
Abstract
Introduction
P
It is now widely accepted that the noncoherent light from LEDs behaves the same as coherent laser light for most medical applications. In addition, the ability to deliver reasonable power densities (up to 100 mW/cm2) over relatively large areas of the body and to mix different wavelengths together (for instance, red and NIR) are major advantages of LED arrays. An important consideration that applies to many areas of PBM is that of the “biphasic dose–response” or Arndt–Schulz curve. 1,2 This principle states that there are optimum parameters (energy density or power density) that provide a benefit to the particular disease, and if these parameters are substantially exceeded, the benefits disappear and can even lead to damaging effects if the dose is extremely high. This phenomenon is also called “hormesis” and has been comprehensively reviewed by Calabrese and Mattson 3 and Calabrese and Baldwin. 4
PBM and Cancer
Because PBM was shown to stimulate the growth of cancer cells in cell culture studies, 5 and can also increase the aggressiveness of some cancer cells, 6 some commentators have asserted that PBM may be contraindicated in clinical use in patients with cancer. 7 However, not all experimental studies have found the same results. In contrast, it was realized that PBM was highly effective in the mitigation of numerous distressing side effects that occur as a result of a range of different kinds of cancer therapy. 8,9
Figure 1 presents a graphical summary of the different kinds of cancer-therapy side effects that could possibly be treated by PBM. These side effects can be so severe that they often lead to the suspension or discontinuation of the cancer therapy with consequent risk to the patient. Perhaps the single most effective indication for PBM (among all known diseases and conditions) is that of oral mucositis. 10 Oral mucositis is a common side effect of many kinds of chemotherapy and of radiotherapy for head and neck cancer. 11 Other side effects that are under investigation by PBM treatment are chemotherapy-induced peripheral neuropathy, 12 radiation dermatitis associated with breast cancer therapy, 13 and lymphedema as a result of breast cancer surgery. 14
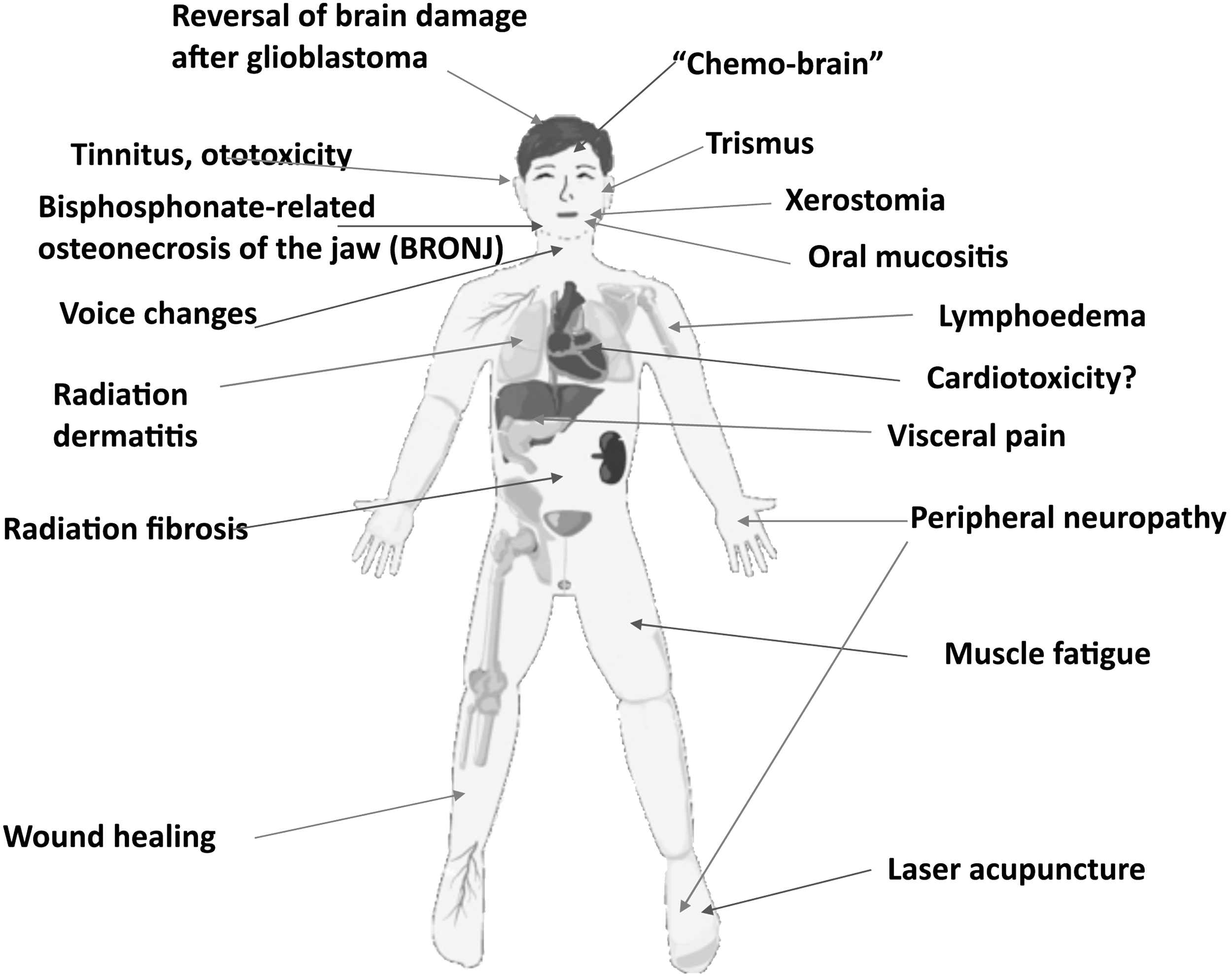
Cancer therapy side effects possibly treated by PBM. PBM, photobiomodulation.
