
Abstract
Introduction
F
Photobiomodulation therapy (PBMT), formerly known as low-level laser therapy (LLLT), 2 is a noninvasive, safe application of light in use for the treatment of a variety of pathophysiological conditions, including inflammation, pain, and chronic wounds, with a few side effects. 3 Moreover, as such a treatment can improve the blood flow, it can be used to improve flap viability. 4
In this study, we treated ischemic flaps with 810 nm near-infrared (NIR) laser, 5 to observe the effect of this treatment on flap revascularization, and attempted to elucidate the mechanism of action.
Materials and Methods
Animals
This study was conducted in accordance with the Guide for the Care and Use of Laboratory Animals and was approved by the Animal Ethics Committee of the Peking University Health Science Center (ethics approval number: LA2013-83).
Sixty healthy male Sprague-Dawley rats weighing 350–400 g were housed in the Experimental Animal Center of the Peking University Health Science Center. All animals were given rat chow ad libitum.
Experiment
Establishment of animal model and laser irradiation
Each rat was anesthetized by intraperitoneal administration of 0.3% sodium pentobarbital at a dose of 0.1 mL/100 g. The surgical site was prepared by shaving the back and disinfecting the skin with conventional iodine alcohol. With the animal lying in the prone position on the operating table, two symmetrical long random-pattern flaps deep to the fascia were raised on the back. Each flap was located 1 cm from the spinous process of vertebrae, 6 cm long and 1 cm wide. The 1-cm-wide pedicle was located at the intersection of a line joining the two iliac spines (Fig. 1). The flaps were then sutured back to the original position with 5–0 silk stitches. Each rat was housed in a single cage postoperatively.

Flap design. The length:width ratio of the flap is 6:1. The two flaps are designed like mirror images by the midline.
Laser irradiation was performed on the left flap of the rat, and the right flap served as an internal control. When laser irradiation was applied to the animal, a stainless steel plate with an opening area of 2 × 8 cm was used to prevent irradiation exposure to the other parts of the animal body (Fig. 2).
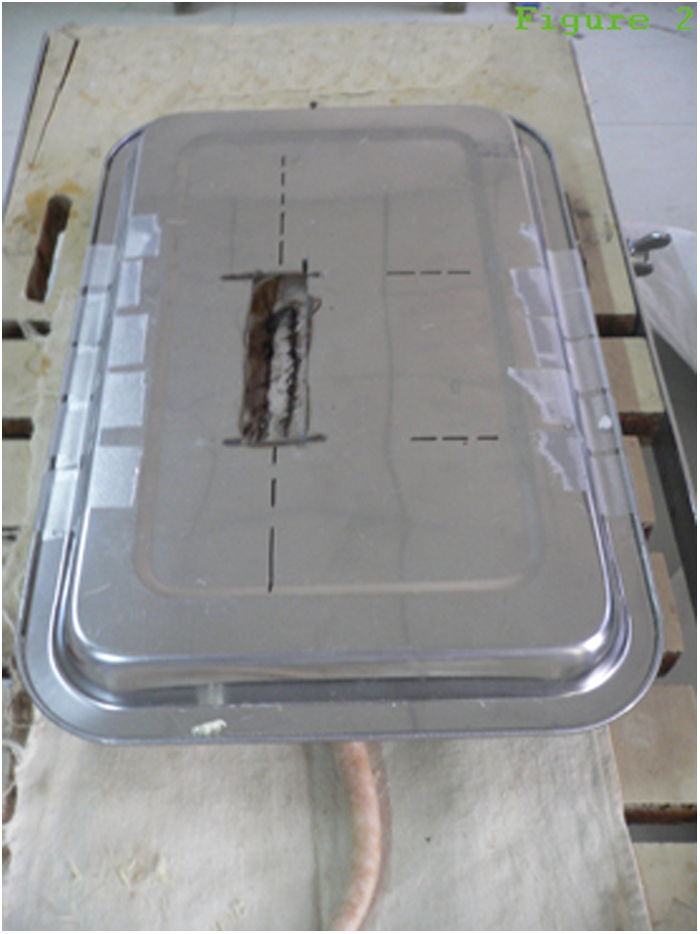
The internal control side flap (right side) and other parts of the rat are covered by a stainless steel plate when the left side flap is irradiated by the 810 nm NIR laser. NIR, near-infrared.
The SUNDOM-300IB/213 semiconductor gallium–aluminum–arsenide (GaAlAs) laser machine (Beijing SUNDOM Medical Equipment Co., Ltd.) was utilized. The laser wavelength was 810 nm. This machine had three laser probes, which were arrayed in a straight line, and the interval between each other was 3 cm. Each laser beam had divergence of 40° in horizontal direction and 10° in vertical direction, respectively. Therefore, each spot of the laser beam was a rectangle, and the short side was parallel to the line of the three laser probes. The distance between laser probe end point and flap surface was 5 cm. So the spot size of the whole three laser beams was 9.56 cm2. The output power of each laser beam was set at 100 mW, so the power intensity was 31.38 mW/cm2. The irradiation time was 6 min, and the energy density was 11.30 J/cm2.
