters of photobiomodulation tested were not efficient in preventing tooth sensitivity after in-office bleaching in vivo.
Footnotes
Acknowledgments
The authors thank FGM® for donating the bleaching kits used in this study.
Author Disclosure Statement
No competing financial interests exist.