Some years ago, when PBM was routinely carried out with laser beams directly applied to the affected tissue region, its use for the mitigation of cancer-therapy side effects was employed with the caveat that the laser should not be used directly over the site of the tumor. However, now that large-area LED arrays and even whole-body light bed systems are becoming more common, the question of whether these devices are safe for a patient with cancer needs to be addressed as pointed out by Sonis et al. 15 Moreover, individuals who are using PBM for general health improvement or for increase in athletic performance 16 are asking the question: what if I have an undiagnosed malignant or premalignant lesion?
Can PBM Stimulate Cancer?
Despite the existence of numerous studies that have shown that PBM can increase the growth rate of cancer cells in cell culture, 17 the number of studies that suggest that PBM can actually exacerbate or stimulate cancer growth in animal tumor models in vivo are relatively few. One study by Frigo et al. compared the effects of PBM (660 nm, 2.5 W/cm2) delivered once a day for 3 days either at a low dose or a high dose in subcutaneous melanoma in mice. 18 The low dose (150 J/cm2) reduced the tumor size (not statistically significant), while the high dose (1050 J/cm2) significantly increased the tumor size. However, this study suffered from some problems such as the claim that a C57BL/6 tumor (B16F10) was grown in a nonsyngeneic mouse strain (BALB/c).
Another study from Rhee et al. looked at PBM (650 nm, 100 mW/cm2) as a single dose to an orthotopic mouse model of anaplastic thyroid cancer. 19 However, these investigators used an immunodeficient nude mouse model, which does not accurately reflect most human patients. The tumor growth was faster in the PBM groups; HIF-1a and p-Akt were increased, while TGF-b1 expression was decreased.
The third study looked at PBM in the Syrian hamster cheek pouch model of chemical carcinogenesis caused by application of dimethylbenzanthracene (DMBA). 20 Researchers applied PBM (660 nm, 424 mW/cm2) every other day for 4 weeks starting at end of the cancer induction period (8 weeks of DMBA). More tumors in the PBM group were histologically graded as “poorly differentiated,” and presumably would have a worse prognosis.
Can PBM Directly or Indirectly Attack Cancer?