We fixed the flap on the center of the whole three light spots, and made the long side of the flap parallel to the line of the three laser probes. The light spots could not cover the entire flap. The area of the flap and normal skin in the vicinities, which had been irradiated, was 5.28 cm2. Total energy delivered to the back of the rat was 59.66 J. Laser irradiation was performed at a laser mode sat on continuous wave, and it was applied once a day under intraperitoneal anesthesia. The rats were divided into four groups on average. Each group was irradiated postoperatively for 4, 7, 10, and 14 days, respectively. The skin flaps were photographed after each irradiation session.
Flap healing and flap survival area
Photographs of the flaps were taken 4–7 days postoperatively when the necrotic areas fixed. Digital images of the skin flaps were analyzed using Image-Pro Plus 6.0 (Media Cybernetics, Inc., Bethesda, MD) to calculate the necrotic areas. Flap survival was calculated using the following formula: flap survival = flap survival area/flap total area × 100%.
Hematoxylin and eosin and immunohistochemical staining
Four rats chosen from each of four groups were euthanized. The 0.5-cm-long basis and end of both sides of flaps of each rat were collected. These four skin samples underwent routine staining with Hematoxylin and Eosin (H&E). We also performed immunohistochemical (IHC) staining of factor VIII for the capillary count, IHC staining of α-smooth muscle actin for the small arterial count, and IHC staining of vascular endothelial growth factor (VEGF) for the integrated optical density (OD) of the positive stained color.
Most of reagents were purchased from Beijjing Zhongshan Golden Bridge Biotechnology Company, Beijing, China. Formalin-fixed, paraffin-embedded tissue sections (4 μm thick) underwent deparaffinization, stepwise rehydration, and endogenous peroxide blockage. For both factor VIII and α-smooth muscle actin staining, slides were processed with antigen retrieval achieved by boiling the slides in citrate buffer (pH 6.0) for 1.5 min. For VEGF staining, slides were boiled in an EDTA solution for 20 min before cooling. Nonspecific binding was blocked using 10% nonimmune goat serum (ZLI-9021) for 10 min. Sections were incubated for 120 min at room temperature with factor VIII antibody (ZA-0111) at a 1:200 dilution, anti-VEGF antibody (ZA-0509) at a 1:100 dilution, or α-smooth muscle actin antibody (ZM-0003) at a 1:100 dilution.
After rinsing, the sections for IHC staining of VEGF and α-smooth muscle actin were incubated with secondary antibodies labeled with HRP (K5007, EnVision™ Detection System, Dako, Denmark) for 30 min at 37°C followed by visualization with diaminobenzidine (DAB+) chromogen (K5007, EnVision™ Detection System), counterstained with Hematoxylin, dehydrated, and mounted. But the sections for VEGF OD analysis were not counterstained with Hematoxylin following visualization with DAB chromogen, which aimed for more accurate analytic results. The sections for ICH staining of factor VIII were incubated with biotinylated secondary antibody (ZB-2010) at a 1:300 dilution for 60 min at 37°C. After rinsing again, these sections were incubated with alkaline phosphatase streptavidin (ZB-2422) at a 1:500 dilution for 60 min at 37°C followed by visualization with BCIP/NBT (ZLI-9041), counterstained with Eosin, dehydrated, and mounted.
Negative controls were processed using the same procedure, except the absence of the primary antibodies. No detectable staining was observed in any of the negative control slides.
In IHC staining of factor VIII, the boundaries of capillaries were stained purple. Ten visual fields (400 × ) were chosen randomly in each slide of basis of both side flaps for capillary count. Then we calculated the mean count, respectively.
In IHC staining of α-smooth muscle actin, the boundaries of arterioles were stained brown. Ten visual fields (400 × ) were chosen randomly in each slide of basis of both side flaps for arteriole count. Then we calculated the mean count, respectively.
In IHC staining of VEGF, the positive expression was cytoplasm stained brown. Image-Pro Plus 6.0 was used for quantified analysis to calculate the integrated OD of positive stained color (brown color) of each slide of basis of both slide flaps. Then we calculated the mean OD, respectively.
Statistical analysis
Data were analyzed using SPSS 23.0 and expressed as mean ± standard deviation. Data were analyzed using a standard t-test, and significance was denoted by p values <0.05.
Results
Flap survival area
All rats demonstrated a steady increase in necrosis size as time progressed (Fig. 3). At 4–7 days postoperatively when the necrotic areas fixed, the irradiated flaps showed significantly more survival areas (85.99% ± 10.03%) than that of the internal control flaps (81.76% ± 10.62%) (p < 0.01).
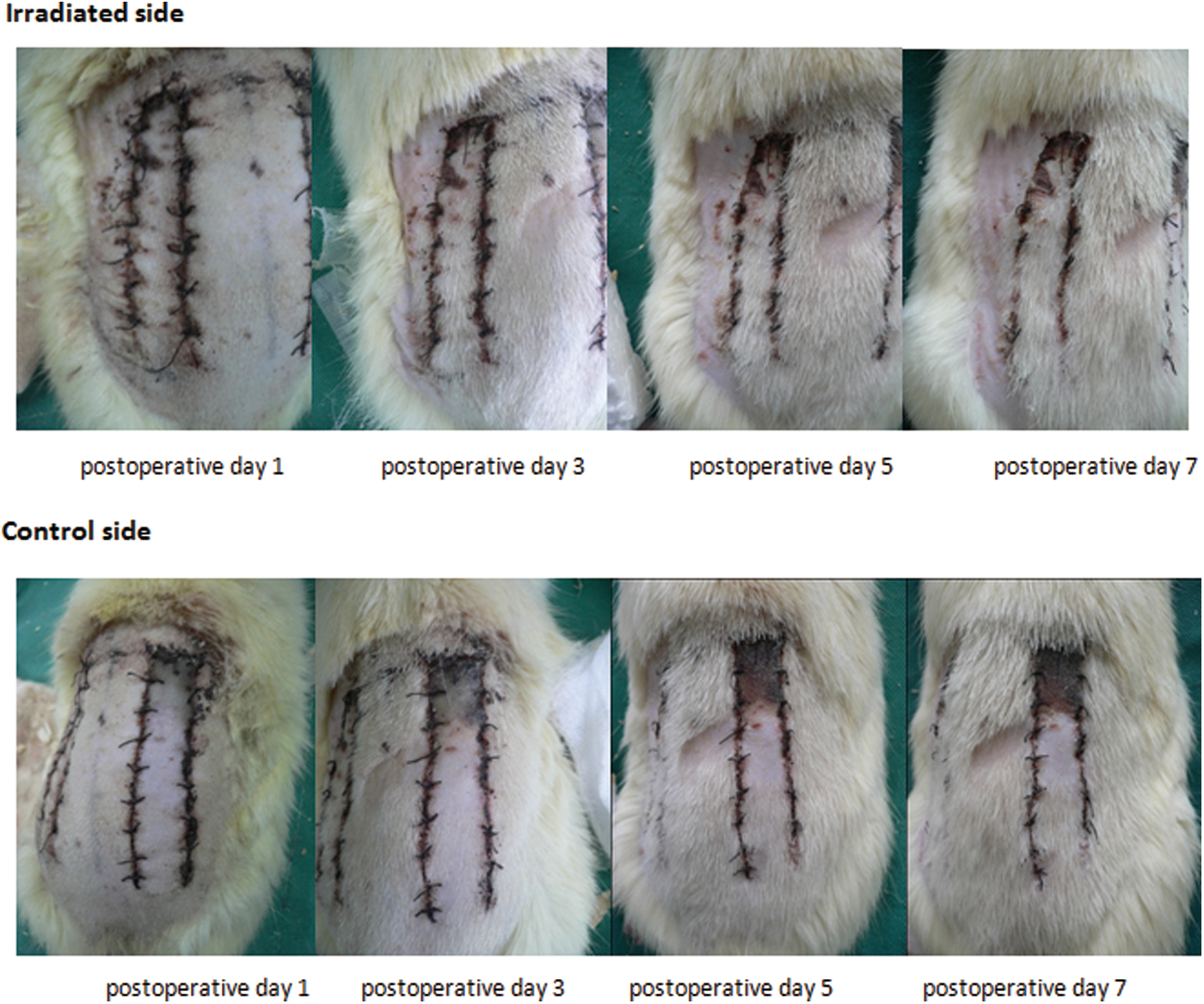
Flap healing changes on first day, third day, fifth day, and seventh day postoperation, respectively. The irradiated side shows a better flap survival. The control side shows poor healing, early necrosis, and black scab formation.
Histomorphology assessment
H&E staining
In the end of irradiated flaps, the structure of the dermomuscular layer was slightly disordered and there was a large number of subcutaneous inflammatory cell infiltration. While in the end of internal constrol flaps, the dermomuscular layer was atrophied and there was a significant accumulation of inflammatory cells.
In the basis of irradiated flaps, tissue structure was discernible with sufficient subcutaneous vasculature and the muscle fibers of the dermomuscular layer arranged regularly. There was only little inflammatory cell infiltration. As for the basis of internal control flaps, the subcutaneous vasculature and muscle fibers of the dermomuscular layer were still rich without shrinkage, but poorly colored. Muscle cells were swollen and there were more inflammatory cell infiltration (Fig. 4).