When we consider the possibility that PBM can have a beneficial effect on cancer, it is important to realize that there are three possible ways by which this may happen (Fig. 2). The first involves the direct effect of the light on the tumor cells themselves and may be thought of as a deliberate use of the biphasic dose–response curve to “overdose” the cancer cells. 21 This possible methodology has been championed by Da Xing's laboratory in China. 22 They call this approach “high fluence low-power laser irradiation, HF-LPLI” and this group often uses a 632 nm HeNe laser delivering 1200 J/cm2 at 500 mW/cm2, over 40 min. 23 After publishing several in vitro articles they carried out an in vivo study in BALB/c mice bearing EMT6 breast tumors. 24 A single dose of 1200 J/cm2 caused complete regression of tumors, which did not occur in rho-zero EMT6 tumors (lacking functional mitochondria). Moreover, since EMT6 tumors are known to be immunogenic, the mice that were cured of cancer showed some long-term immunological memory.
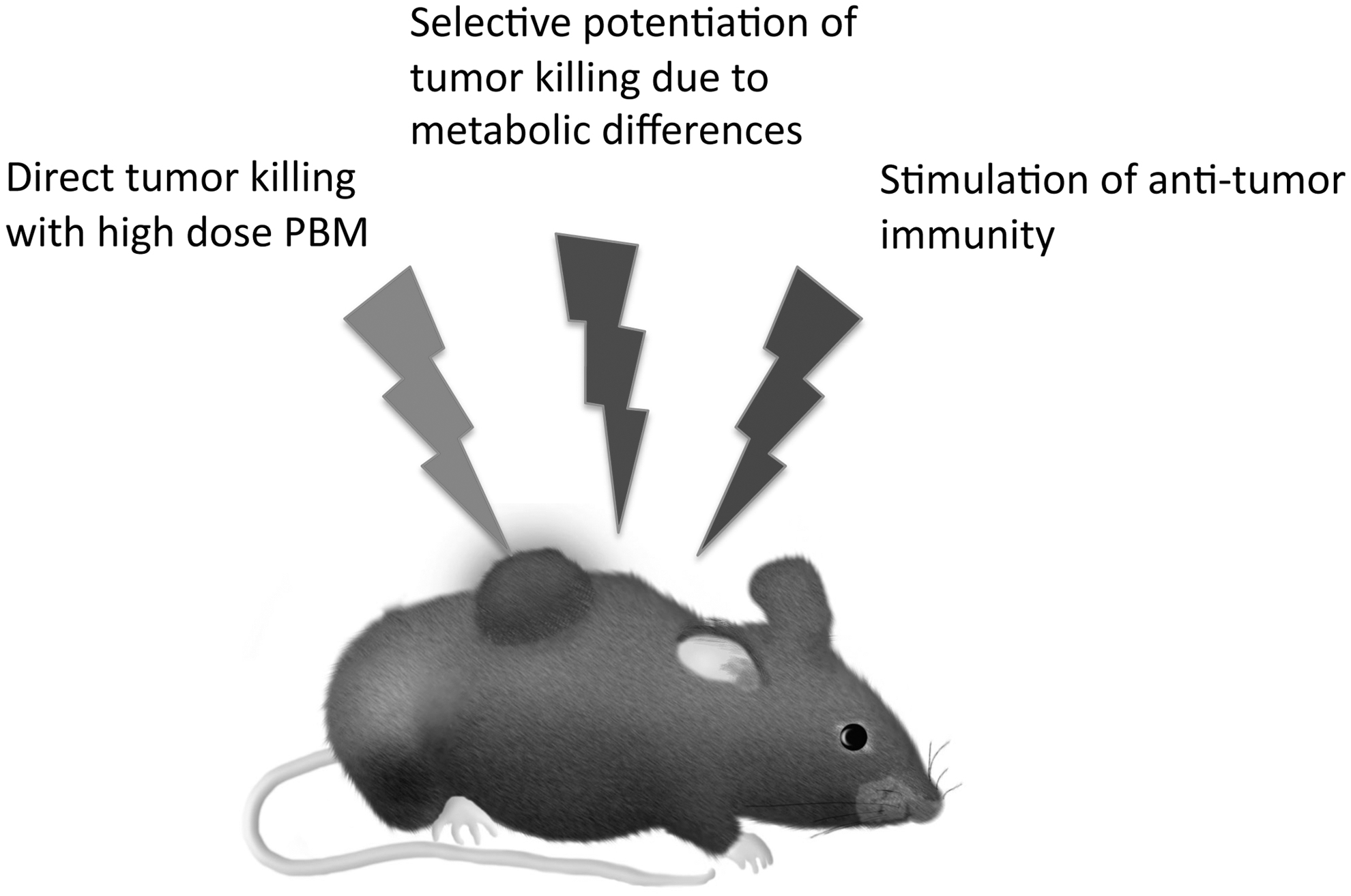
Possible mechanisms by which PBM could be applied against cancer.