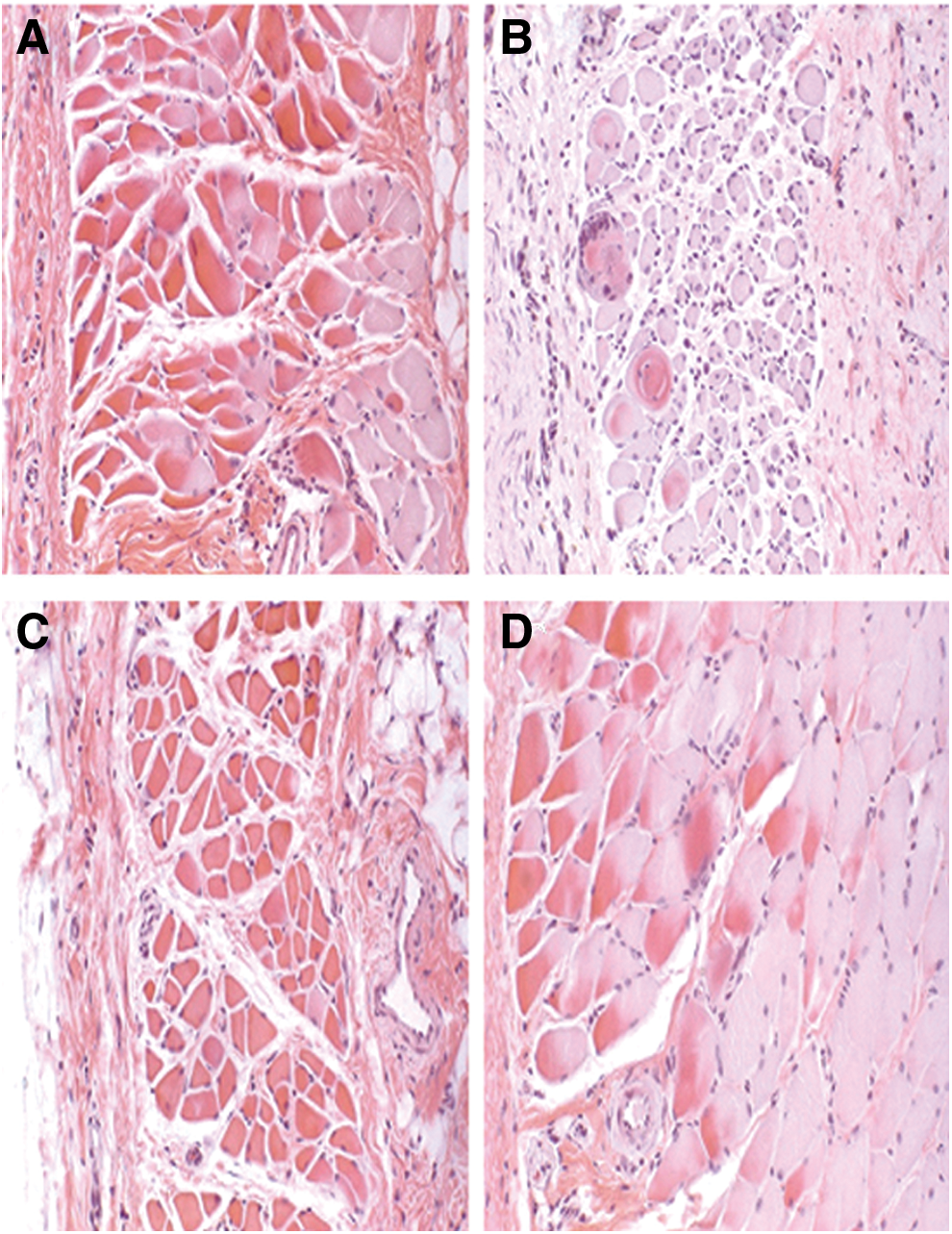
HE staining (200 × ) of both side flaps after 14 days of irradiation.
Capillary count of factor VIII-related antigen IHC staining
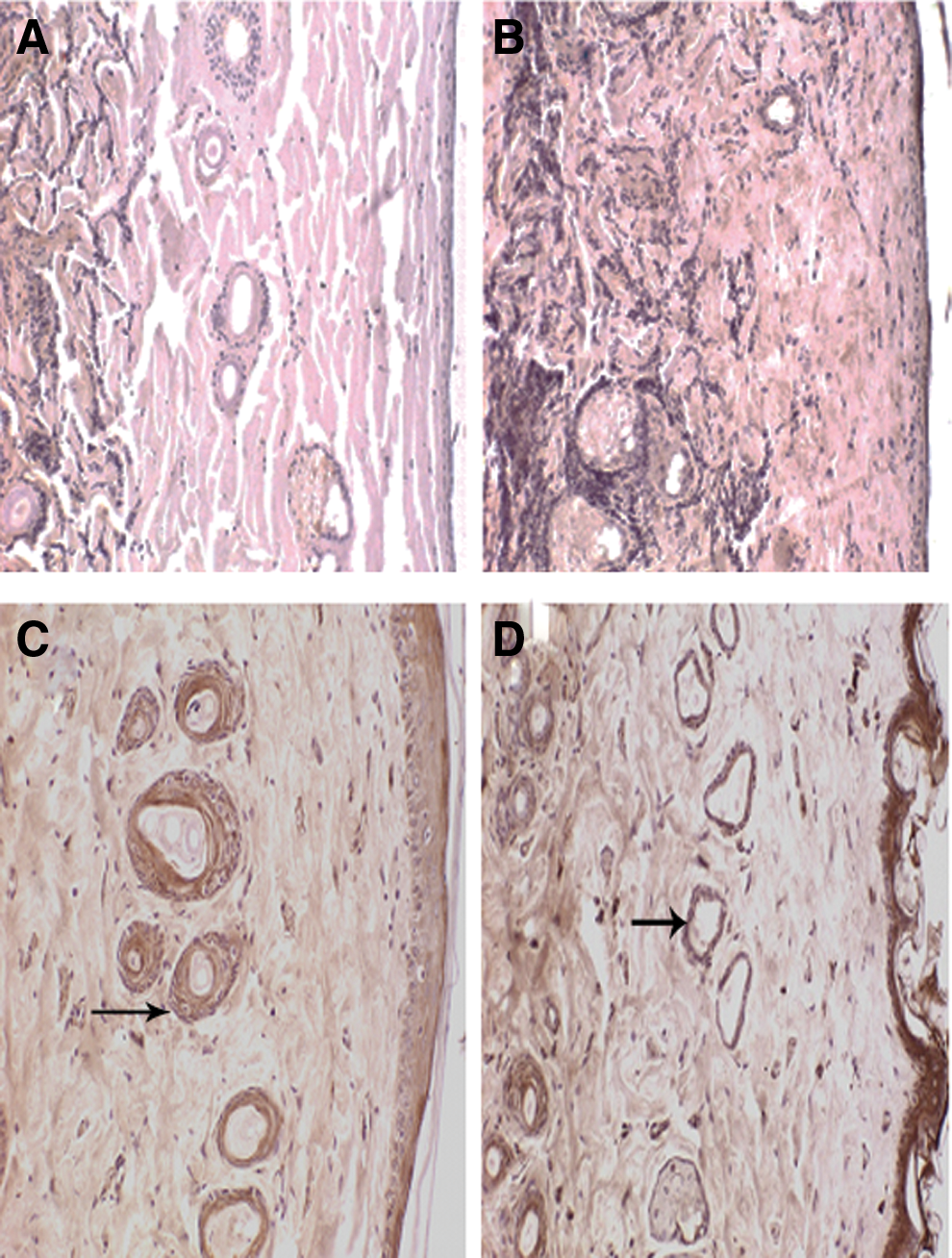
The end of both side flaps demonstrated scabbing, necrosis, and uniform pink eosin staining under microscopy without purple capillaries distribution. The basis of flaps demonstrated rich capillaries, as shown in Fig. 5. The capillary count of basis of both side flaps is shown in Table 1. The results showed that the capillary count of the irradiated flaps was significantly higher than that of the internal control flaps (p < 0.05); however, there was no significant difference in the 4-day group.
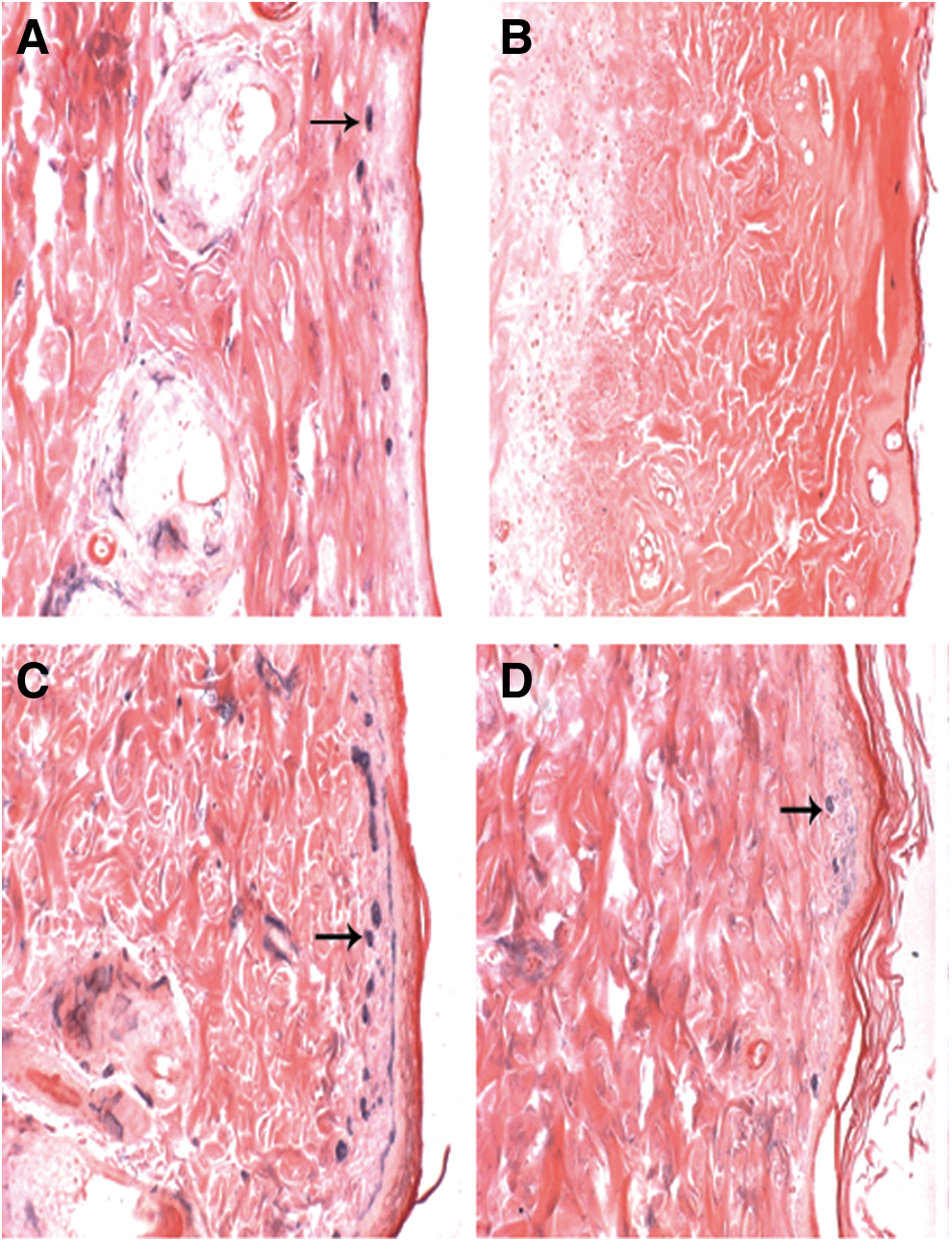
Factor VIII IHC staining (200 × ) of both side flaps after 14 days of irradiation, (arrow, capillary).