The second method relies on taking advantage of a differential effect of PBM between malignant cancer cells compared to the effects seen on healthy normal cells. This involves combining PBM with an additional cytotoxic anticancer therapy, so that it increases the killing of cancer cells, while at the same time protecting normal healthy cells. While this may appear “too good to be true,” there are some scientific reasons why it may in fact be the case.
These considerations are related to the Warburg effect, by which the mitochondria of cancer cells change their metabolism to carry out aerobic glycolysis instead of oxidative phosphorylation. 25 This phenomenon occurs due to the rapid growth of tumor cells outpacing the development of a sufficient blood supply, forcing the cancer cells to become tolerant to chronic hypoxia. Glycolysis consumes much less oxygen than oxidative phosphorylation. The consequences of the Warburg effect are that malignant cells and normal cells may behave very differently in response to PBM. In cancer cells, where adenosine triphosphate (ATP) supply is quite limited, the ATP boost given by PBM may allow the cancer cells to respond to pro-apoptotic cytotoxic stimuli with more efficiently executed cell death (apoptosis) programs, which are heavily energy dependent (i.e., require a lot of ATP 26 ). In contrast, in normal healthy cells that have an adequate supply of ATP, the effect of PBM produces a burst of reactive oxygen species (ROS) that could induce protective mechanisms and reduce the damaging effects of cancer therapy on healthy tissue (Fig. 3). Although this favorable scenario remains a hypothesis at present, there are some published articles that suggest that it could indeed be the case in some anticancer strategies, such as reports that PBM can potentiate the killing of cancer cells by photodynamic therapy 27 and also by radiation therapy. 