Compared with the internal control flap, p < 0.05.
Small artery count of anti-α-smooth muscle actin IHC staining
The small artery's distribution in the epidermis and subcutaneous connective tissue is shown in Fig. 6. The small artery count of the basis of both side flaps is shown in Table 2. The results showed that the number of small arteries in the irradiated flaps was significantly higher than that in the internal control flaps (p < 0.05); however, there was no significant difference in the 4-day group.
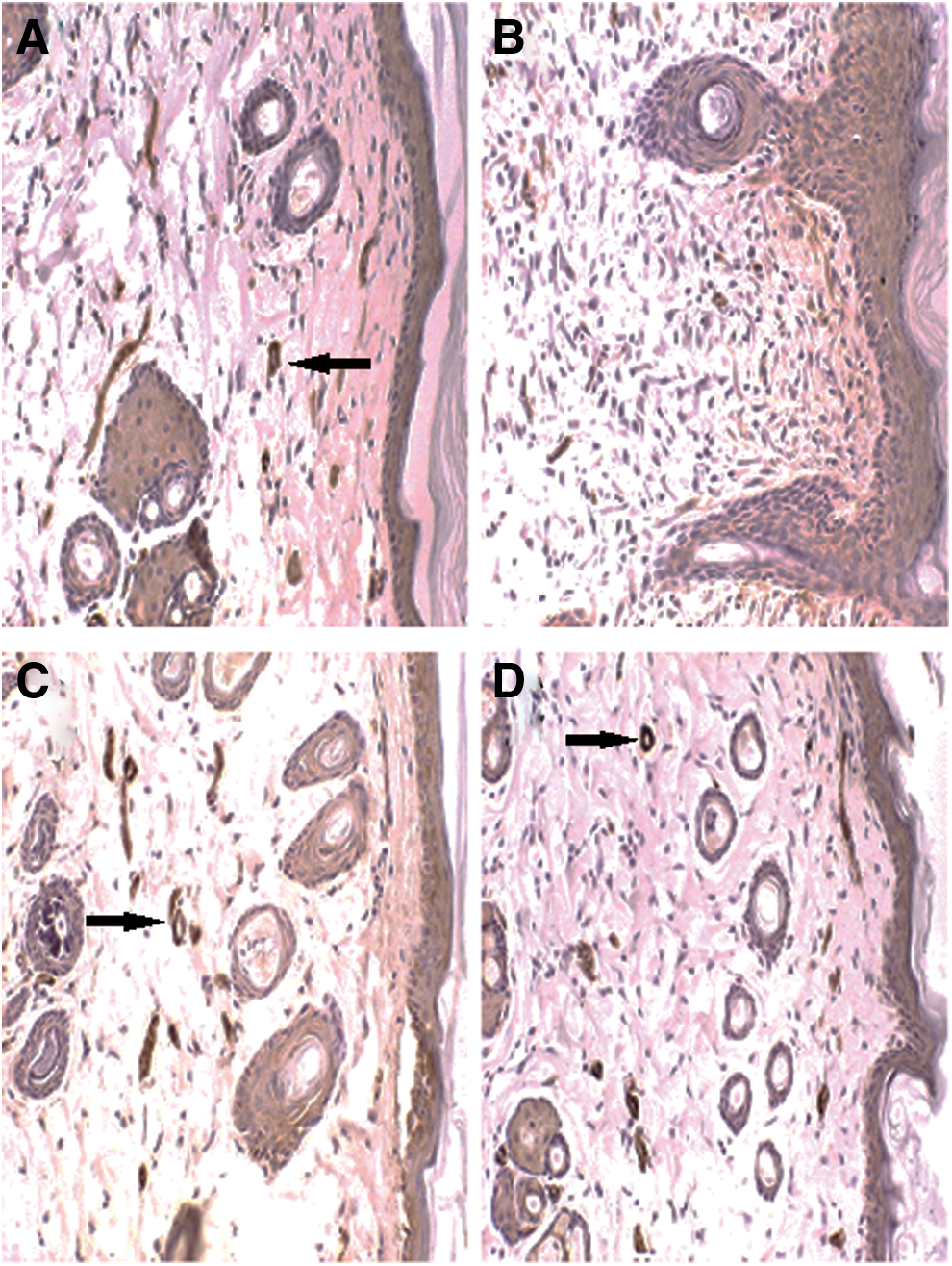
α-smooth muscle actin IHC staining (200 × ) of both side flaps after 14 days of irradiation, (arrow, arteriole).
Compared with the internal control flap, p < 0.05.
OD of VEGF IHC staining
Weak expression of VEGF was present at the end of the flaps. However, high expression of VEGF was present in the basis of the flaps, especially in vascular endothelium and dermomuscular layer (Fig. 7). The OD of the basis of both side flaps is shown in Table 3. The OD of the irradiated flaps was slightly higher than that of the internal control flaps, but without statistical significance (p > 0.05).
VEGF IHC staining (200 × ) of both side flaps after 14 days of irradiation, (arrow, expression of VEGF).
Compared with the internal control flap, p > 0.05.
Discussion
LLLT, which has been applied for more than 40 years, 6 is now denominated as PBMT. 2 The PBMT can result in beneficial therapeutic outcomes, including but not limited to the alleviation of pain or inflammation, promotion of wound healing, and tissue regeneration. 2 All of these effects are not mediated through the thermal increase, which is one of the most distinguishing features of PBMT as compared with other photoceutical modalities. 7 The basic biological mechanism of the effects of PBMT is thought to be through absorption of low-level laser by chromophores, in particular cytochrome c oxidase (CCO), which is complex IV of the mitochondrial respiratory chain. 8 Then the cells activate retrograde light-sensitive cellular signaling events to transport the light signal from mitochondria to nucleus, which eventually alter the cellular metabolism and functions. 9 The mitochondrial photoacceptor, CCO, is identified as a principal tissue chromophore for visible/NIR spectral light. 8
The tissue–light interaction primarily depends on wavelength, as it determines the absorption mechanism and the depth of penetration. 10 PBMT generally employs light at red (630–680 nm) and NIR (800–830 nm) wavelengths to modulate biological activities, 11 as they are highly active in the healing process. 12 –14
Red light is readily absorbed by blood and skin surface components, thereby limiting its tissue penetration to <10 mm. While NIR light is not readily absorbed and has a much deeper depth of tissue penetration (30–40 mm or more), this provides a greater deposition of photons into the wound bed, and show therapeutic healing efficacy. 15 Moreover, biological tissue has lower scattering capacity at the NIR region than at the visible region, 16 because CCO has distinct absorption bands in the red and in the NIR regions. 13 So NIR is found to be the most effective and widely studied wavelength range followed by red light exhibiting beneficial photobiomodulatory effects on impaired dermal wound healing, which could be attributed to the greater penetration and to the absorption spectrum of CCO. 15,16 To investigate the revascularization of ischemic flaps, target tissues applied with PBMT are located deeper under the skin. From this perspective, 810 nm NIR laser was selected in our study.
Flap survival area
In our study, improvement of ischemic flap survival was the most apparent performance of the 810 nm NIR laser irradiation. Flap revascularization could be observed by the naked eye.
According to Bossini's experiment, 17 670 nm laser effectively increased the viability of the skin flap and energy density of 24 J/cm2 was more effective than 12, 6, and 3 J/cm2, so there was a tendency for better results at higher energy density. While other studies demonstrated that too high energy density of light had deleterious effects on cells by inducing apoptosis through generation of high levels of reactive oxygen species. 18,19 Previous research indicated that the effect of wound repair improvement by PBMT was a result of an inversely proportional relationship between wavelength and fluence, with treatment more effective when combining higher fluence with shorter wavelength or lower fluence with longer wavelength. 20
Al-Watban 21 demonstrated wound healing of diabetic rats was markedly accelerated after PBMT at 810 nm by fluence of 5 and 10 J/cm2 (not at 20 and 30 J/cm2). Similarly, PBMT at 808 nm (GaAlAs) and 10 J/cm2 could improve incisional wound healing. 22 In our study, to improve ischemic flap survival, 810 nm laser irradiation was performed daily in our study with energy density of 11.30 J/cm2 and total energy of 59.66 J. The present experimental results did show that 810 nm NIR lasers reduced the necrotic area as evidenced by the survival area of up to 85.99% ± 10.03%. Whether the fluence used in the present study was optimal still needed further research. However, these data indicated a positive effect of 810 nm NIR laser therapy on flap survival.
The result of better survival revealed that the 810 nm NIR laser irradiation might strongly promote revascularization, accelerate healing, and then reduce necrosis. The effect of revascularization promotion and healing acceleration had been proven by many studies. Kubota 23 showed increased blood flow and perfusion of transferred flaps after irradiation with an 830 nm NIR laser. Gupta 15 and Keshri 24 both demonstrated healing efficacy of 810 nm NIR laser PBMT on dermal wounds. Our finding of the necrosis reduction by 810 laser irradiation was in agreement with other studies. Prado, 25 for instance, indicated 830 nm laser was effective in increasing skin flap viability in rats. In addition, das Neves 26 found that PBMT with 830 nm laser decreased the area of necrosis in rats subjected to nicotine, which had been confirmed to have the deleterious effect on skin flap.