28 These researchers have reported that, in theory, PBM increases cell death in cancer cells in response to cytotoxic stimuli. Alternatively, while in normal cells, PBM will exert its protective effect as is well known in the case of neurotoxins, for example. 29
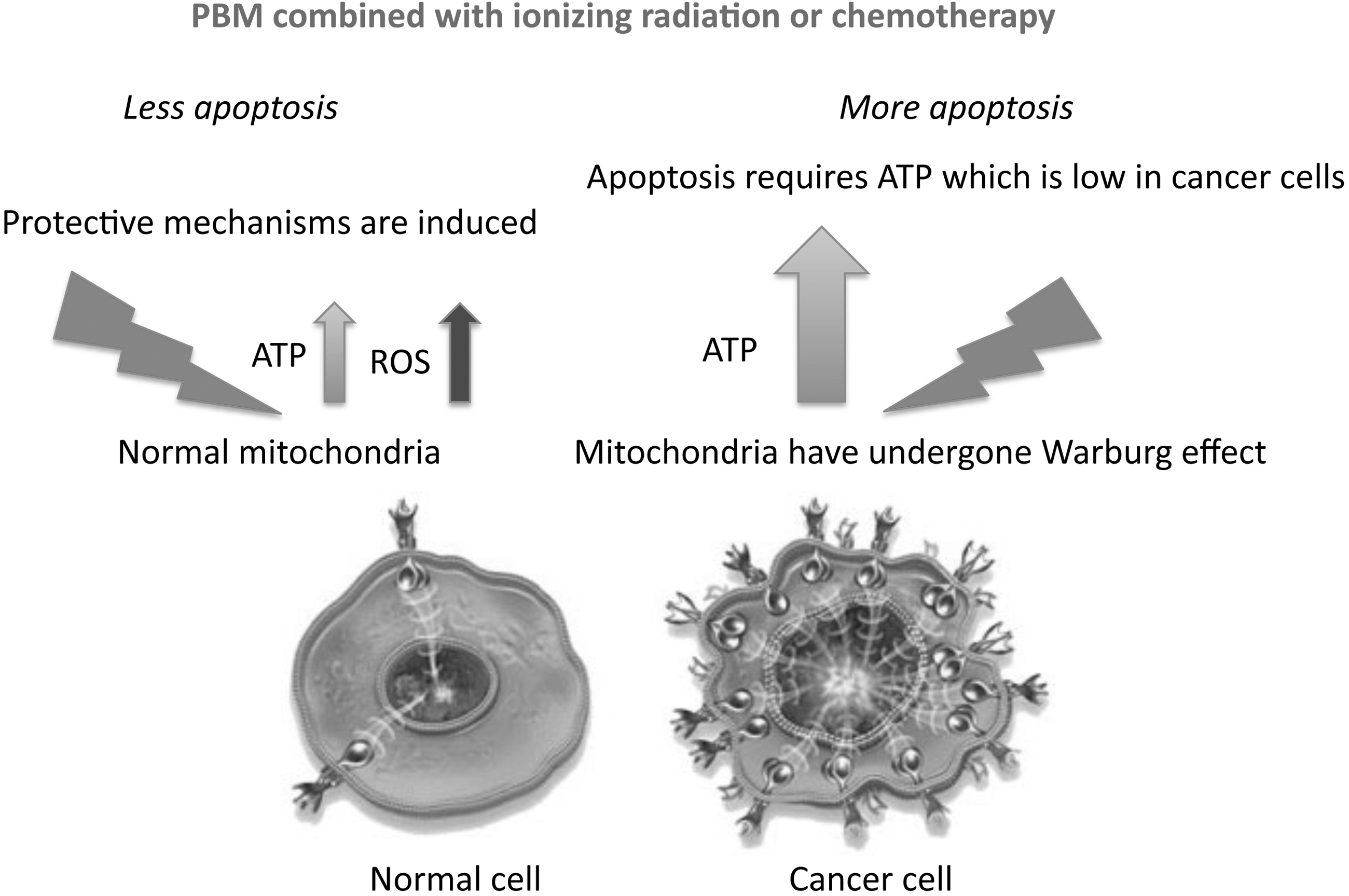
Mechanisms of selective potentiation of cytotoxicity against cancer cells while preserving normal cells.
The third mechanism, by which PBM could be beneficial to cancer patients, is its possible role in stimulation of the immune system to fight against the cancer. Ottaviani et al. 30 showed in a mouse model of melanoma that PBM using three different protocols (660 nm, 50 mW/cm2, 3 J/cm2; 800 or 970 nm, 200 mW/cm2, 6 J/cm2, once a day for 4 days) could all reduce tumor growth and increase the recruitment of immune cells (in particular, T lymphocytes and dendritic cells secreting type I interferons). PBM also reduced the number of highly angiogenic macrophages within the tumor mass and promoted vessel normalization, which is another strategy to control tumor progression.
A recent article from Brazil 31 used PBM (660 nm, 100 mW, delivering 35, 107, or 214 J/cm2) to the tumor site thrice every 2 days starting 14 days after rat Walker sarcoma tumor implantation. They measured expression of IL-1β, IL-6, IL-10, and TNF-α by enzyme-linked immunosorbent assay and COX-1, COX-2, iNOS, and eNOS by reverse transcriptase polymerase chain reaction (RT-PCR) in the subcutaneous tumor tissue. Although tumor response was not directly measured, they claimed that the lowest dose (35 J/cm2) produced significant increases in IL-1β, COX-2, and iNOS and significant decreases in IL-6, IL-10, and TNF-α and concluded that the 35 J/cm2 “produced cytotoxic effects by generation of ROS causing acute inflammation.”
Is There Evidence of Clinical Efficacy?