Morphological changes
Naked eye results are supported by the histological patterns, which can offer some information about the mechanism responsible for the improved flap survival. Surgical trauma to the body causes inflammatory reactions. Intense inflammatory response may cause flap edema and pain. Moreover, tissue swelling may decrease blood flow velocity and reduce the nutrient supply of the flap. However, PBMT can be used for anti-inflammatory treatment, which has been confirmed by previous studies. 27,28 In addition, there were some other researches that had the same results. Pinfildi 29 indicated that PBMT could stimulate mast cell growth in flaps to increase vascular perfusion. Albertini 30 found that red laser (660 and 684 nm) PBMT significantly reduced carrageenan-induced paw edema, and muscle inflammation was also significantly reduced in rats. All of these showed that PBMT could reduce inflammation and edema and inhibit inflammatory cell migration.
As for NIR laser, positive effect on the reduction of inflammatory cell infiltration was still significant. Keshri 24 demonstrated that 810 nm PBMT could reduce inflammatory infiltration and enhance fibroblast proliferation, angiogenesis, and re-epithelialization in the wound tissues of immunosuppressed rats. The study of Rezende 31 suggested that 830 nm NIR laser irradiation could act on the cellular events that happen during inflammatory stage, and the reduction on the duration of the inflammatory stage might result in a faster entry into the proliferative stage of healing. Moreover, their histological analysis also showed a lower polymorphonuclear infiltration in irradiated lesions than control lesions. Study of Pallotta 32 also indicated that 810 nm PBMT was able to significantly inhibit the total number of leukocytes, which was confirmed by cell counting showing the reduction of polymorphonuclear cells at the inflammatory site.
In our study, HE staining showed that the inflammatory cells in the irradiated flaps were significantly less than that in the internal control flaps, which demonstrated that the flaps treated with 810 nm NIR laser irradiation healed well, whereas the flaps that were not irradiated became swollen due to inflammatory exudation and healed slowly. Therefore, reduction on the duration of the inflammatory stage might promote revascularization of ischemic flaps, sequentially improve the healing, and reduce the area of necrosis.
The revascularization rate directly affects the survival of flap transplanted. VEGF can promote the growth of vascular endothelial cells and the formation of blood vessels. PBMT had been demonstrated to increase the gene expression and release of VEGF by cells. 33 Prado 34 found that 830 nm PBMT promoted flap expression of VEGF and angiogenesis, and sequentially reduced flap necrosis. Keshri 24 also demonstrated VEGF expression increased significantly in the 810 nm laser irradiation group than the control group. Our study showed that 810 nm laser irradiation promoted VEGF synthesis in, and secretion from, the basis of the flaps. But the expression of VEGF between the irradiated side and the internal control side was not significantly different, which was not consistent with previous studies. We thought it possible that VEGF of irradiated flap went to adjacent cells or tissue of the internal control flap, which was on the same rat, through paracrine mode. 35 But we did not test it in this study.
VEGF can also promote vascular proliferation within flaps. Yaakobi 36 used 804 nm laser to treat rats with myocardial infarction by ligation of the left anterior descending artery. They found the myocardial infarction size was reduced significantly after the irradiation, and neovascularization rate of the laser irradiation group was 3.1 times higher than that of the control group, which was a significant increase. Oron 37 demonstrated 810 nm PBMT applied to mdx mice during postnatal development might have a significant beneficial effect in the process of skeletal muscle regeneration and angiogenesis.
Our study also found significant changes of vascular proliferation in the flaps on the irradiated side. The factor VIII-related antigen IHC staining for capillaries and anti-α-smooth muscle actin IHC staining for small arteries showed higher number of blood vessels in the irradiated flaps than the internal control flaps. This phenomenon became apparent with continuous irradiation more than 4 days, and there was an increasing trend. The previous study 26 also demonstrated that 830 nm NIR laser could increase the number of blood vessels of flaps, and consequently, decrease the area of necrosis. In addition, the proliferation of blood vessels of the 4-day group in our study showed no statistically significant difference between the irradiated side and the internal control side, indicating that the effect of 810 nm laser on angiogenesis became prominent after 4 days of irradiation. These data suggested that it took a few days for endothelial cells to form vascular structures.
Our data suggested that the increased number of blood vessels was closely related to the 810 nm laser irradiation, which resulted in more perfusion of blood in the ischemic flaps and in the decrease of the necrotic area of the end of ischemic flaps.
Conclusions
The focus of this research was the 810 nm NIR laser effect on the revascularization of ischemic flaps on the rats. Our findings indicated that PBMT with 810 nm laser, at the tested parameters, inhibited excessive inflammation and facilitated angiogenesis, so improving revascularization, promoting flap healing, and enhancing skin flap survival. Nevertheless, further studies should be conducted to find optimal therapeutic parameters and to determine the efficacy of 810 nm NIR laser irradiation on patients for clinical application.
Footnotes
Acknowledgments
The authors thank Jian-Ning Li, Yong-Guang Ma, Dong Li, and Li Chen for assisting with the experiment.
Author Disclosure Statement
This work was supported by the Scientific Seed Fund of Peking University Third Hospital.