A very interesting recent article 32 reported that PBM could actually increase treatment outcome and progression-free survival in cancer patients. Ninety-four patients diagnosed with oropharynx, nasopharynx, and hypopharynx cancer were subjected to conventional radiotherapy plus cisplatin every 3 weeks. Preventive PBM was applied to nine points on the oral mucosa daily, from Monday to Friday, and lasted on average 45.7 days. The PBM parameters were 660 nm, 100 mW, 4 J/cm2, and spot size 0.24 cm2. Over a follow-up period of 41 months, patients receiving PBM had a statistically significant better complete response to treatment than those in the placebo group (p = 0.013). Patients subjected to PBM had better progression-free survival than those in the placebo group (p = 0.030) and had a tendency for better overall survival. The mechanism(s) for this effect require more investigation. It could be that the avoidance of oral mucositis led to better nutrition and more complete chemoradiotherapy, while it is also possible that the PBM exerted a direct anticancer effect.
Santana-Blank et al. 33 carried out a Phase 1 trial of PBM on 17 patients suffering from a variety of “advanced malignancies.” They used a 904 nm infrared laser, pulsed at 3 MHz, applied using a 2-mm high top hat with a 10-mm beam diameter, and placed at right angles to the surface of the patient's skin in previously determined areas of closest proximity to the biologically closed electric circuits and the vascular interstitial closed circuit that would most efficiently carry the laser energy to the target tissues. 33 This approach was first described by Nordenstrom 34 who inserted wires through the thoracic wall to reach pulmonary tumors and circulated electric current. Patients were given a laser device to use at home each day and were allowed to remain in the trial as long as possible.
In addition to evaluation by the attending physicians, the patients were asked to keep a journal over the length of their time in the trial and to record the time and duration of each PBM application, as well as any sign, symptom, or problem/side effect experienced. No dose-limiting toxicity was observed. Five patients reported occasional headaches (grade 2), and four referred local pain (grade 2). Statistically significant increases in Karnofsky performance status and quality of life (QLI) were observed in all of the follow-up intervals compared with pretreatment values. In the six surviving patients, one patient had a complete response, one partial response, four stable disease >12 months, and one progressive disease. In the patients that died during the trial, significant increases in QLI were observed during the first two intervals. Eight patients had stable disease >6 months and two had progressive disease. The overall response rate was 88.23% in these terminally ill (late stage) patients.
Analysis of the peripheral blood leukocytes showed an initial increase in TNF-α followed by a decrease in survivors and a progressive and constant increase in TNF-α levels and an increase in serum levels of sIL-2R in those who died. 35 The mechanisms operating in this clinical study require more investigation, but if it can be repeated, it could be very promising.
Finally, Russian investigators have reported use of PBM in cancer patients, but it is difficult to retrieve details of the studies. 36,37
Conclusions and Unanswered Questions
PBM is becoming a well-established approach to mitigate or prevent the development of cancer therapy associated side effects, especially oral mucositis. The more intriguing question is not merely whether PBM is safe and effective in cancer patients, but whether PBM can play an active role in cancer treatment? There are tantalizing reports that this may indeed be the case, but there are many questions still to be answered. The wide array of different devices and parameters that have been used make this quite a complicated area.
While the biphasic dose–response is accepted in normal tissue, how it applies to malignant tissue is unclear. In some cases, it appears that a very high dose will create a cytotoxic level of ROS that can directly destroy the tumor. In other cases, the main effect of PBM appears to stimulate the immune system, and a low dose may be more effective. If the aim is to stimulate the immune system, then it is best to directly irradiate the tumor or to direct the light to the bone marrow, the lymphatic organs, or even the whole body? What can be concluded is that now is perhaps the time to lose the fear of exacerbating cancer by shining light on it and start to plan well-controlled clinical trials, even if these must necessarily be in advanced patients who have run out of options. There is clearly a great number of new possibilities involving the combination of PBM with other forms of cancer therapy, which may allow us to take advantage of biochemical differences between cancer and normal cells to effectively work against the cancer.
Footnotes
Acknowledgments
M.R.H. was funded by U.S. NIH grant R01AI050875.
Author Disclosure Statement
S.T.N. and J.R.S. are co-owners of JOOVV, Inc., a company selling light therapy devices. M.R.H. is on the scientific advisory board of JOOVV, Inc.